

|
|
|
|
|
||
|
|
|
|
|
||
Disadvantage of Delayed Implant Placement: Failure to Place Implant in the Septum
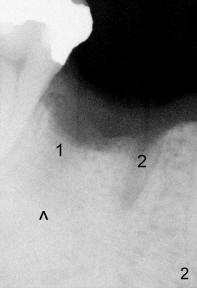
A 41-year-old man presents for #30 extraction for future implant. X-ray shows radiolucency at the furca and the distal apex (Fig.1 arrowheads), severe infection, apparent contraindication for immediate implant. The tooth is extracted using periotome and sectioning without bone graft. To make thing worse, dry socket develops postop. With proper treatment, the wound heals eventually.
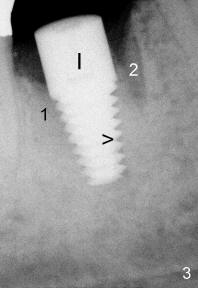
To our pleasant surprise, the distal socket (Fig.2: #1) appears to heal better 3 months after extraction, as the density in socket #1 is higher than that in socket #2. A 6x14 mm implant is apparently placed in the distal socket with combination of osteotomes and drills (Fig.3). In contrast immediate implant allows the surgeon to see the septum with less chance of deviation.
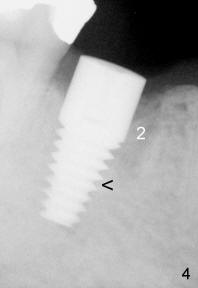
Five months later, bone grows into the threads of the implant (Fig.4: arrowhead), suggesting osteointegration. The density of socket #2 is higher than that in Fig.3.
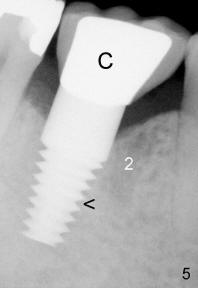
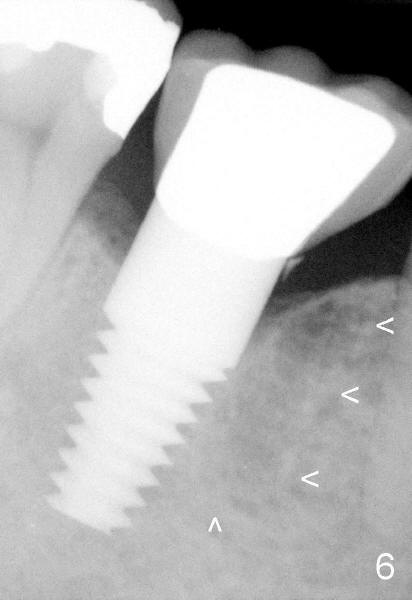
A crown is cemented 2 weeks later (Fig.5: C). Six and one half months post cementation, the patient returns for follow-up. Bone trabecular patterns within the area indicated by arrowheads are consistent with mastication function of the implant (Fig.6). This tooth is so strong that it may contribute to breakdown of an opposing tooth.
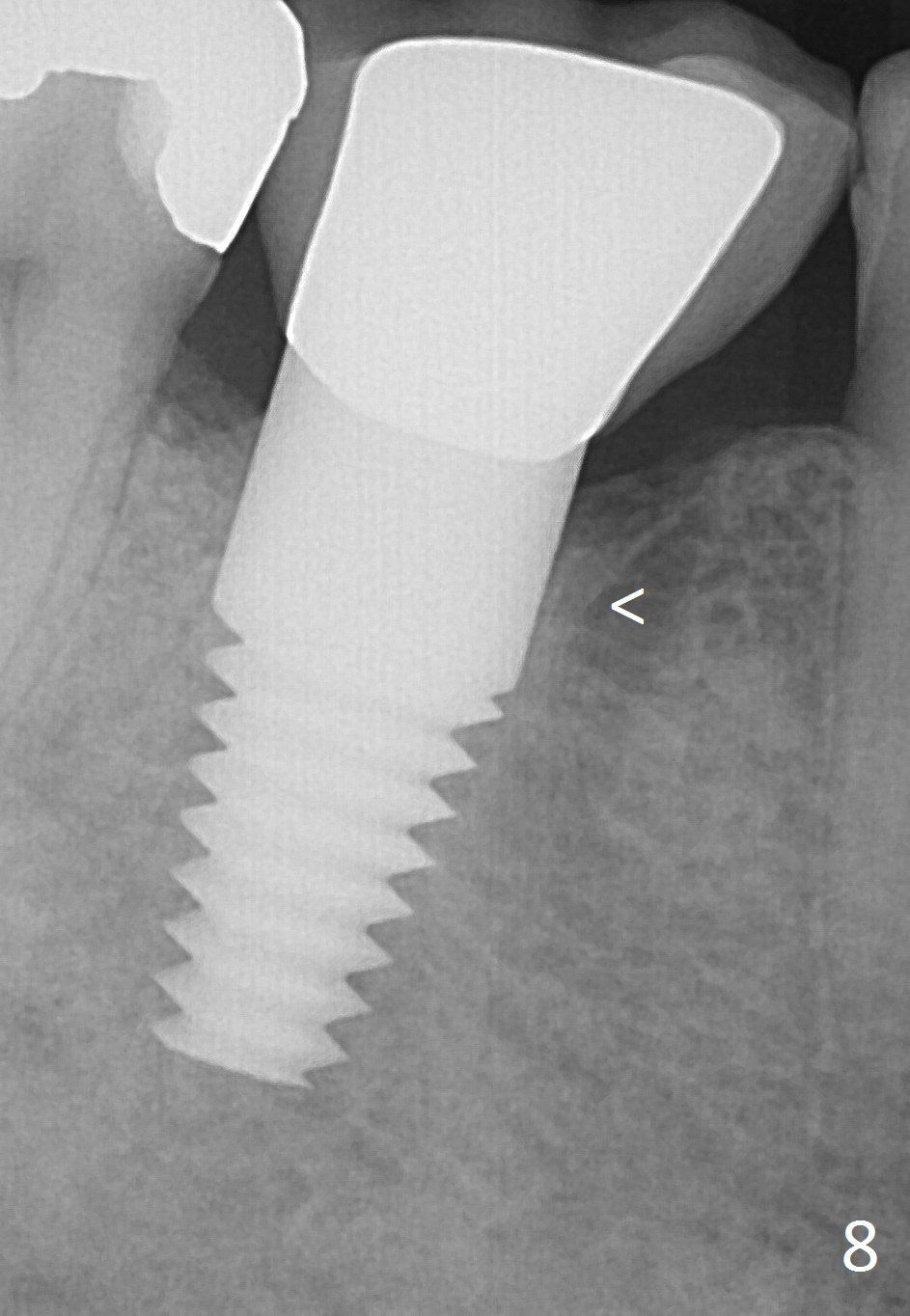
Fig.7 is taken 4 years 10 months post cementation (part of panoramic X-ray), while Fig.8 6 year post cementation with increased bone density.
Return to Follow Up Xin Wei, DDS, PhD, MS 1st edition 05/18/2011, last revision 05/19/2018