









|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
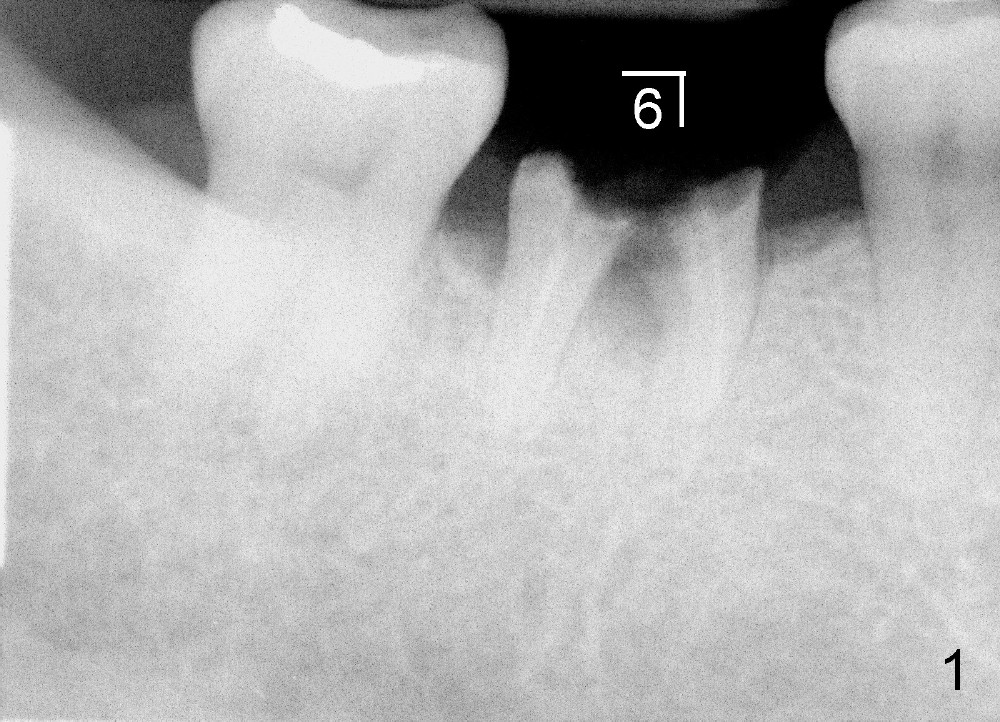
Immediate Implant of Lower First Molar
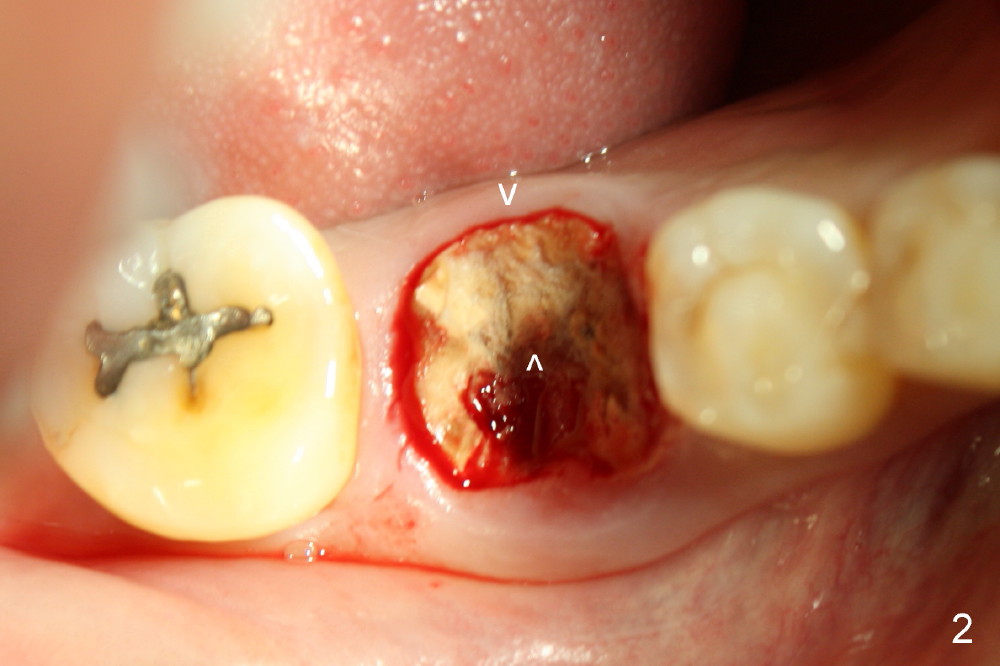
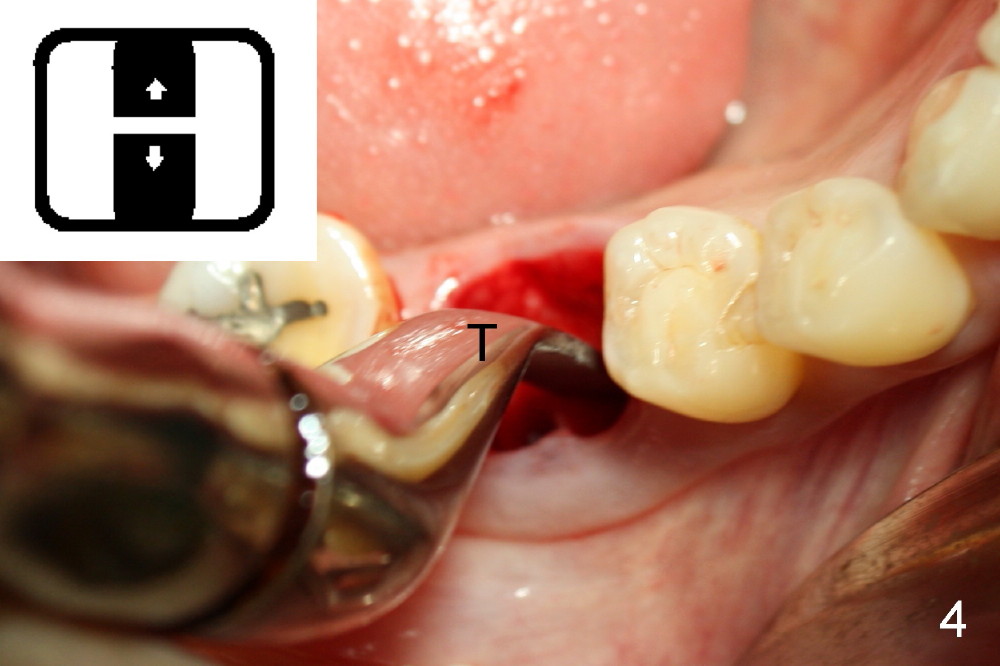
A sixty-year-old lady suddenly fractured the crown of the lower right first molar (Fig.1). The residual roots were sectioned (Fig.2 between arrowheads) and removed. The septum (Fig.3 *) is round on the top between mesial and distal sockets (1,2). Thin osteotomes (SS, SB; Fig.4: T) were used to section the septum mesiodistally. Fig.5 shows the sectioned septum, which makes it easy to insert round osteotomes (RT, Fig.5 inset green; Fig.6 R) without slipping either into the mesial or distal socket.
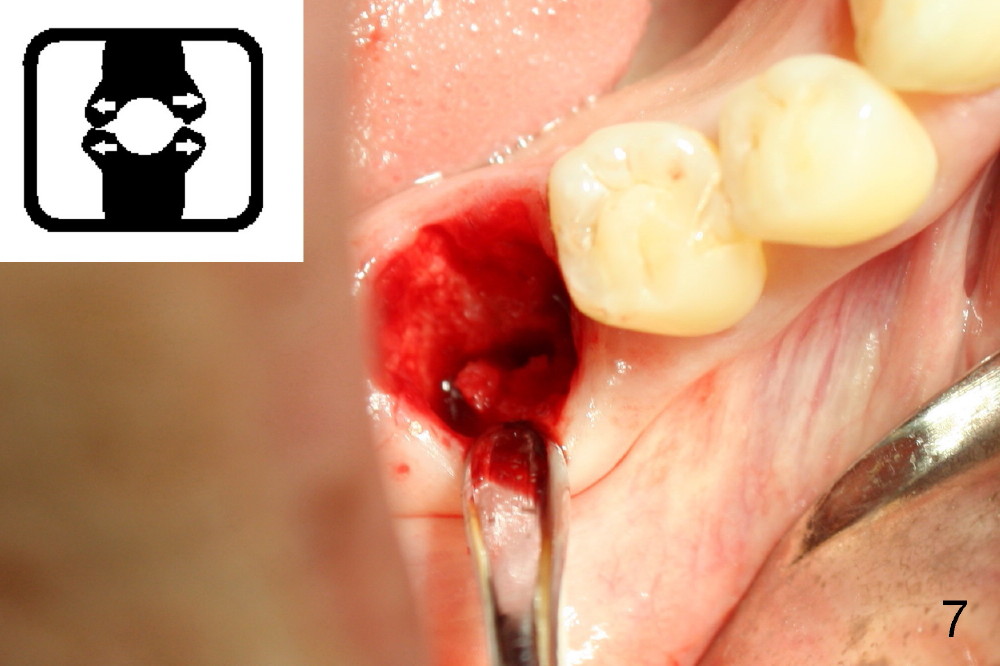
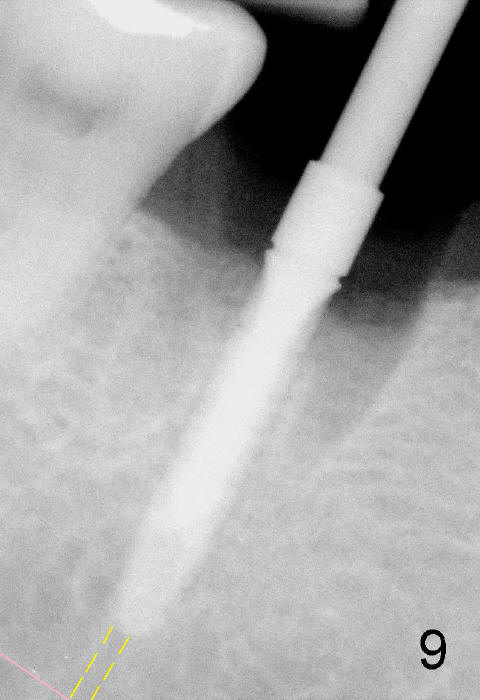
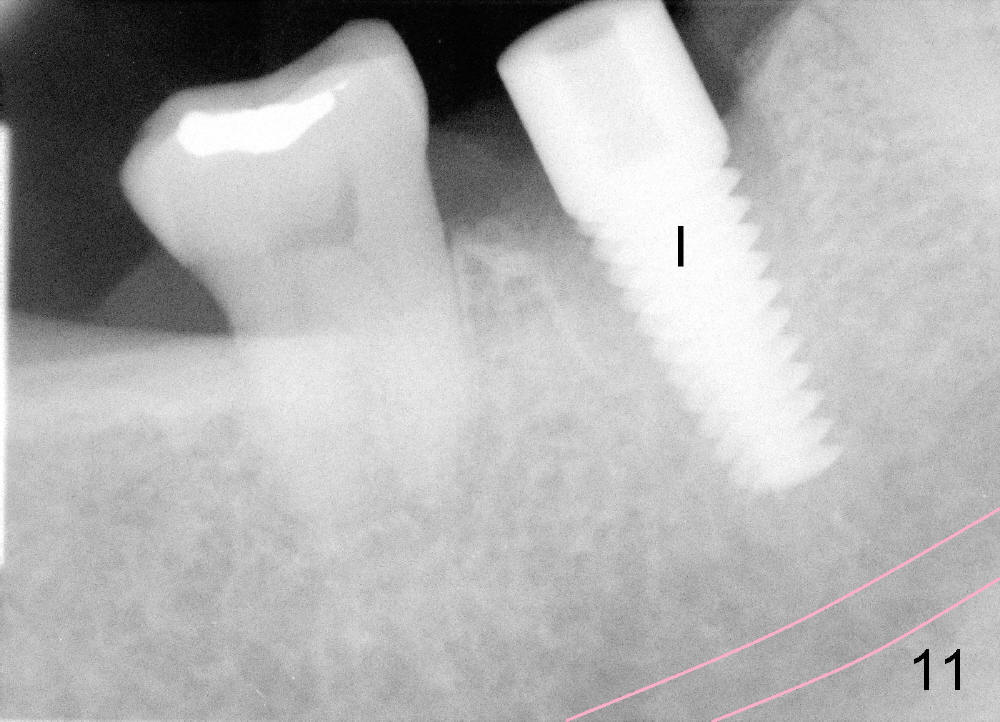
Septal bone is apparently pushed into the mesial and distal sockets (Fig.7 inset arrows) when a small round osteotomes is removed. The deeper portion of osteotomy is created by drills (Fig.8,9). The septal bone is further pushed mesiodistally as the osteotomy enlarges with combination of drills and osteotomes (Fig.10). A 6x17 mm tapered implant is placed with insertion torque >60 Ncm (Fig.11: I).
Fig.12 is taken 1 week post implantation with formation of fresh granulation tissue mesially (<).
There is no atrophy of the buccal plate 2 months postop (Fig.13).
The implant is stable with sign of apparent bone growth around it 4.5 months postop (Fig.14). There is painless localized gingival erythema and edema (Fig.15 <). The infection is most likely from a fistula of #9 (perio-endo disease, after perio surgery and RCT). Without too much thought, an unipost has been cemented, gingival retraction cord (*) inserted and impression taken.
The infection is treated surgically. Nine months post-implantation, there is minimal buccal plate resorption (Fig.16 follow arrowheads). This is the most important reason of immediate implantation.
Xin Wei, DDS, PhD, MS 1st edition 03/18/2013, last revision 12/16/2013