

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
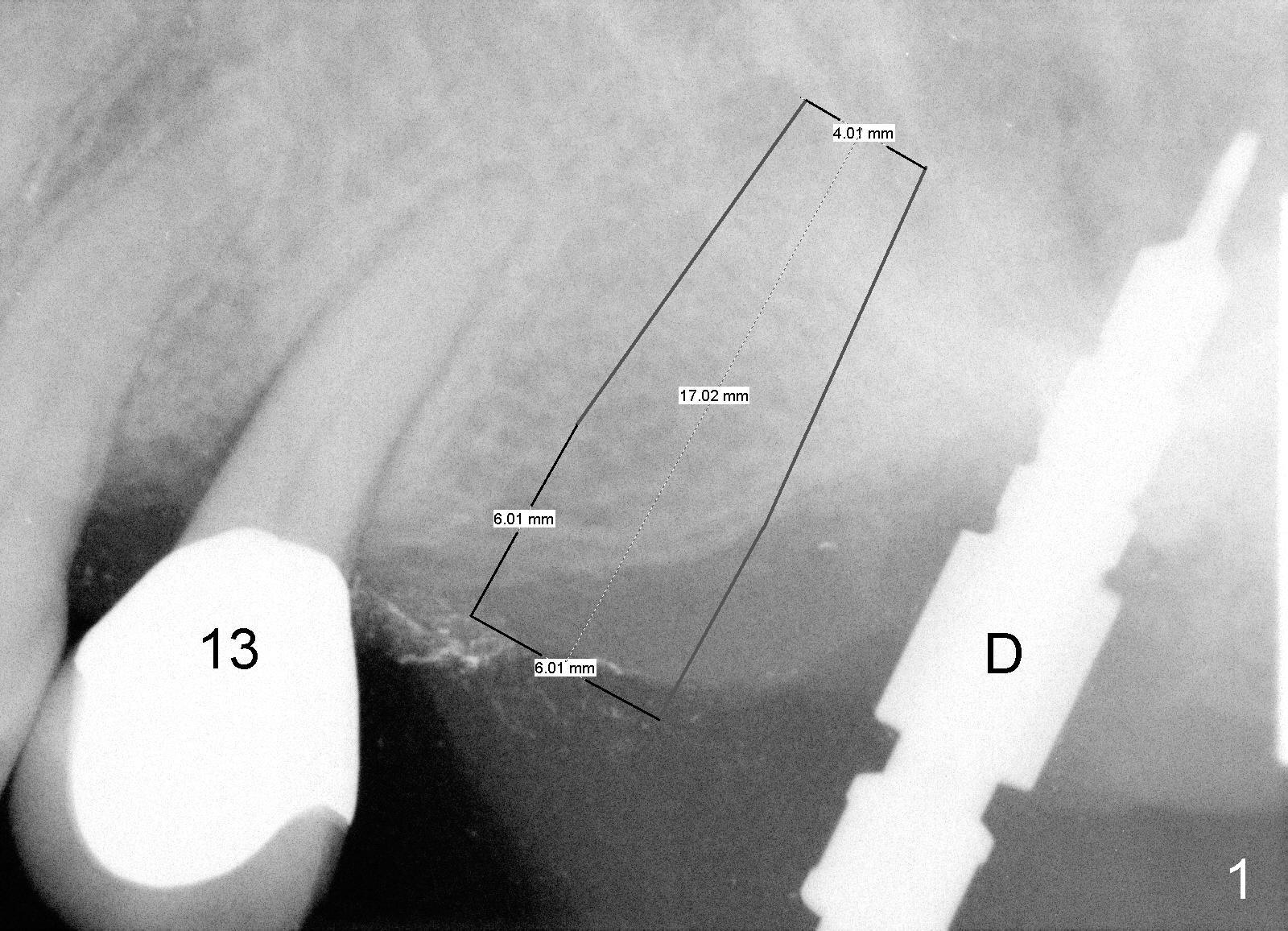
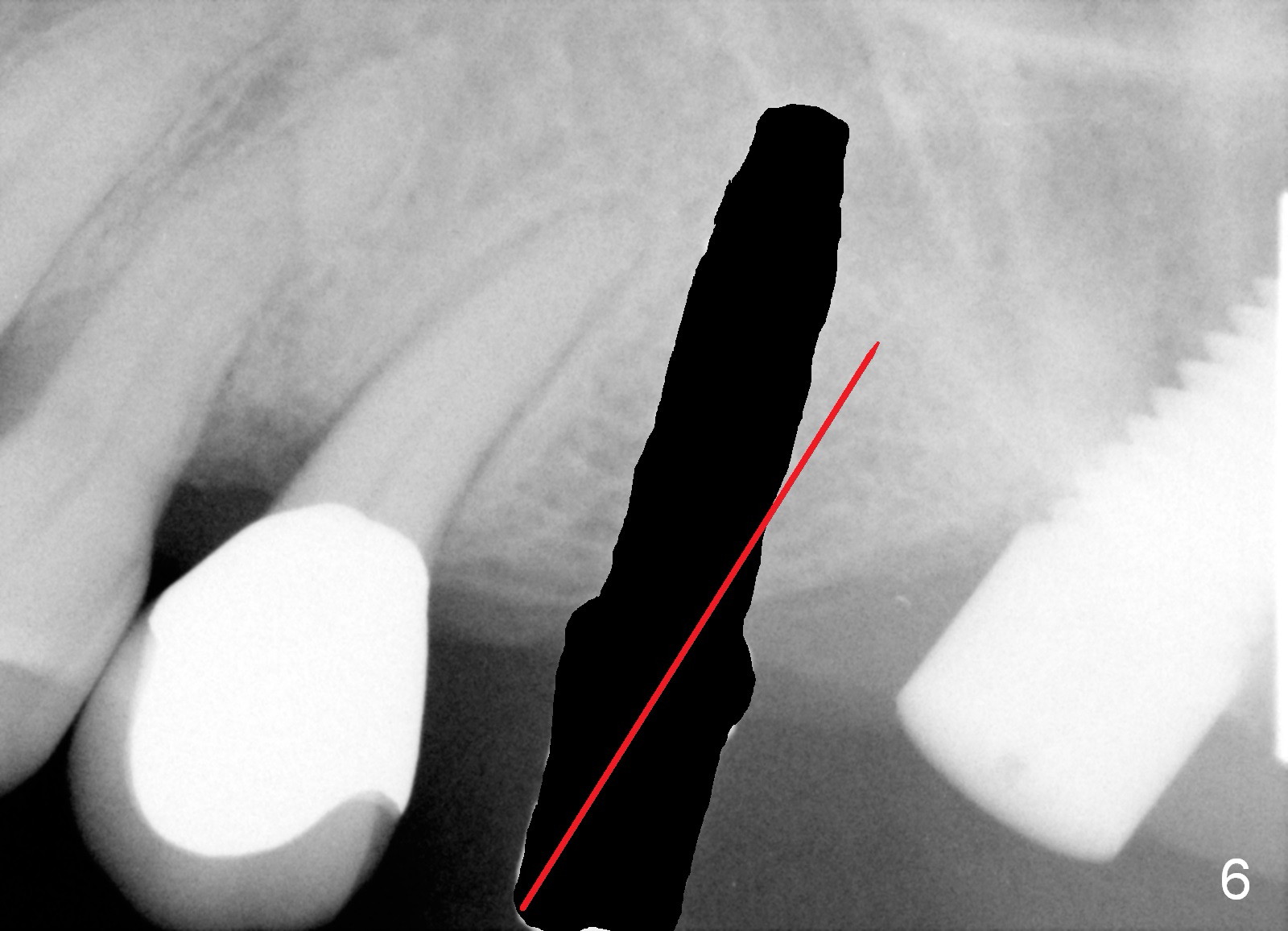
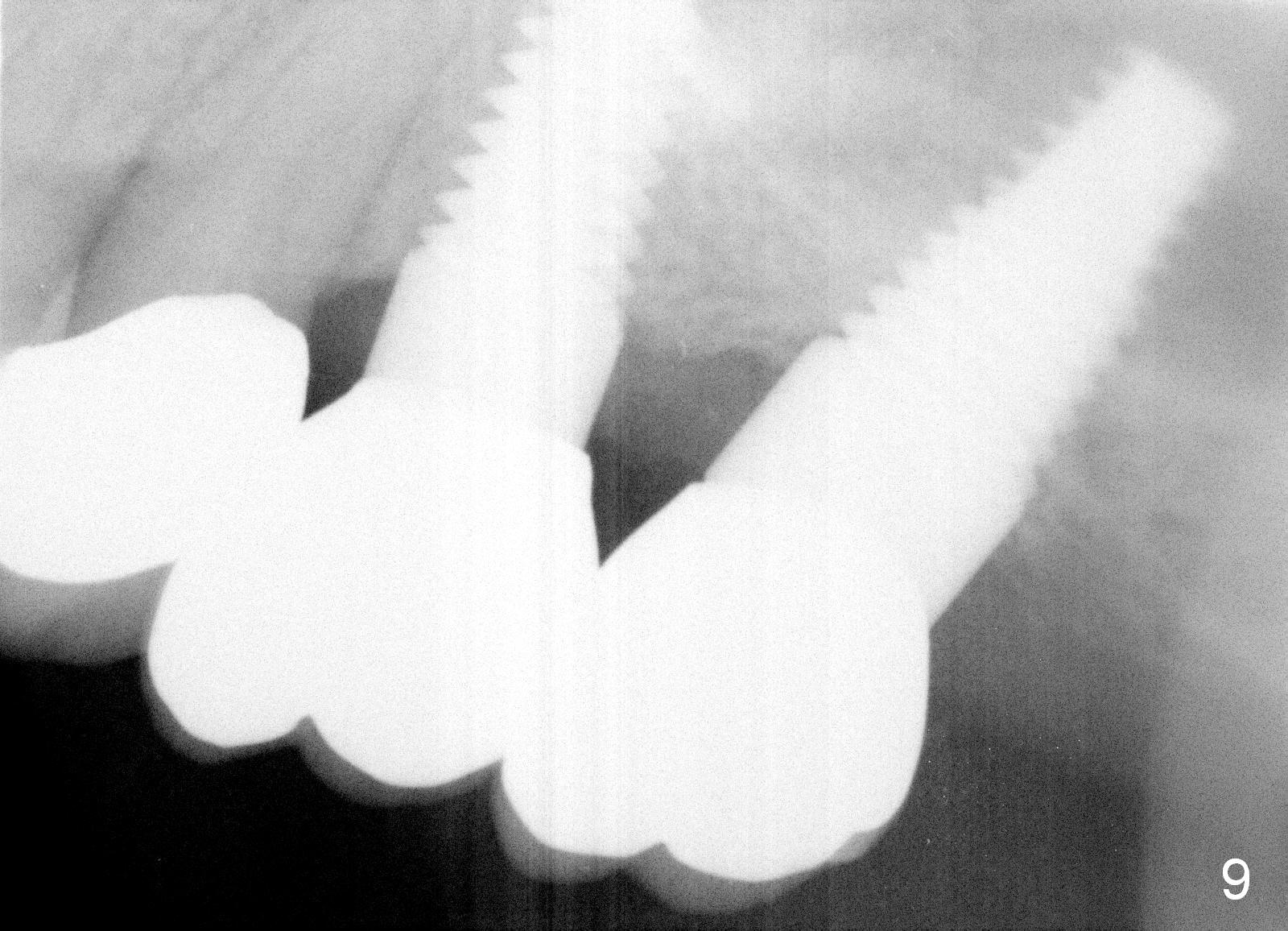
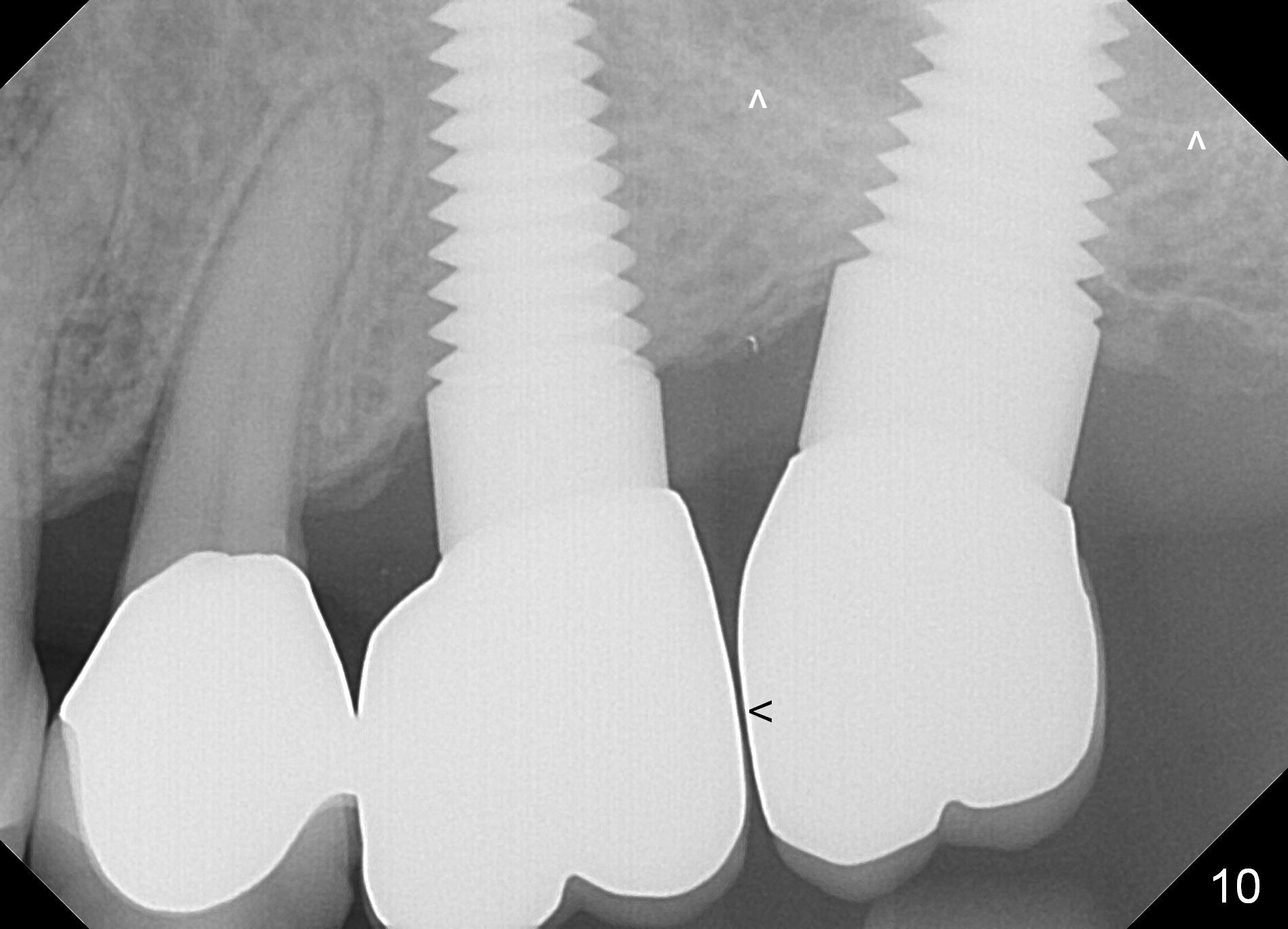
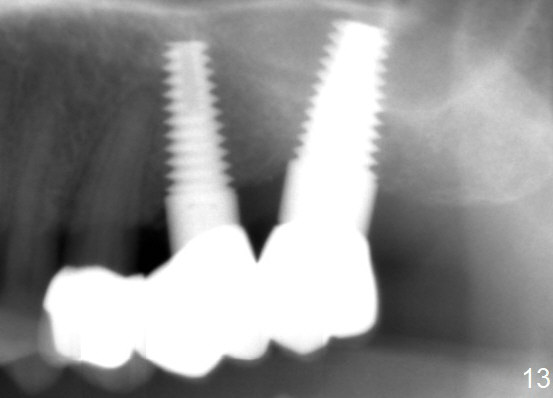
How to Change Trajectory of Non-immediate Implant
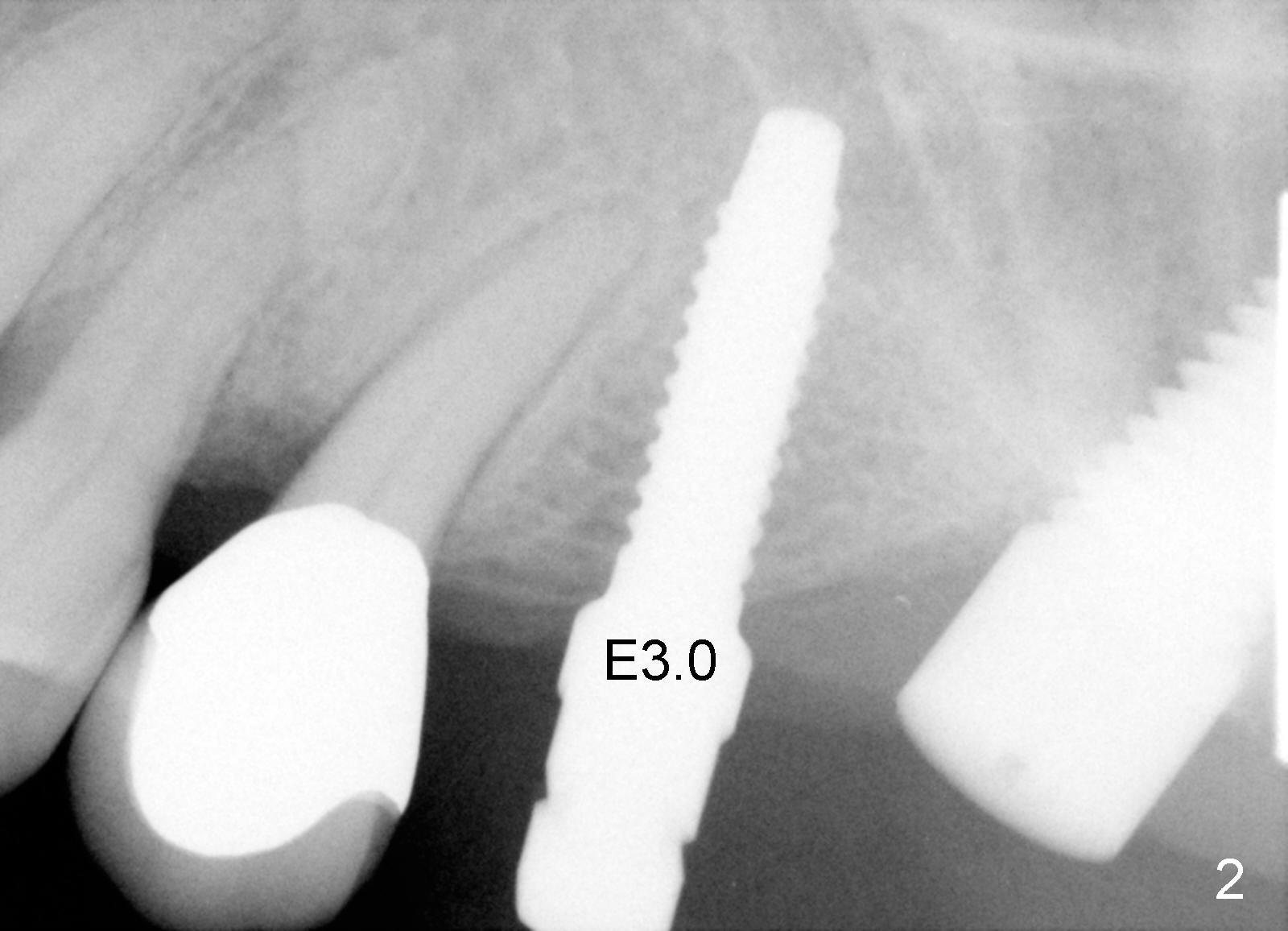
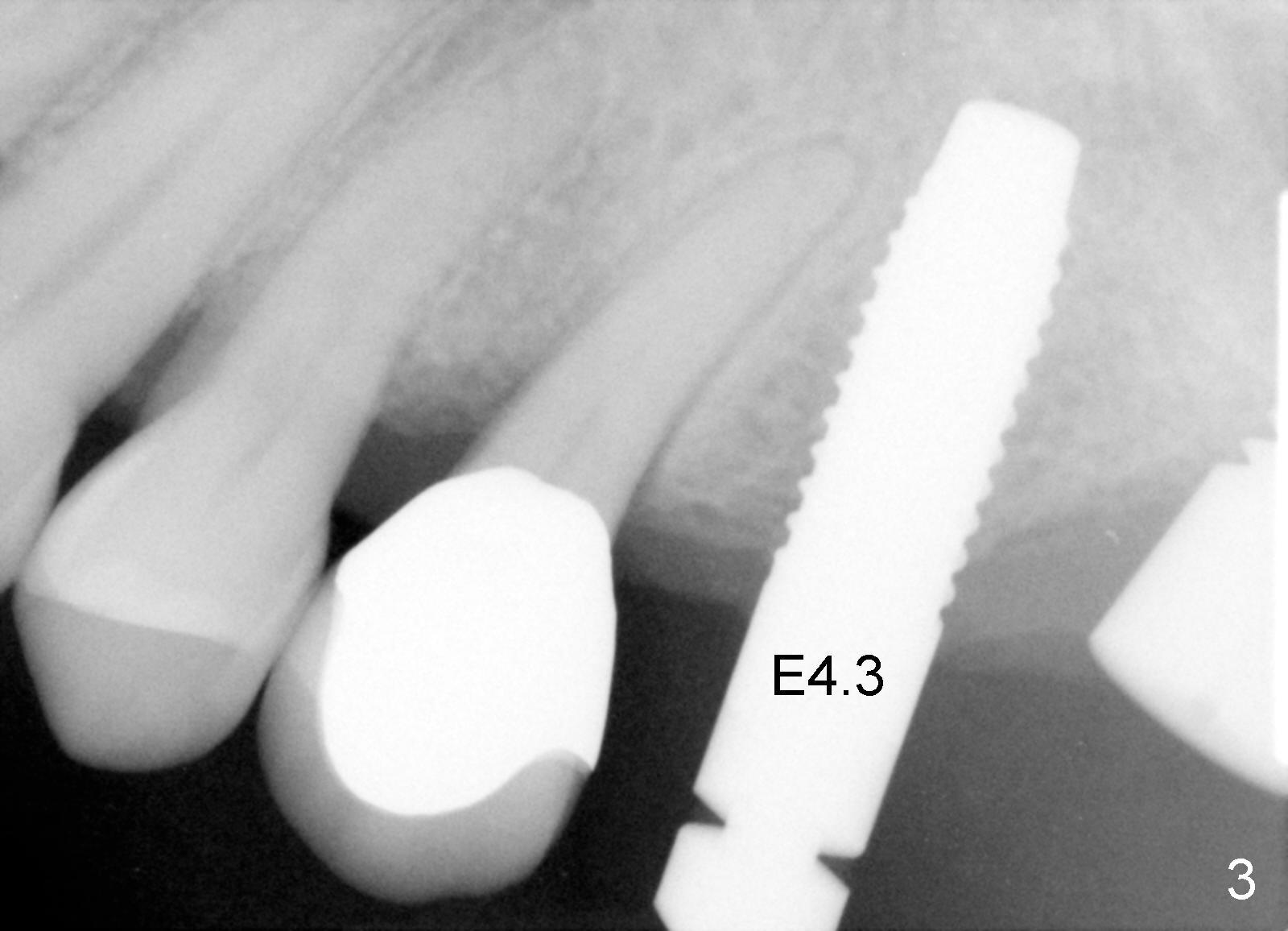
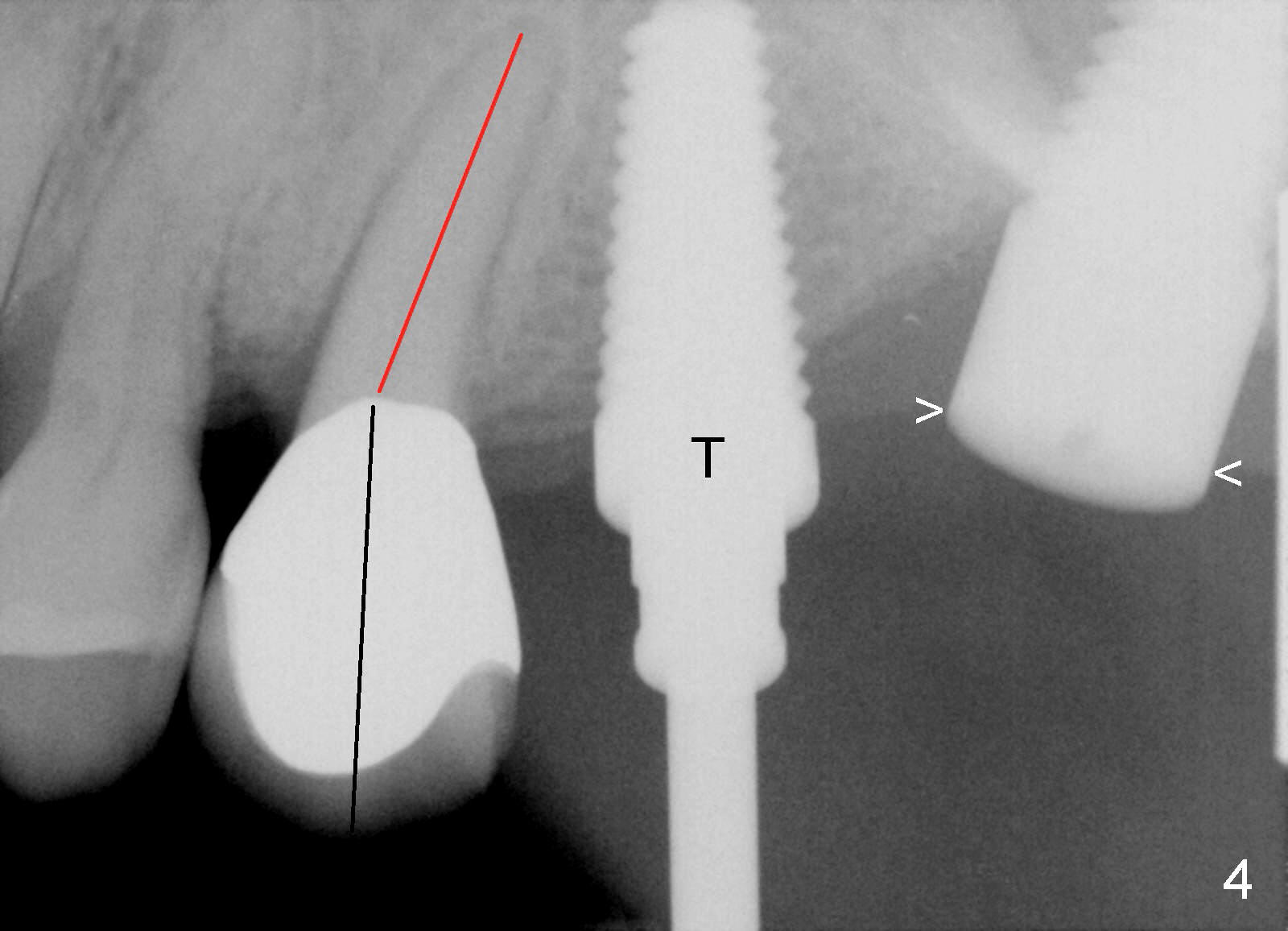
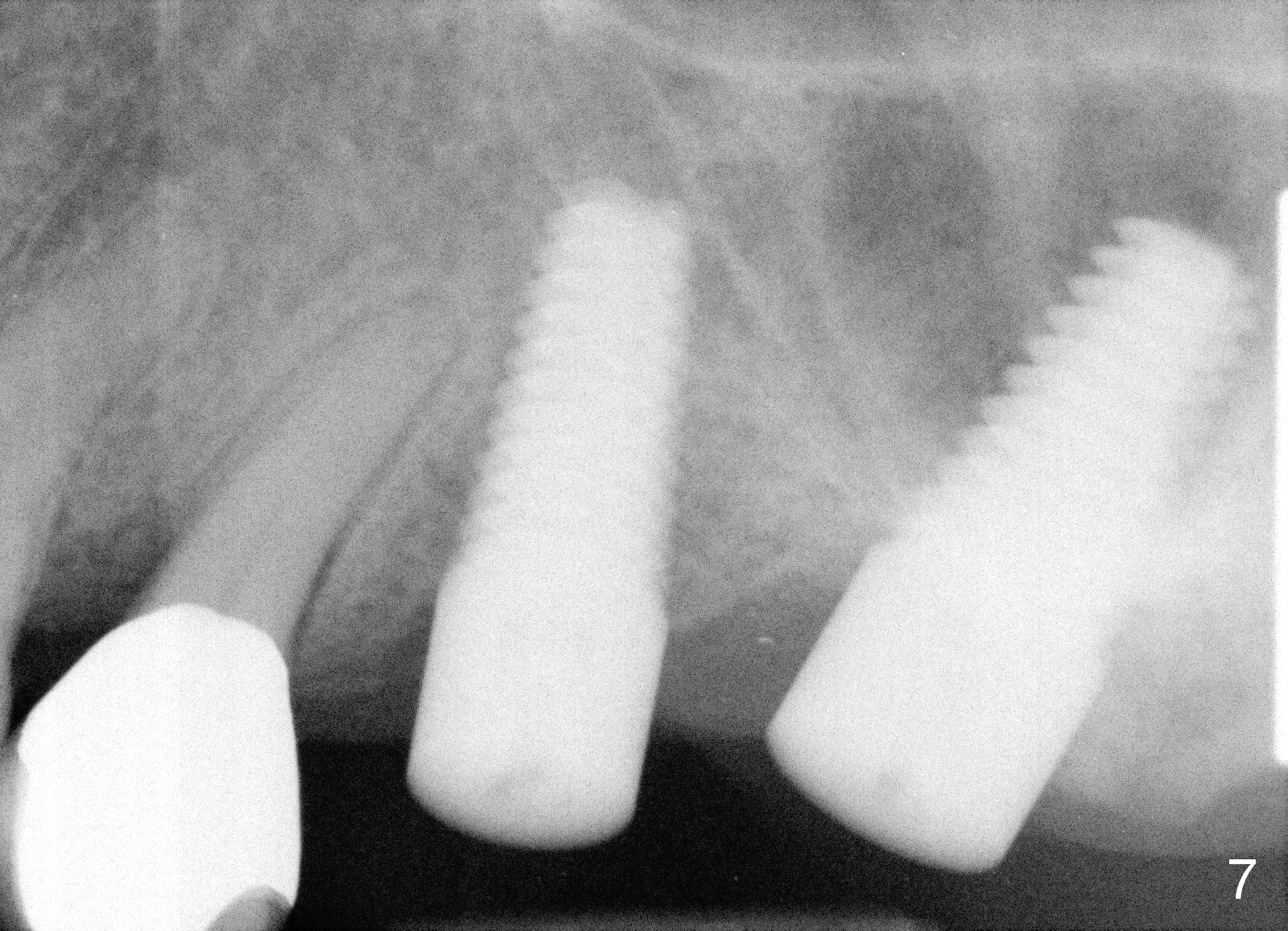
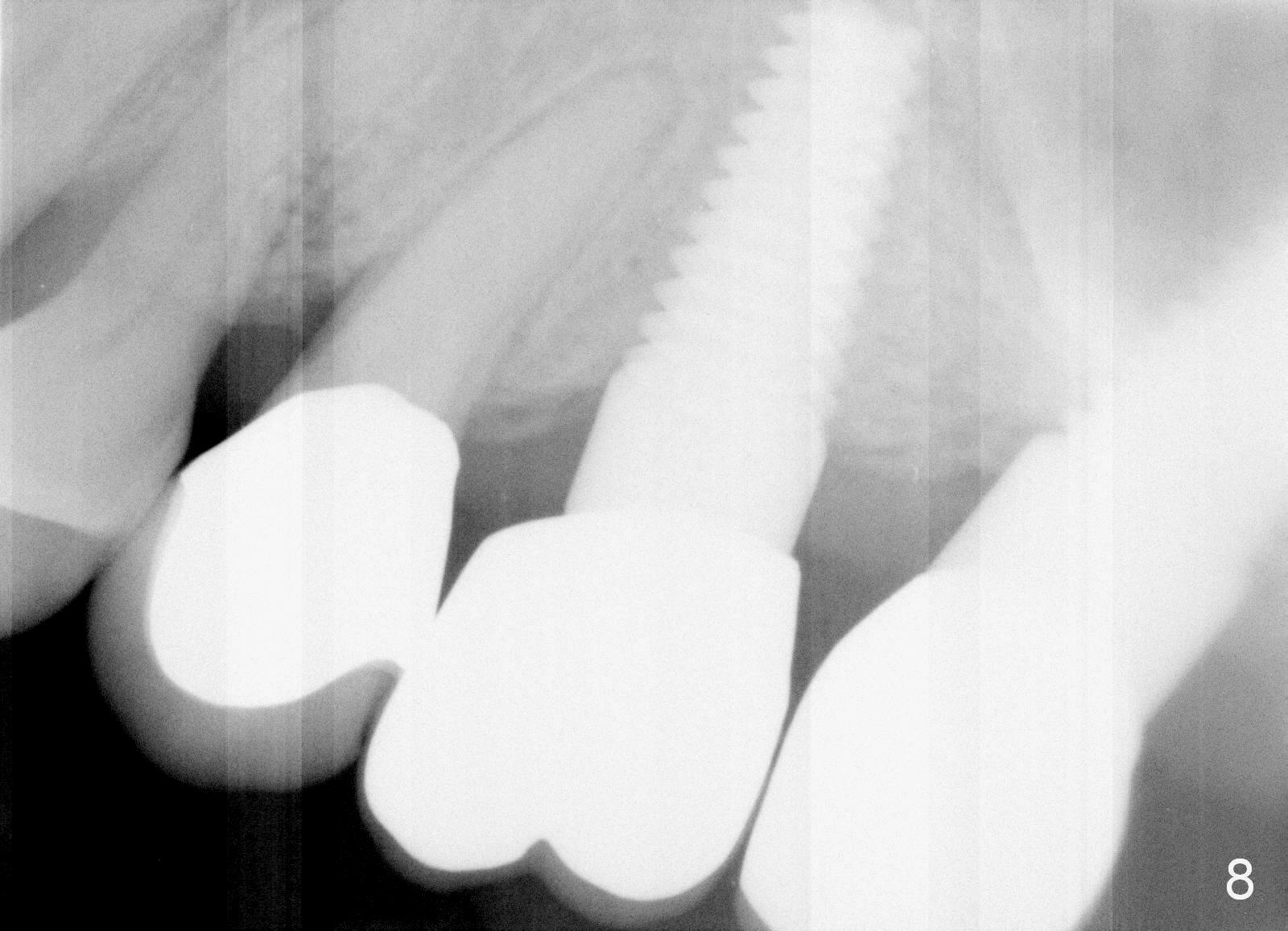
A 58-year-old man used to have a upper left 3-unit bridge. Two months after extraction and immediate implant at the site of the posterior abutment, an implant is planned to be placed at the site of the pontic, #14 (Fig.1). Osteotomy starts with a 1.6 mm pilot drill, followed by bone expanders, parallel to the crown of the tooth #13. The first intraop PA shows that 3.0 mm bone expander is close to the root of the neighboring tooth (Fig.2). No matter what is done to change the trajectory of the osteotomy using expanders according to the crown morphology of the neighboring tooth, the next 3 expander does not improve in parallelism (Fig.3). When a 6x17 mm tap is inserted (Fig.4 T), it is realized that axis of the tap is parallel to the axis of the crown of the neighboring tooth (black line), but not that of the root (red line). It is too late to change the trajectory drastically; a 6x17 mm implant is placed with insertion torque > 60 Ncm (Fig.5). It is best to change the trajectory as early as possible, e.g., after taking the first intraop PA and withdrawing the expander (Fig.6 black area) and as much as possible (red line; starting new osteotomy). It is quite similar to immediate implant. There is no bone loss 2 months postop (Fig.7), 18 months (Fig.8,9) or 34 months (Fig.10)post cementation, in spite of open contact between the crowns (Fig.10 black arrowhead). This is partially due to supragingival margin (Fig.11,12 (immediately pre-cementation)). No bone loss is noted 3 years 5 months post cementation (Fig.13).
In contrast, the trajectory of an immediate implant could be changed almost anytime and much easier. An immediate implant is always larger than non-immediate one at similar sites.
Return to
Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 07/19/2015, last revision 08/04/2017