

.jpg)
.jpg)
2)%20abutment.jpg)



|
|
|
|
|
||
|
|
|
|
|
||
|
|
|
|
|||
Implant Placement Level
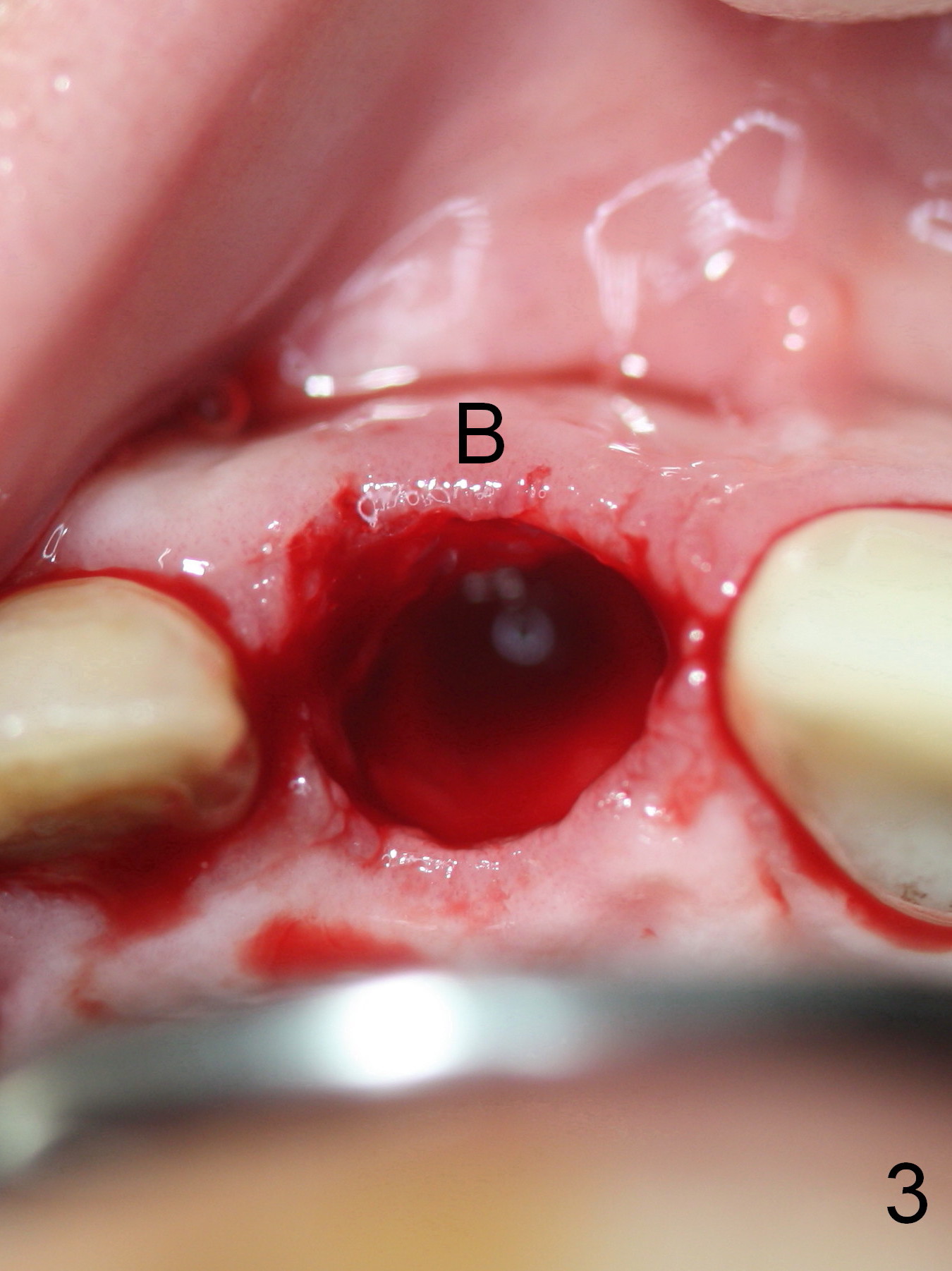
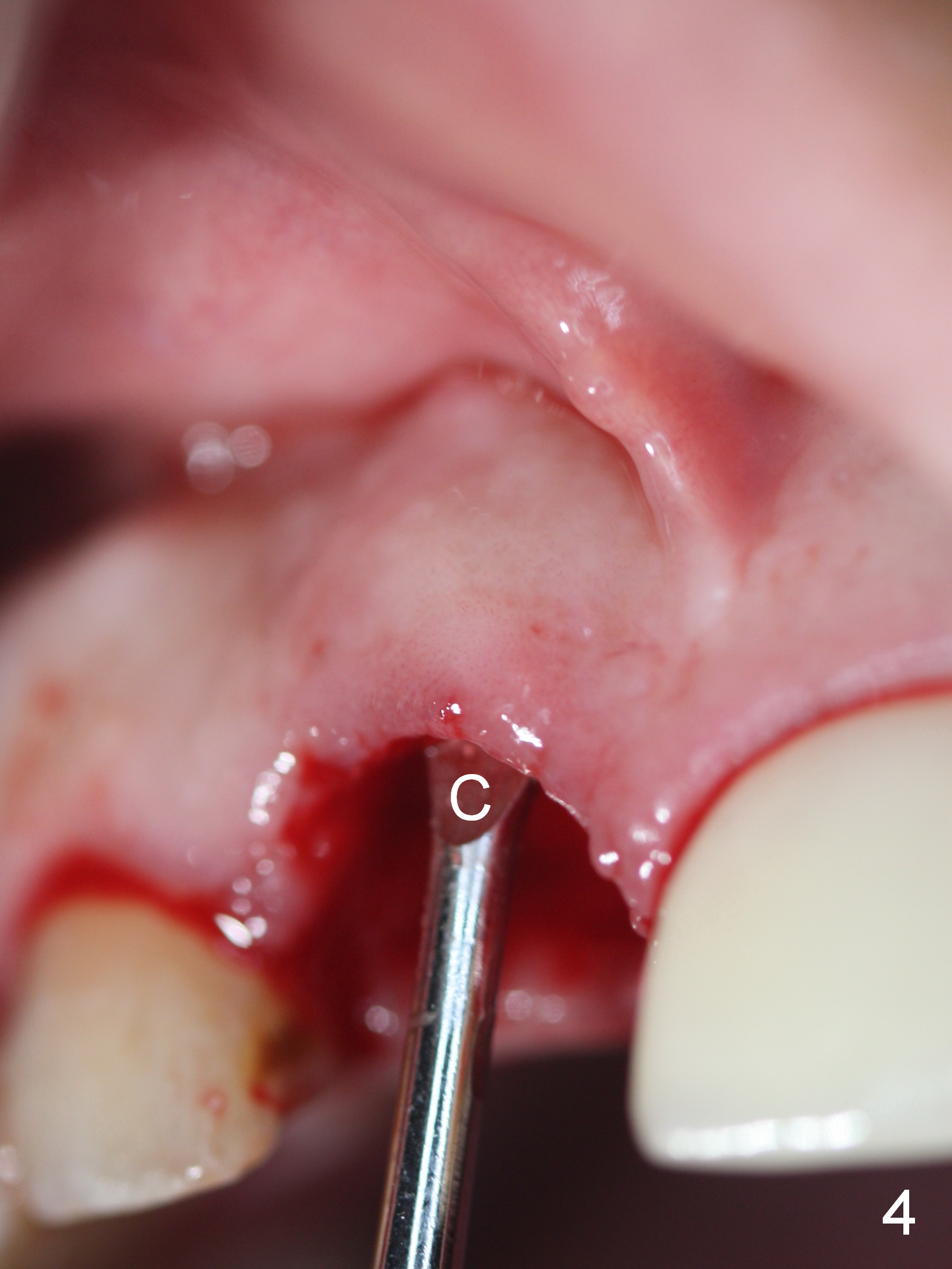
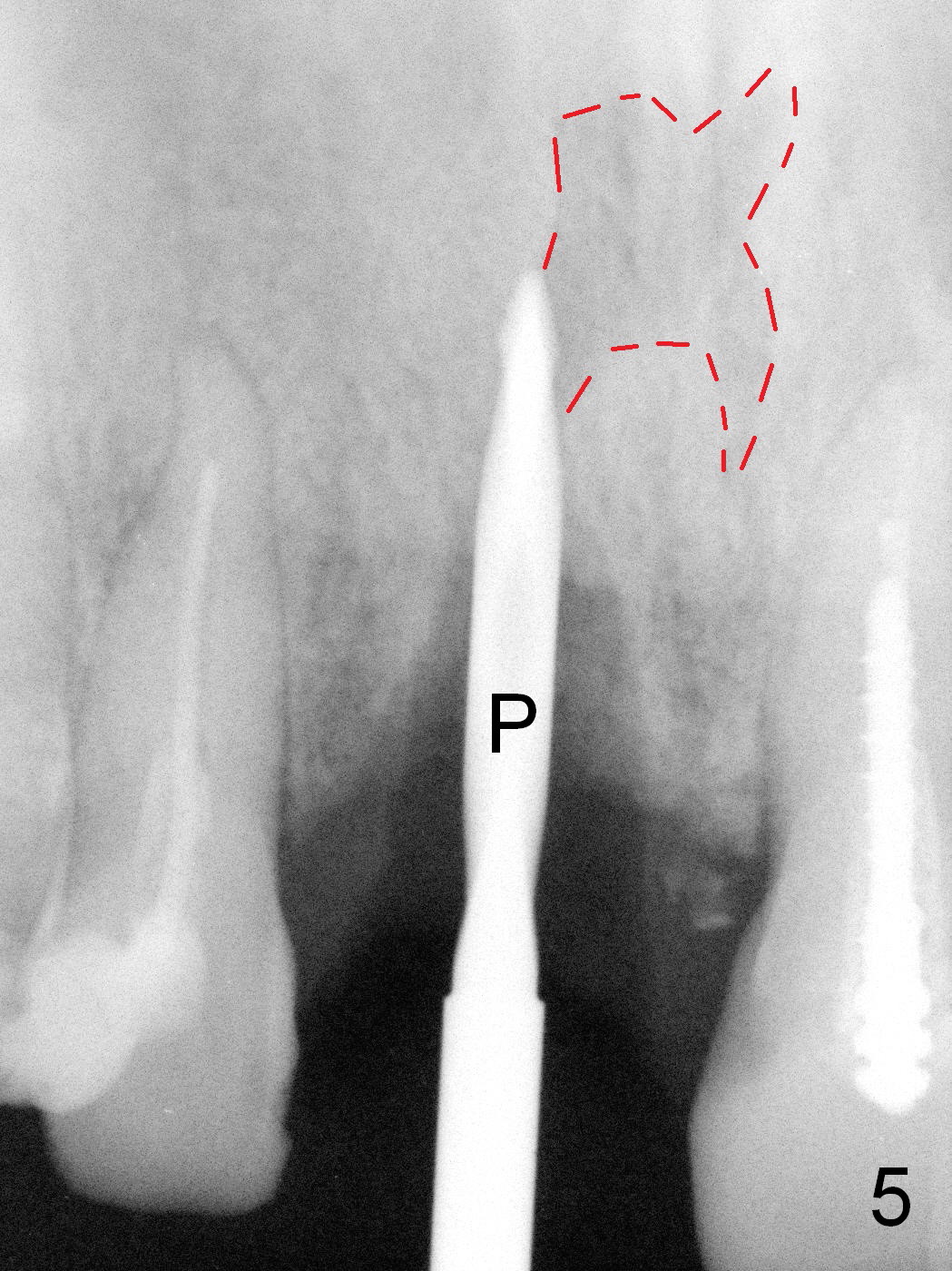
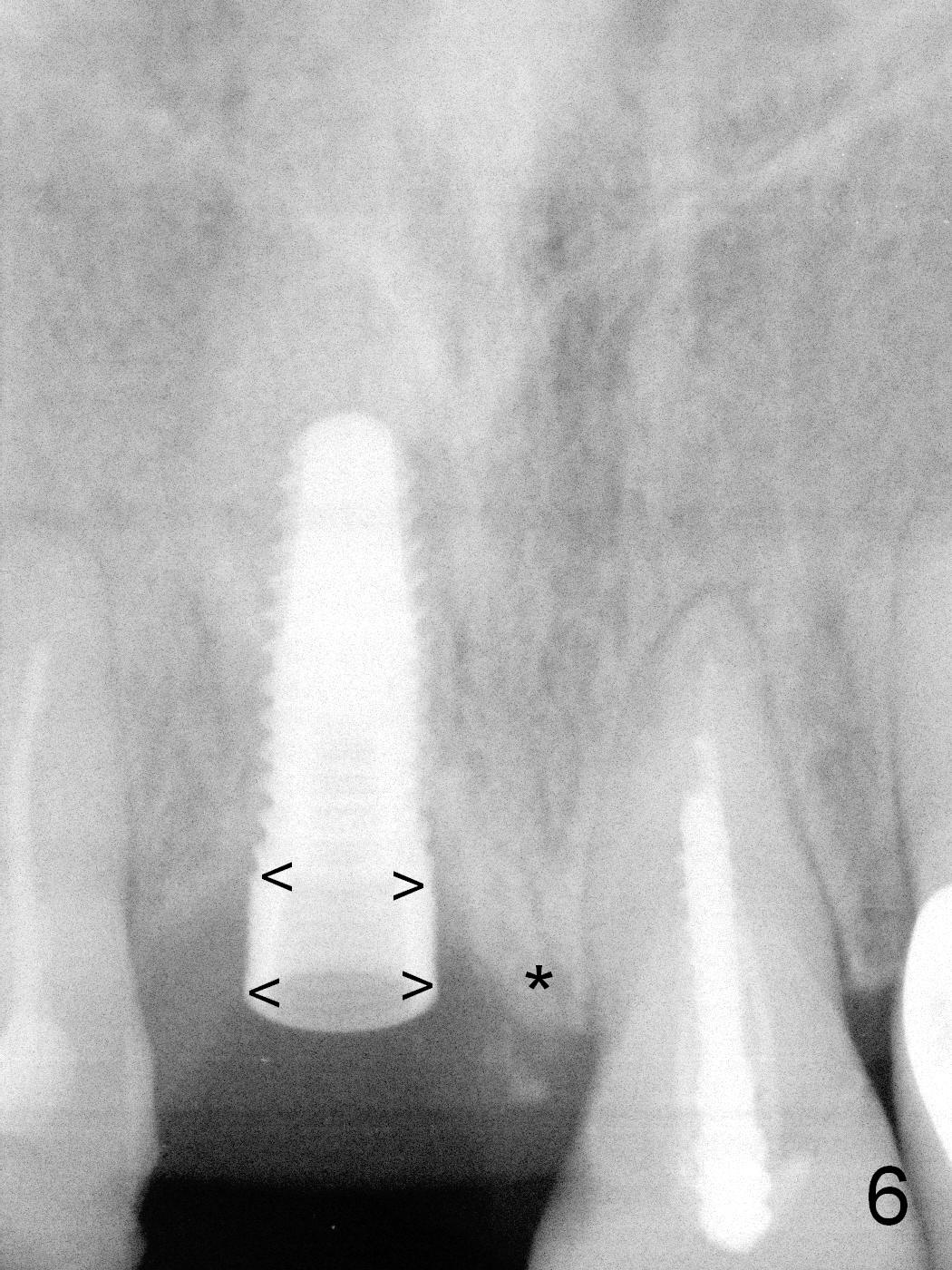
When the patient returns for #8 extraction and immediate implant, there is periradicular infection (Fig.1 <), associated with root fracture (Fig.2). Although there is no buccal collapse after extraction (Fig.3 B), the labial plate is defective (Fig.4 (C: currette)). The tip of the 2 mm pilot drill (Fig.5 P) is close to the Incisive Canal (red dashed line). After adjustment of the osteotomy trajectory, the plateau of a 4.5x14 mm bone-level implant is placed at the mesial crest level (Fig.6 *); the most coronal microthreads of the implant are not covered by the native bone mesiodistally (arrowheads), but by bone graft (Fig.7 *, mineralized cortical and cancellous allograft and Osteogen). The implant plateau is 1-2 mm apical to the CEJ of the neighboring tooth (Fig.7 >). A 5.8x4(3) mm abutment (A) is placed immediately for an immediate provisional. The abutment also helps keep the graft in place. The graft is also placed buccally to repair the buccal plate defect.
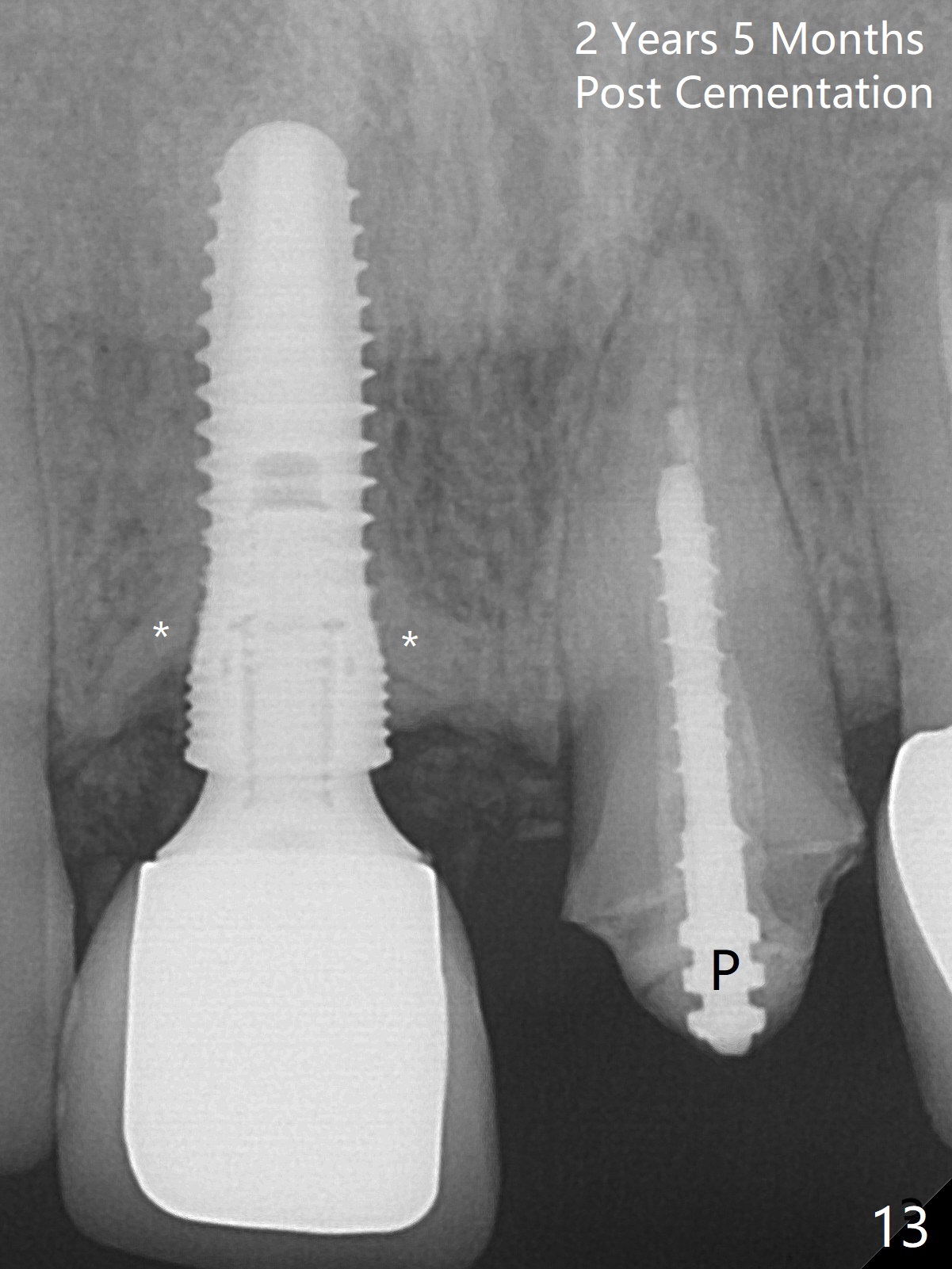
The patient returns for final restoration 3 months 11 days postop. The density of bone graft appears to be reduced (Fig.8, as compared to Fig.7). There is no periapical infection (Fig.9 >, compare to Fig.1). Due to change in the gingival margin and easy dislodgement of the provisional, a longer abutment with a shorter cuff (5.8x5.5(2) mm) is used prior to impression and shade selection (Fig.10,11). One month post cementation, the buccal plate over the implant crown looks non collapsed (Fig.12 *). There is dense bone formation at the coronal end of the implant 2 years 5 months post cementation (Fig.13 *) with the normal soft tissue.
Return to
Upper Incisor Immediate Implant,
Technicians,
4,
9,12,31
9 crown
Xin Wei, DDS, PhD, MS 1st edition 10/24/2015, last revision 08/23/2020