

,%20before%202nd%20step%20of%20grafting.jpg)







|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
|
|
|
|
|
|
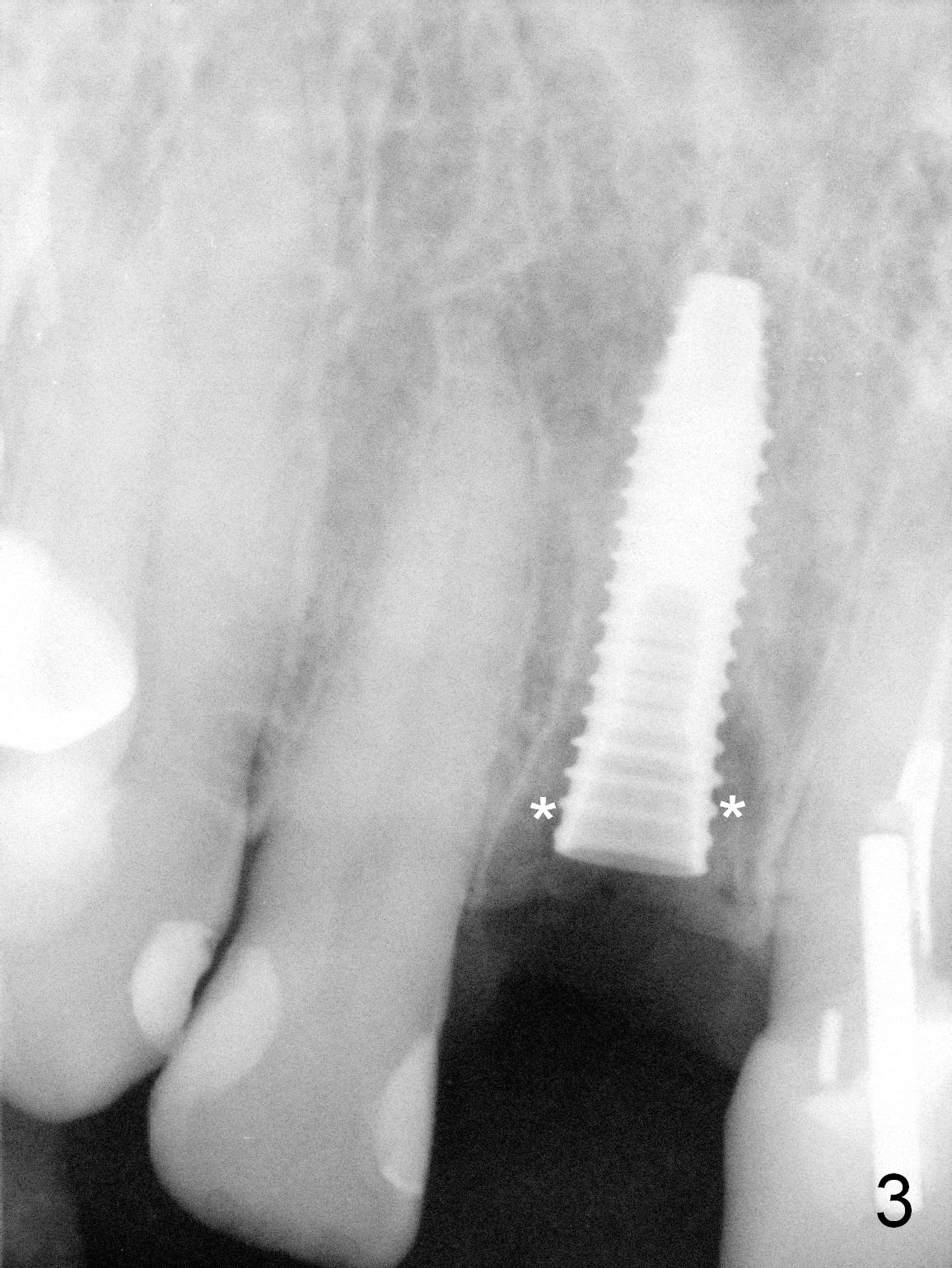
Fig.1 shows equigingival tooth fracture with that of the fiber post (*). There is buccal or palatal plate defect after extraction. Osteotomy is initiated in the palatal slope, with 3.2x18 mm drill in place (Fig.2, gingival level). Then a 4x15 mm bone-level implant is placed as palatal as possible with ~ 35 Ncm (Fig.3). After further placement of the implant, a straight abutment (4.5x5(3) mm) is placed (Fig.4); peri-implant space (Fig.3 *) has been closed with allograft and Osteogen. An immediate provisional is fabricated using a crown form, instead of the hollow porcelain crown. In fact the latter should have been done for better morphology.
When the palatal wall is defective with a smaller socket, the osteotomy tends to be placed more buccally; there is higher chance to use an angled abutment.
Since the repeated failure of the anterior restoration, an implant is to be placed at the site of #2 for posterior support.
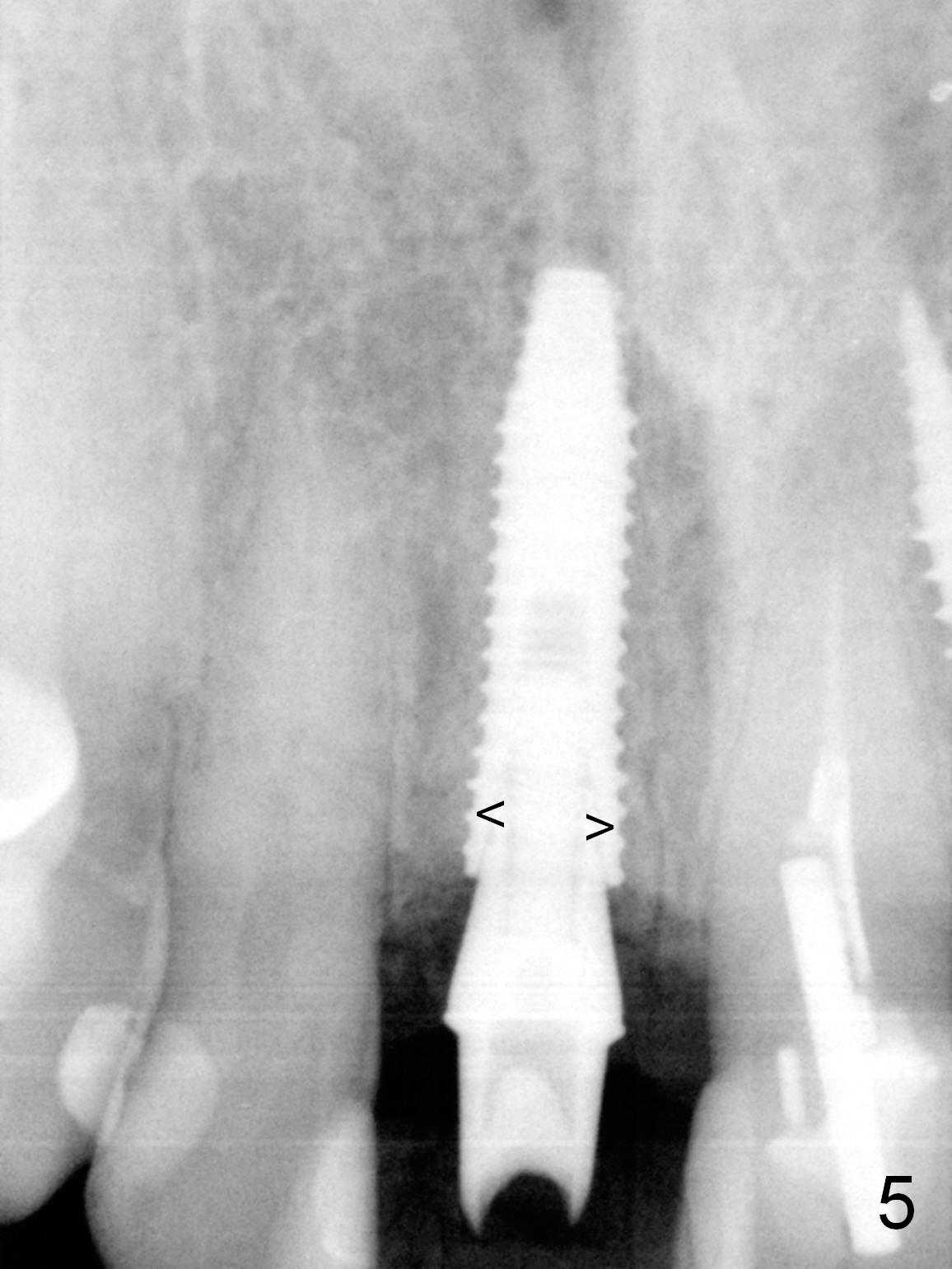
Peri-implant gaps appear to remain to be closed by bone 3.5 months postop (Fig.5 arrowheads). The existing crown (Fig.6,8 C, sent to lab) seems to be able to cover the metal abutment in shade (Fig.7,9). Use of the same material and shades A1 (body and incisal edge) and A2 (gingiva, Fig.10,11) should be capable of achieving cosmetic results.
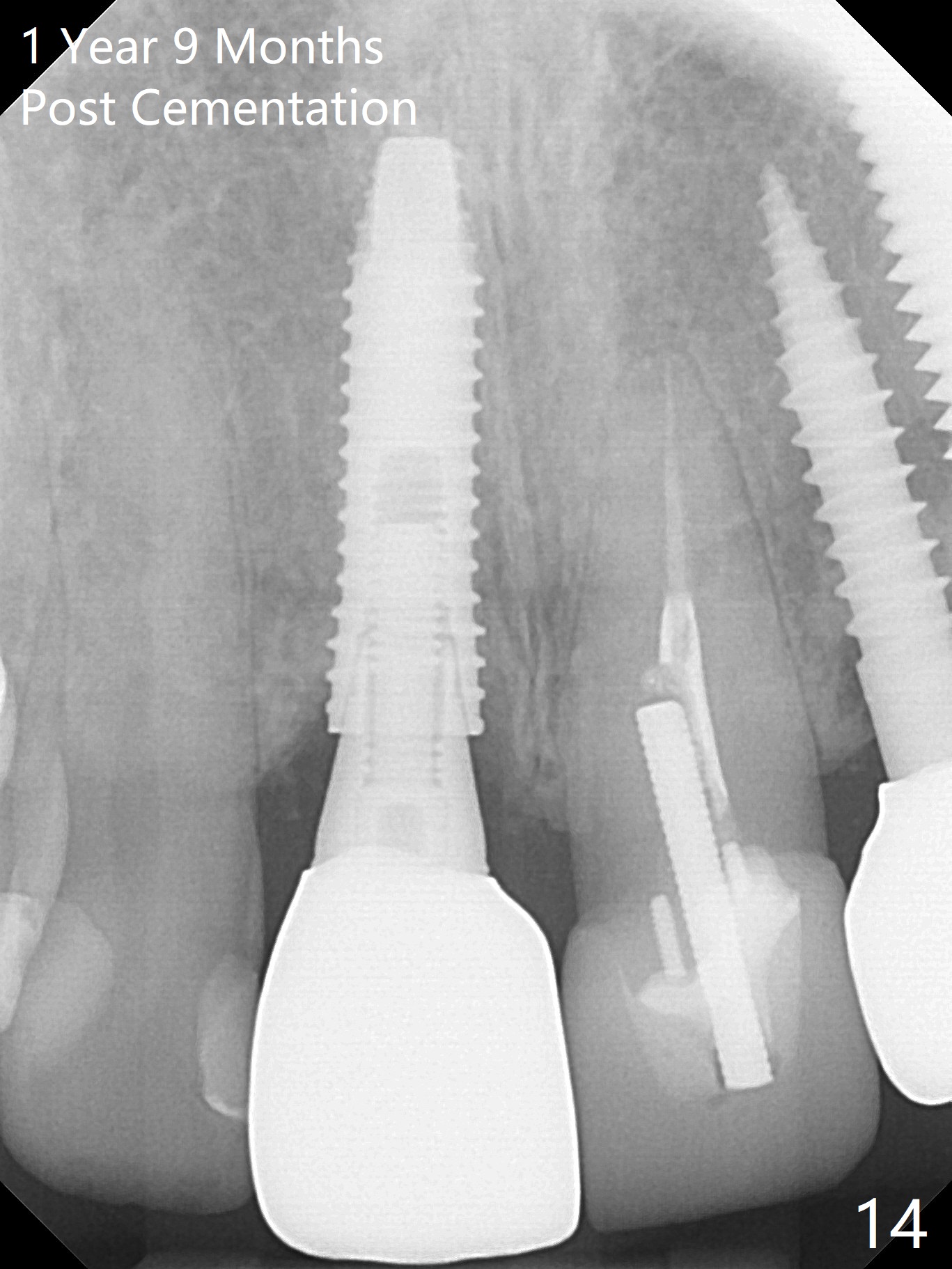
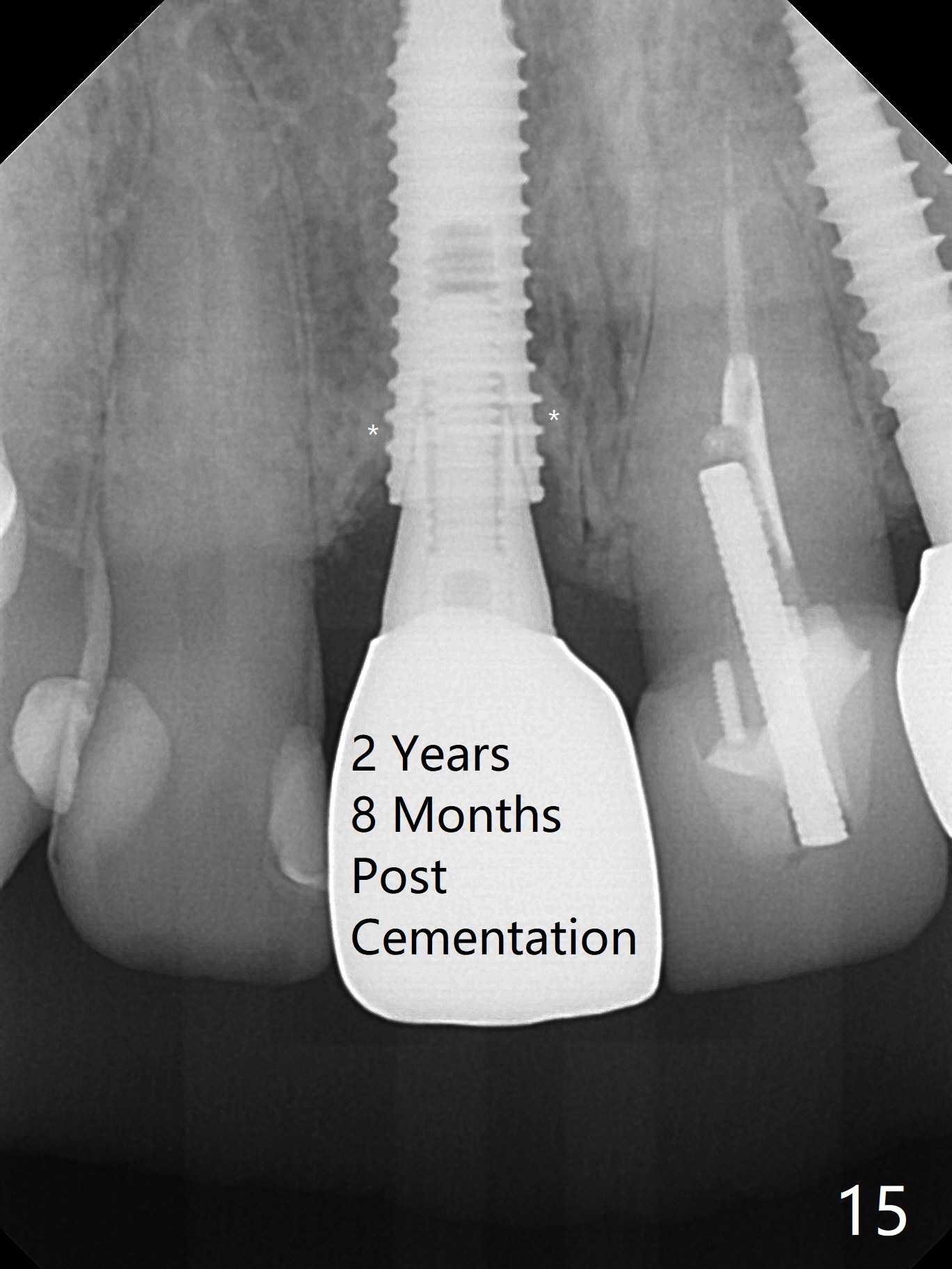
The crown chips distoincisally 4 months post cementation (Fig.12). When remaking the crown, pay attention to the opposing tooth with the prominent distoincisal edge (Fig.7). Please choose an appropriate material. I do not remember which crown we cemented last time: Emax or Generic Zirconia. Please study the existing crown (attached in the case). The patient likes the original shade, although it does not match that of the neighboring teeth. There is minimal bone loss 1 year 8 months post cementation (Fig.13,14). The bone density around the most coronal threads increases 2 years 8 months post cementation (Fig.15 *).
Return to Upper Incisor Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 04/25/2016, last revision 05/25/2019