


,%204.8x5(3).jpg)




,%205(2).jpg)

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|||
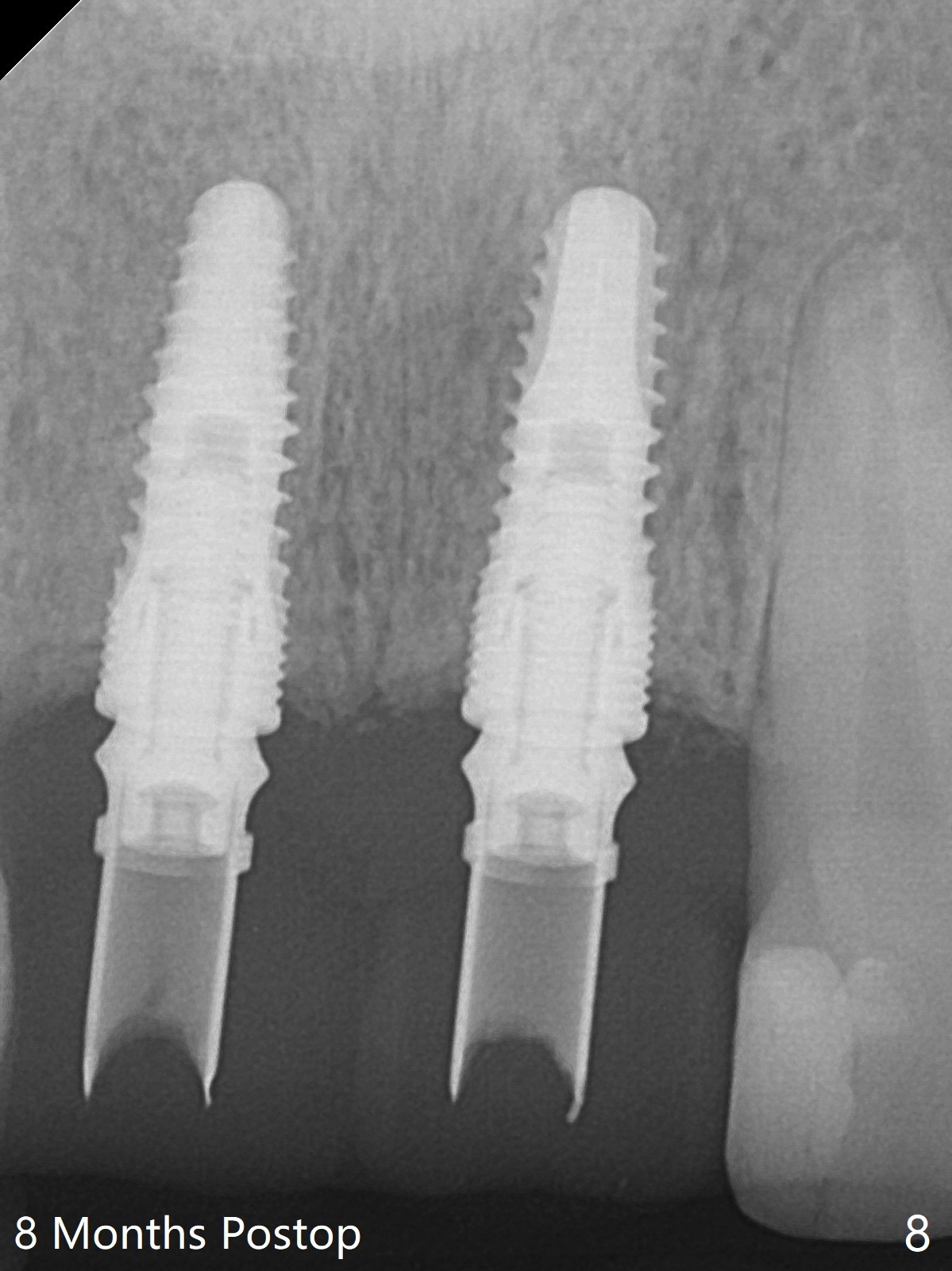
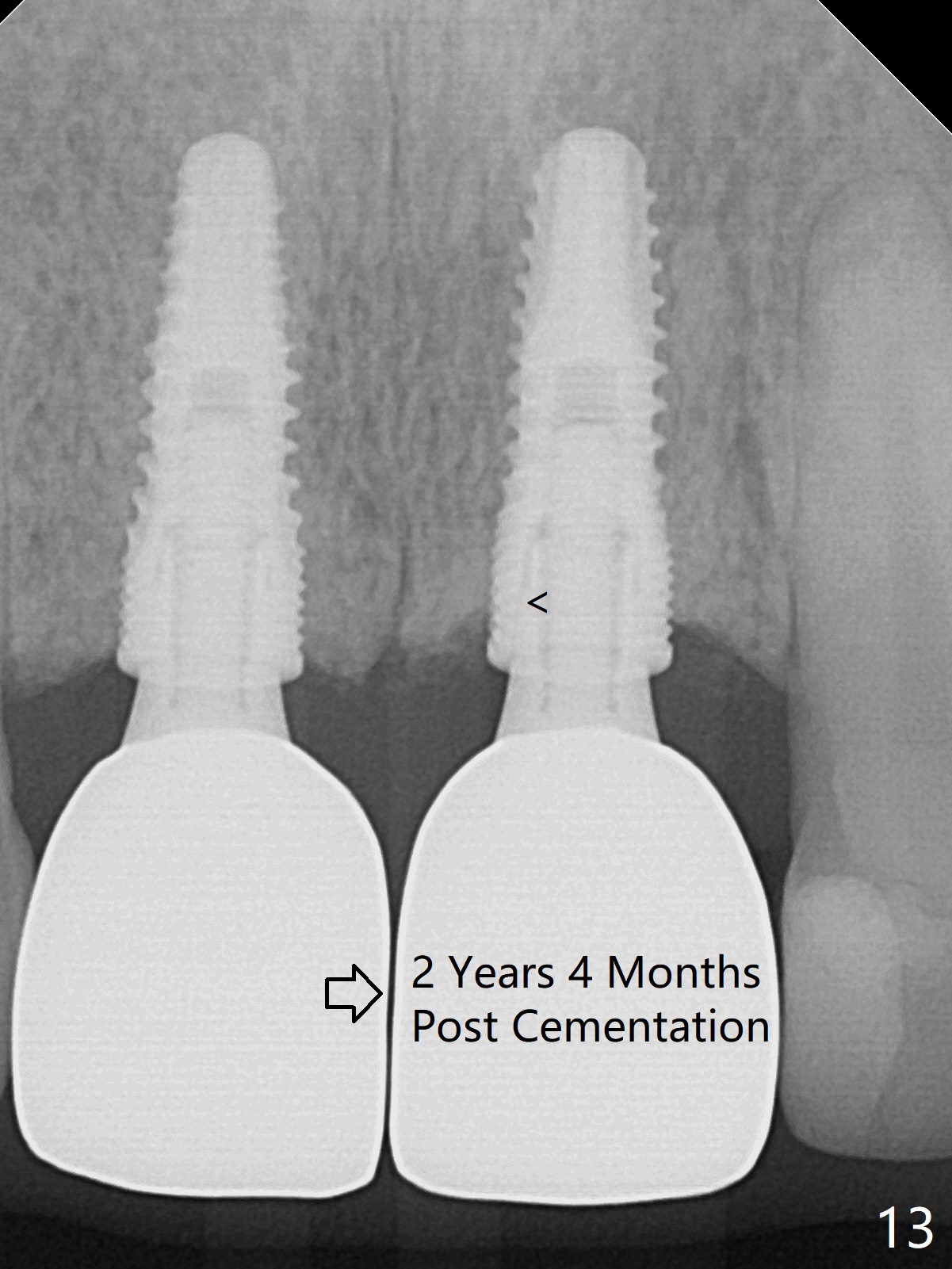
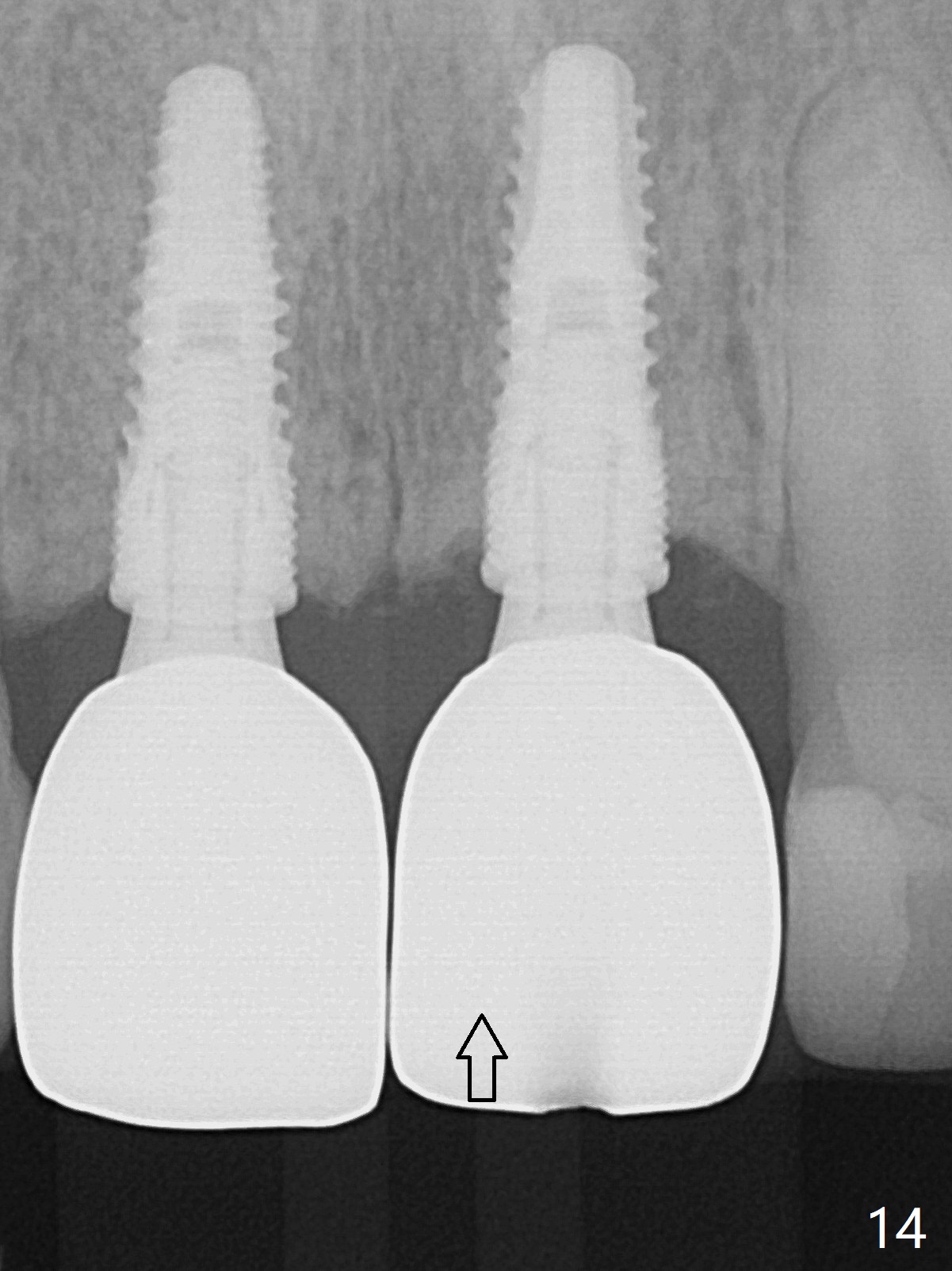
Use Existing Crowns as Provisional Restoration
When the patient returns for extraction and immediate implants, the teeth #8,9 are mobile (Fig.1,2). The buccal plate of the sites are existing, although that at #8 appears thinner. The palatal crest is the lowest with 3 mm subgingival. Initial depth of the osteotomy is 16 and 15 mm (the palatal gingival margin as landmark) at #8 and 9, respectively (Fig.3). After 4.1x12 mm SM implants are placed (Fig.4), they are placed .5-1 mm deeper (Fig.5); allograft (*) placed before and after insertion of 3.9x5.5(3) and 4.8x5.5(3) mm abutments. The existing porcelain crowns (splinted) are hollowed and relined as provisional restorations (Fig.5-7). The buccal papilla is slightly torn intraoperatively and sutured. Three weeks postop, the provisional will be modified to make incisure between the 2 crowns so that the papilla can grow down. In spite of modification, the patient complains of air leak between the crown. Temporary abutments were used with new provisional on November 7, 2017. The gingiva is healthier 8 months postop (Fig.8-11). The incisal edge of the provisional is discontinuous, (Fig.9) suggesting the access hole too buccal. When the patient returns for impression, consider using angled abutments as well as cemented ones. In fact the latter are chosen (Fig.11). The crowns are cemented without access holes 8.5 months postop (Fig.12, immediately post cementation (<: residual cement, which is to be removed)). In fact the abutment has been incompletely seated (Fig.13 <; since cementation Fig.12) and is loose 2 years 4 months post cementation (Fig.13 open arrow). The crown/abutment is removed by creating an access nearly the incisal edge; when the abutment is completely seated, the crown moves gingival (Fig.14 arrow) and rotates. Heavy occlusal adjustment is made. The patient will return for pick up impression when COVID 19 is over. Return to Upper Incisor Immediate Implant, IBS Xin Wei, DDS, PhD, MS 1st edition 08/15/2017, last revision 09/14/2020