





|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|||
|
|
|
|
|||
Place Implant as Apical as Possible to Prevent Peri-implantitis
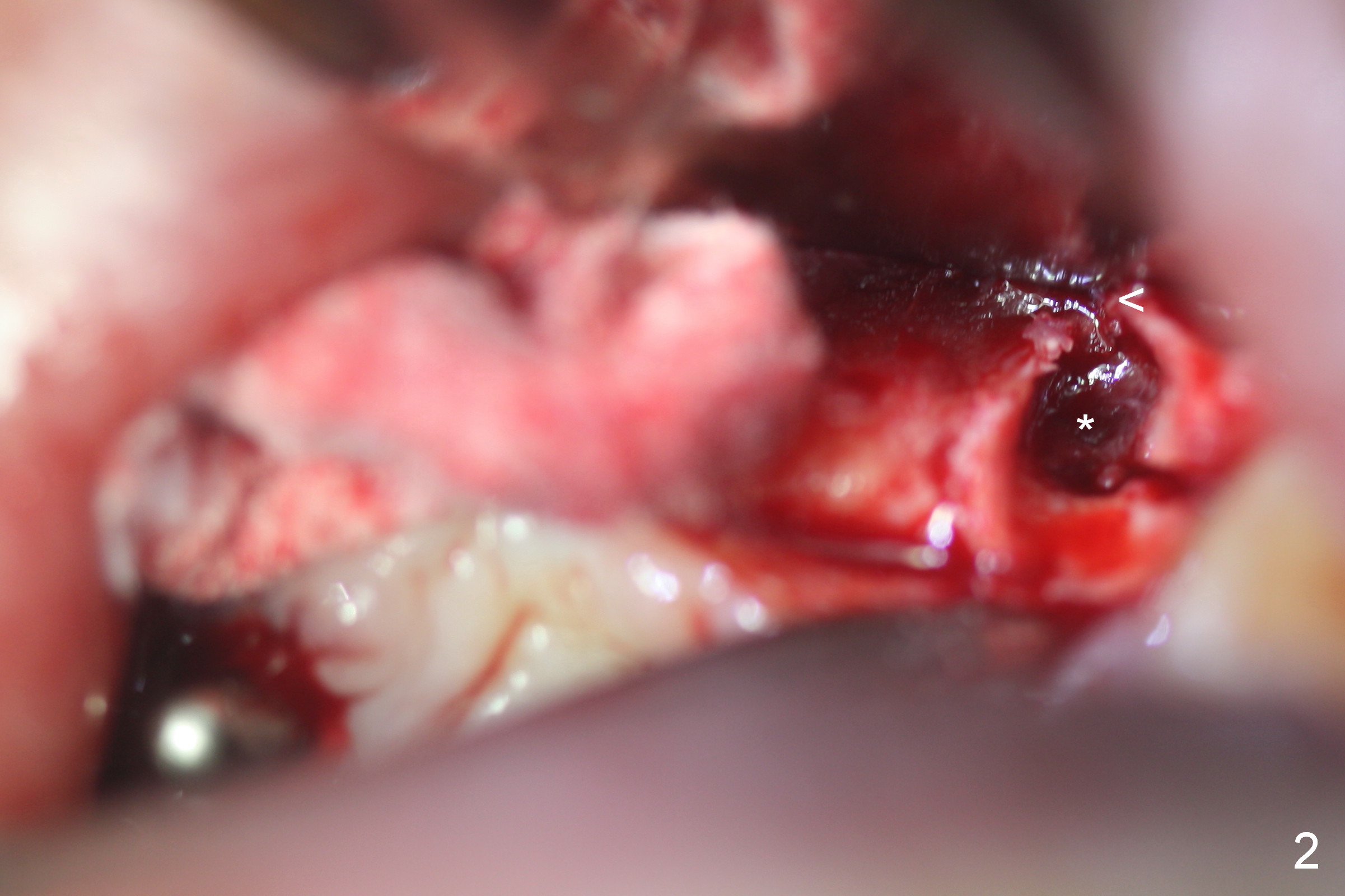
There is gingival erythema buccal to the residual root at #10 (Fig.1 *). When the tooth is extracted, the buccal plate has perforation (Fig.2 <) with granulation tissue (*). The socket is opened for better visibility and manipulation. Following 2 mm pilot drilling, a parallel pin is inserted or the drill is kept in place (Fig3,4). Since the bone has low density, osteotomies are under prepared with using long implants. A 3.8x15 mm implant is incompletely seated at #7 initially (Fig.5). After increase in osteotomy depth, the implant is placed deeper (Fig.7 arrow (<: allograft)).
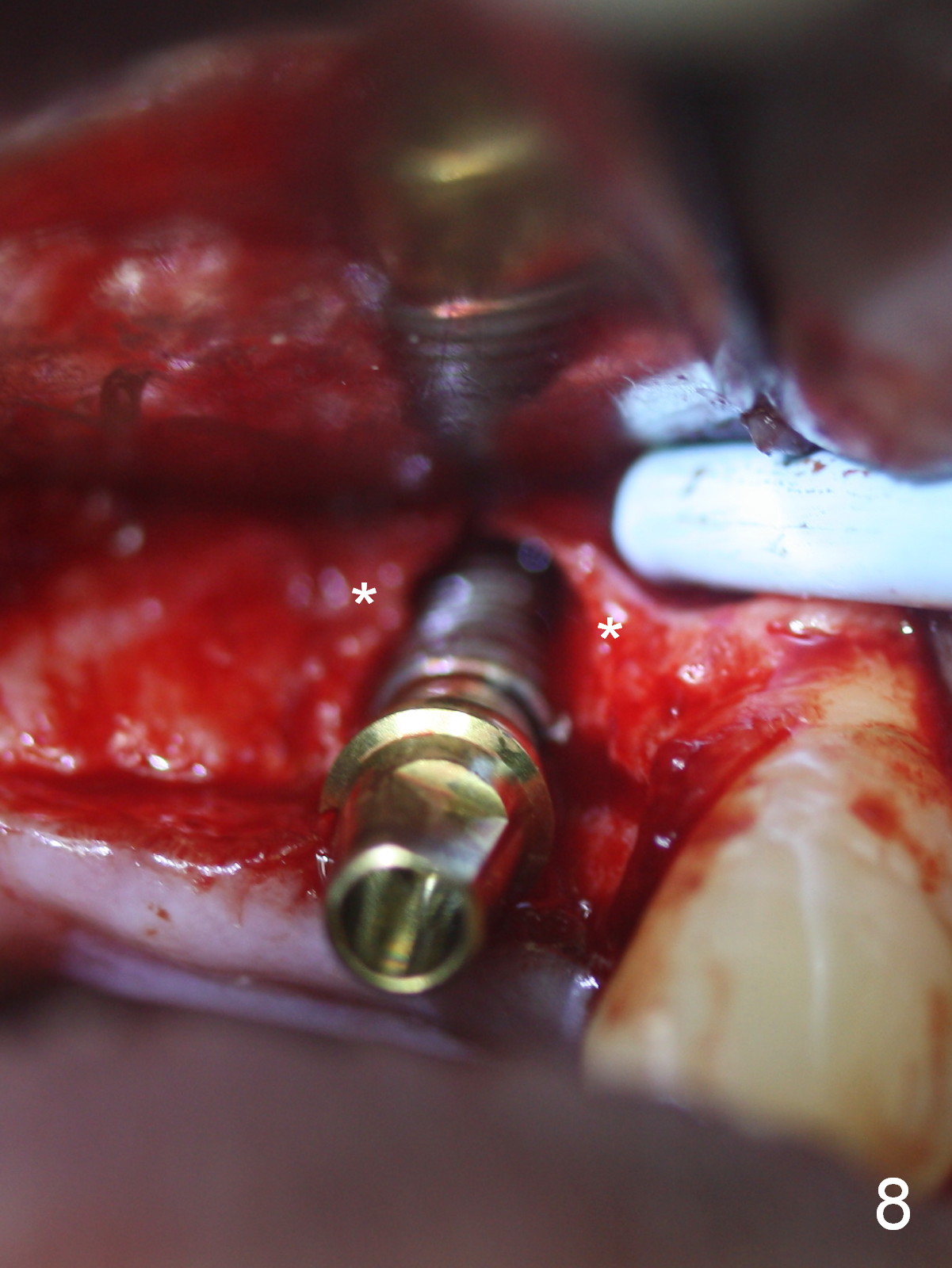
With an open socket, placement of a 3.8x16 mm implant at #10 is much easier both in buccopalatal positioning and depth (Fig.6,8). In addition guided bone regeneration is also more easily finished (Osteotape). Fig.8 shows that the implant is palatal to the buccal plate (*). There is sufficient space for bone grafting.
The patient returns for follow up 1 week postop (Fig.9). He is scheduled to return for provisional trimming in 2 weeks (Fig.10) so that the papillae will gradually grow downward (pink). If the concavity at the pontic areas is insufficient, acrylic should be added on (Fig.11 white area) so that the midline papilla may be pushed downward to be slender immediately (arrow).
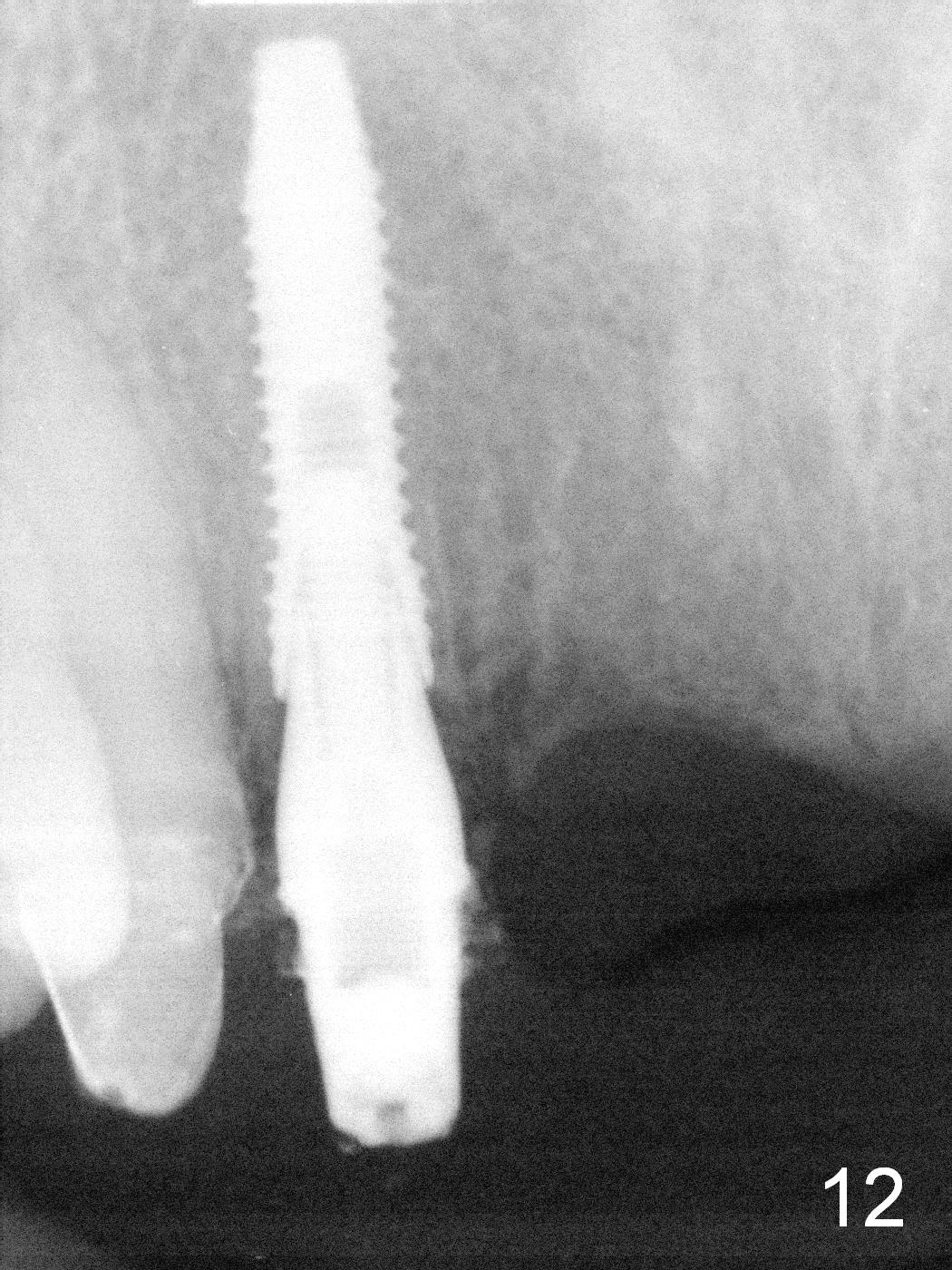
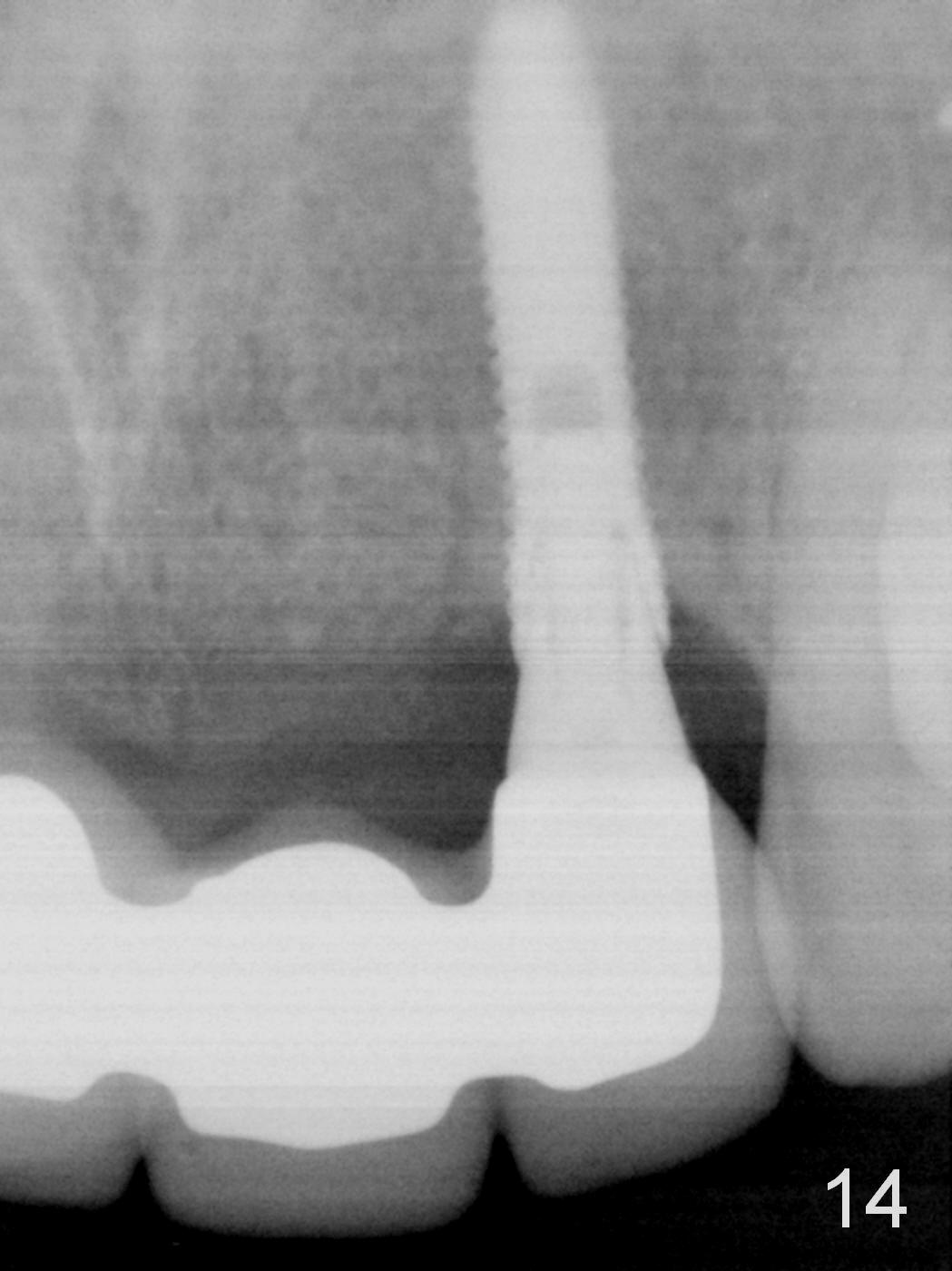
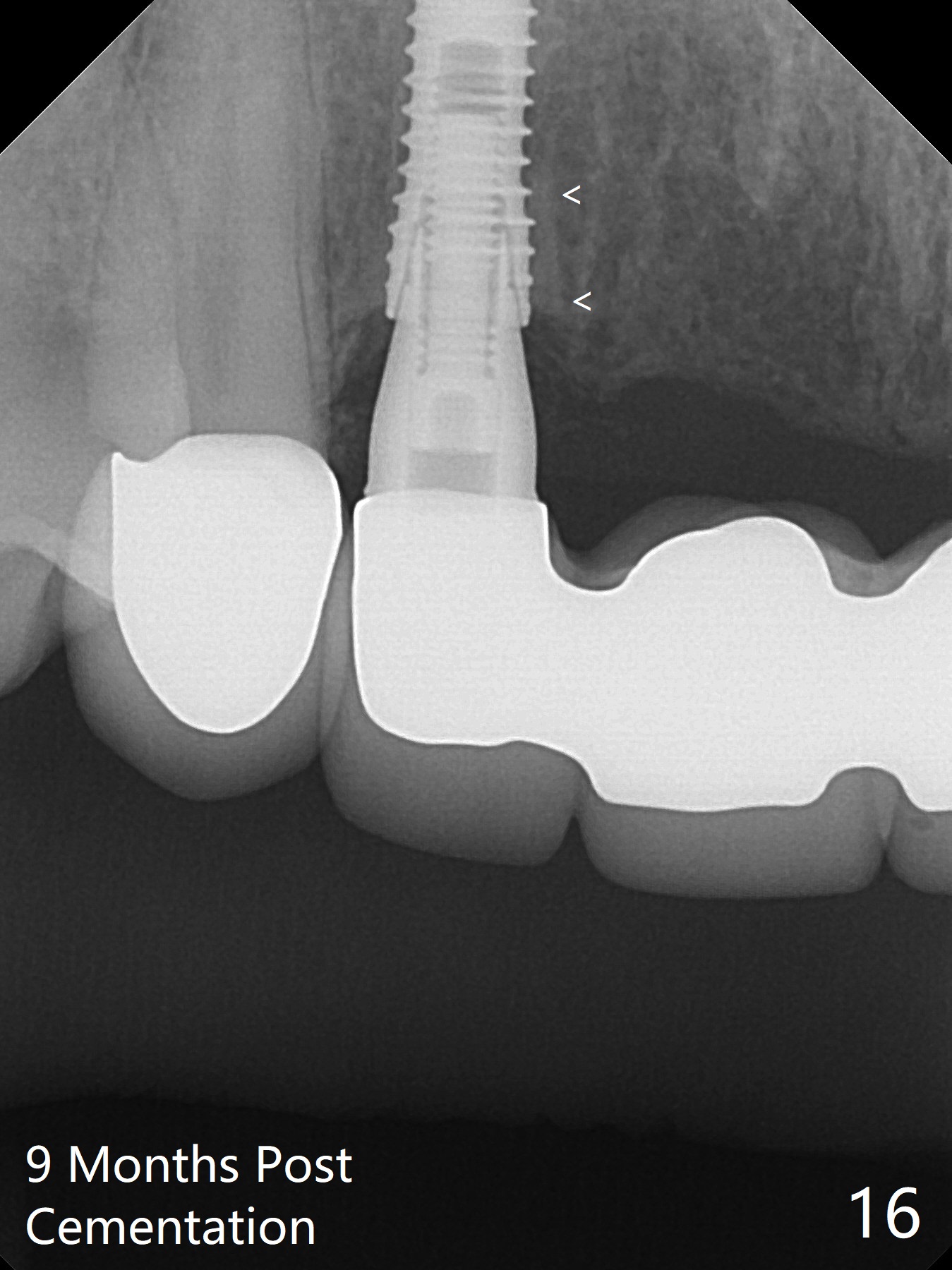
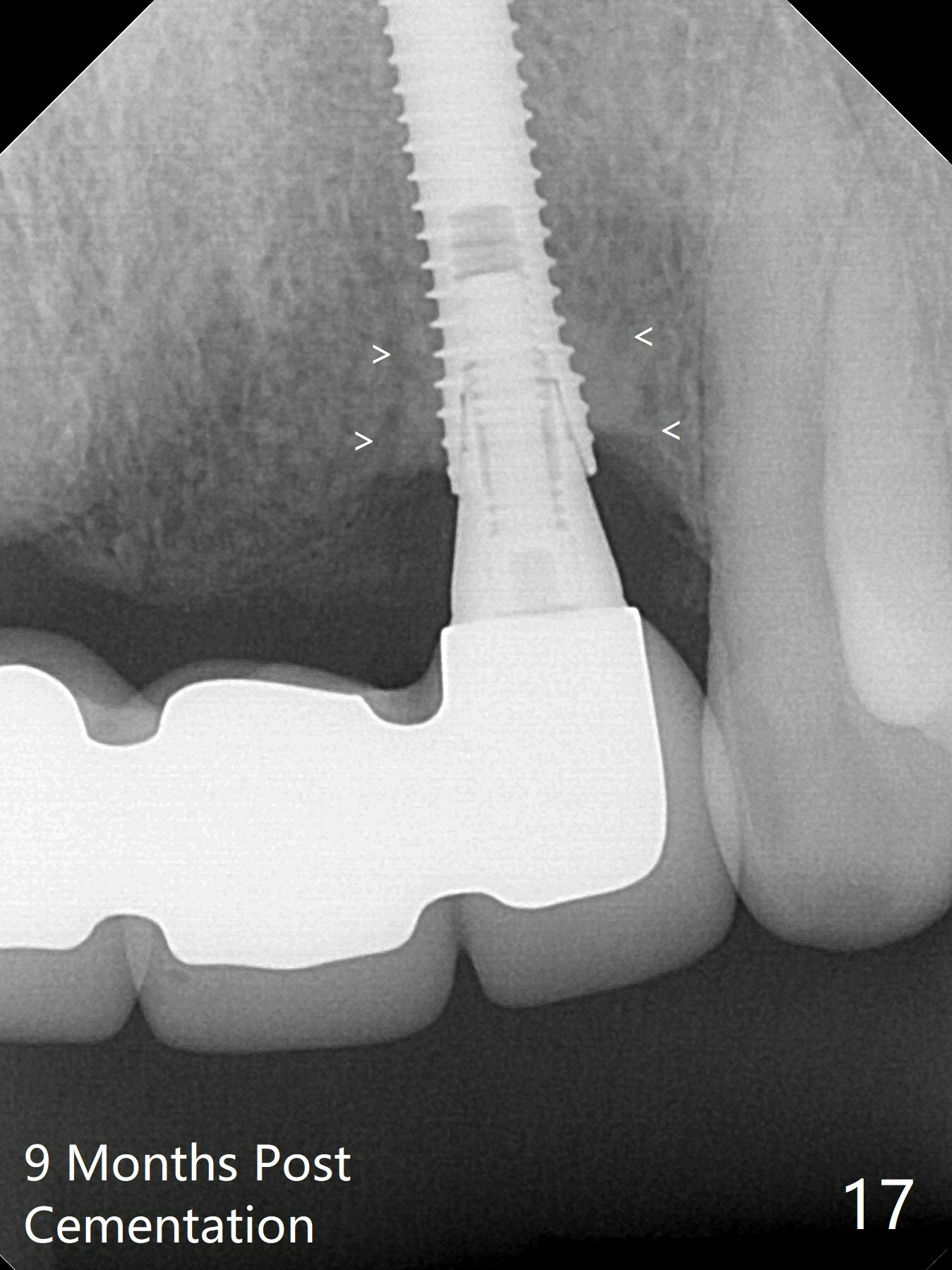
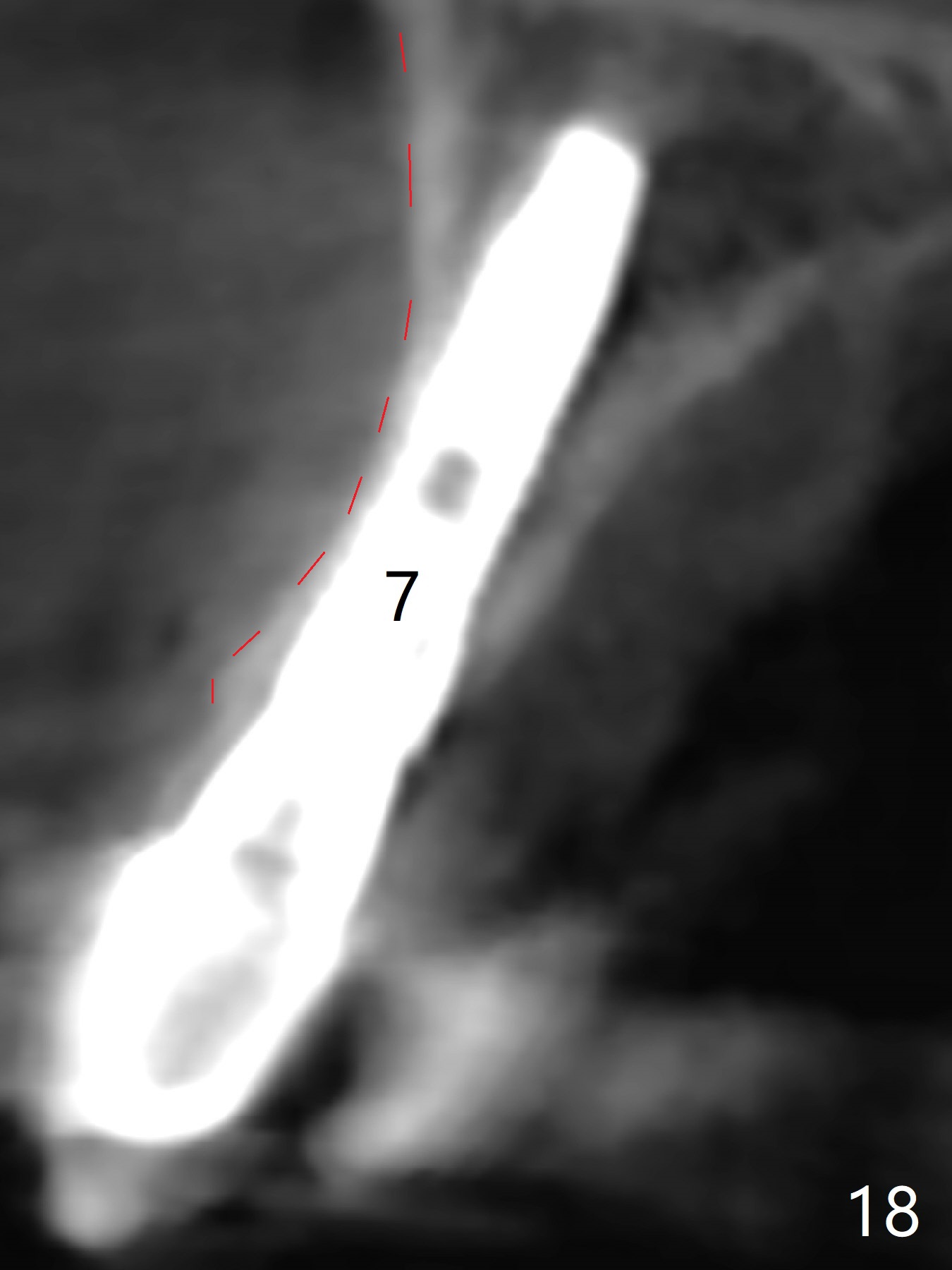
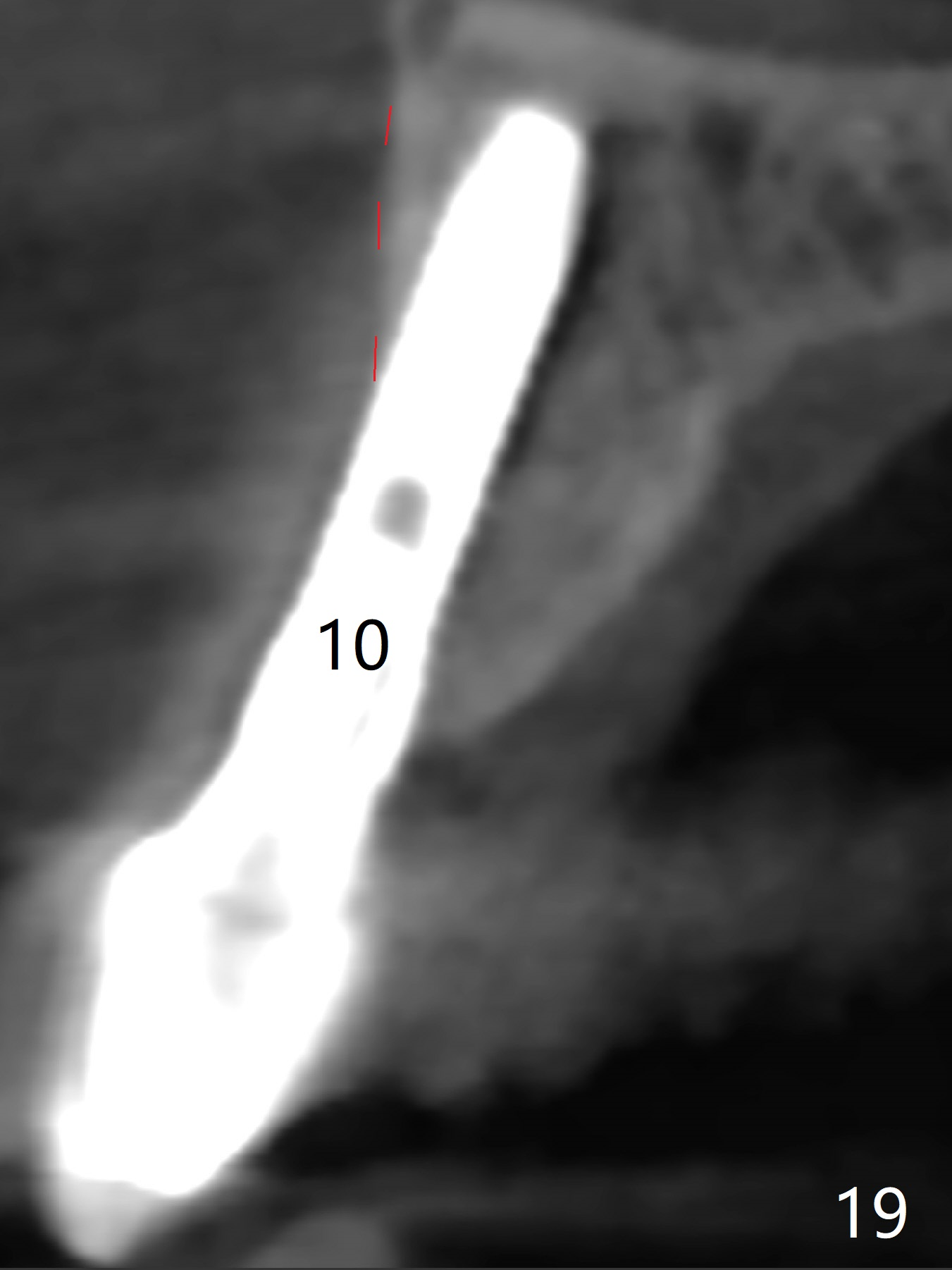
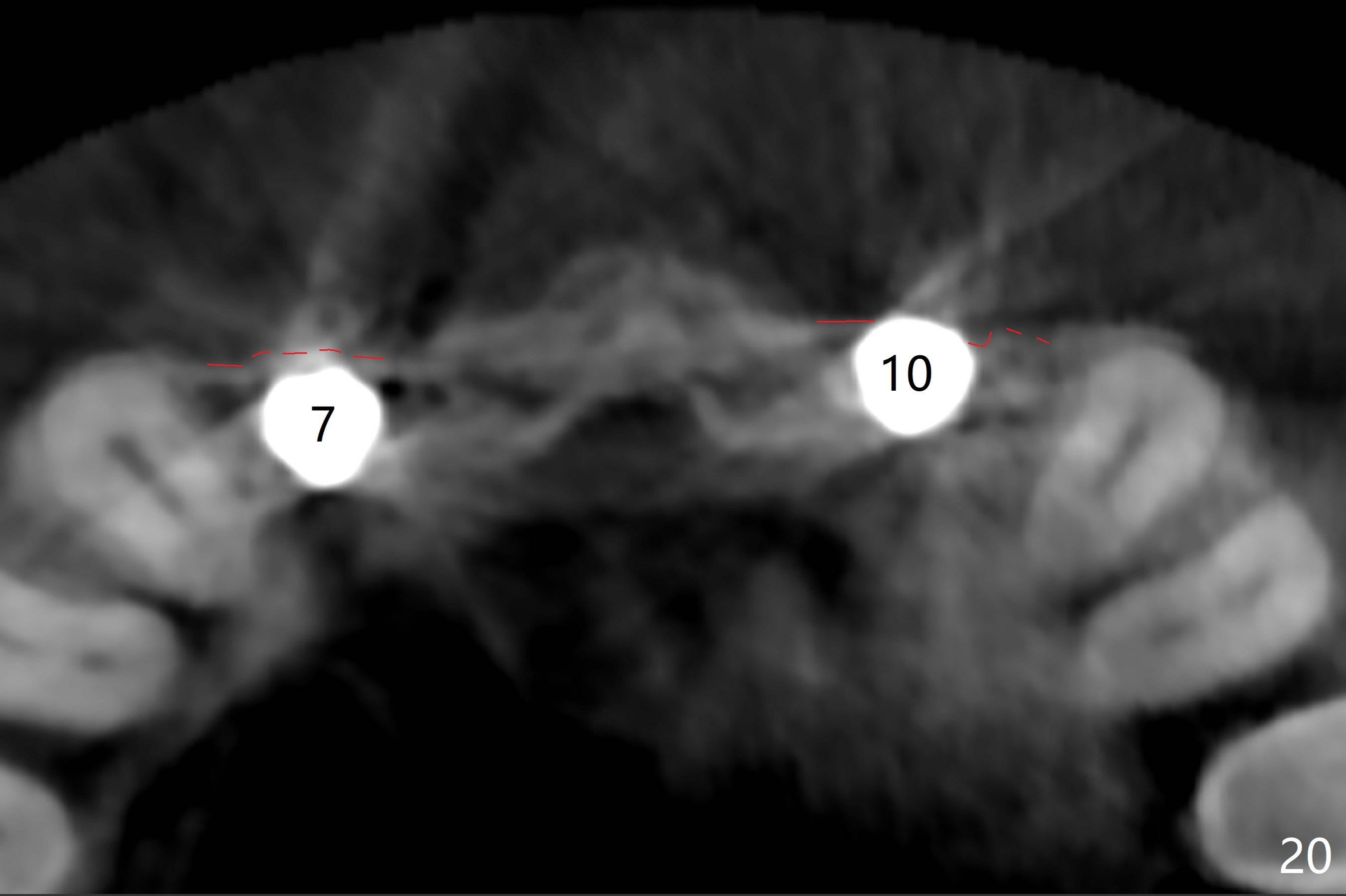
The patient returns because of dislodgement of the provisional 3 months postop. The retainer at #10 perforates at the palatal surface due to over trimming for occlusal clearance. Acrylic is added to the palatal surface of the retainers at #7 and 10 for repair and strength; the provisional is recemented (Fig.12,13). The patient returns 3 months post cementation (8 months postop) with discomfort at #10 (Fig.14,15). Clinically the gingiva is slightly erythematous, probably due to lack of oral hygiene. There is dense bone formation around the coronal ends of the implants 15 months post cementation (Fig.16,17<). Coronal (Fig.18,19) and axial (Fig.20) sections of CBCT taken 2 years post cementation show that while the buccal plate is intact at #7 (red dashed line), the gingival portion of the buccal plate at #10 remains missing.
Return to Upper Incisor Immediate Implant
#2
Crack Tooth,
19
Xin Wei, DDS, PhD, MS 1st edition 02/23/2016, last revision 07/16/2018