|
|
|
|
A Second Option for Immediate Provisional
Pressed-fit implant cannot achieve primary stability, but it can be used for immediate implant and immediate provisional. The neighboring teeth are adopted for fixation.
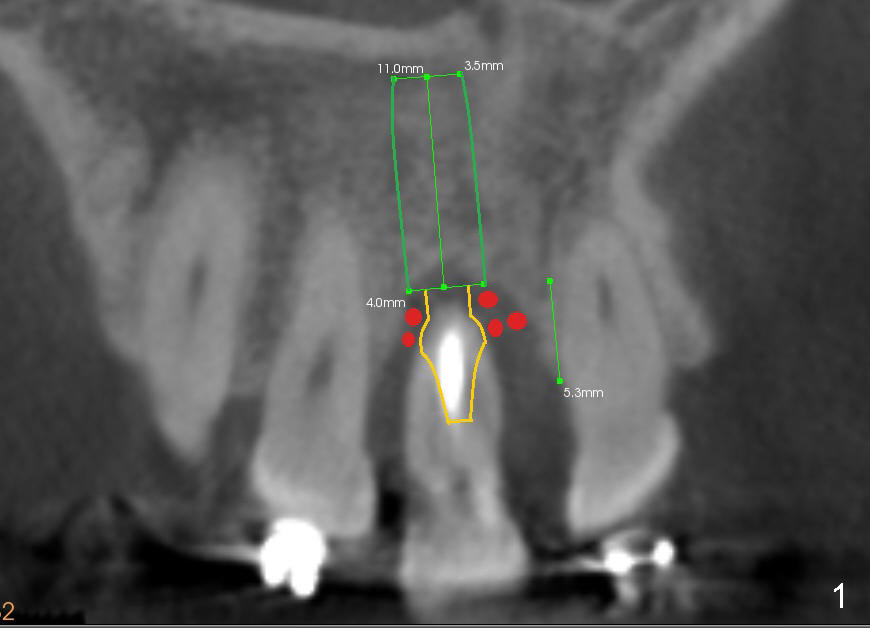
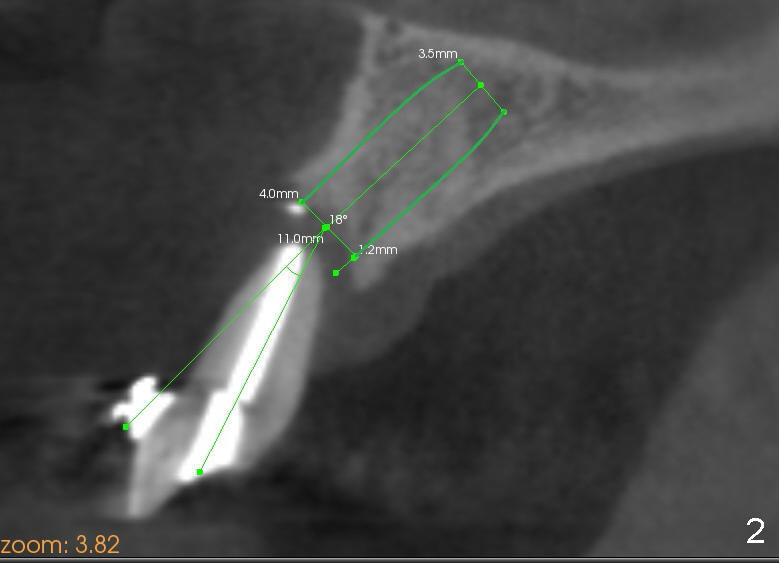
The tooth #8 of a 46-year-old lady has an endo-perio disease, complicated by occlusal trauma (Fig.1 (sagittal), 2 (coronal) CT sections).
A 4x11 mm Bicon implant with 2.5 mm well is placed, followed by insertion of a 4x6.5 mm non-shouldered abutment 15° angulation (brown outline in Fig.1). An immediate provisional is fabricated using a 4x6.5 mm plastic sleeve, crown form and jet.
After osteotomy with 2.0 mm pilot drill (16:1 handpiece) and 2.5-4.0 mm (hand) reamers (400:1 handpiece), the implant is separated from its black healing plug, attached to a 2.5 mm seating tip and a straight handle and seated into the osteotomy. If the position of the implant is good, take it out with the seating tip. Separate them extraorally. Press the abutment into the implant well extraorally. Insert the complex into the osteotomy. Rotate them into a correct angulation and check bite.
Or the implant is placed with its plug. Then the plug is separated from the implant intraorally. Insert the abutment into the well of the implant and check occlusion.
An immediate provisional is made and polished with occlusal adjustment, as mentioned above. The crown form should be a little narrower than the mesiodistal space.
Place bone graft around the most coronal portion of the implant and apical to the hemisphere of the abutment (red circles in Fig.1). If the labial gingiva is insufficient, harvest connective tissue graft from the palate.
Acid etch the proximal surfaces of the neighboring teeth. Use composite to bond the provisional to the neighboring teeth. Check occlusion again. Polish if needed.
When the 3 mm latch reamer is being used, the labial plate is palpated thin.
It is felt that the plate may be perforated when the 3.5 and 4 mm reamers are
used. A screw-typed implant
is placed instead with primary stability.
Xin Wei, DDS, PhD, MS 1st edition 02/09/2014, last revision 02/12/2014