










|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Abutment Diameter of 1-Piece Implant
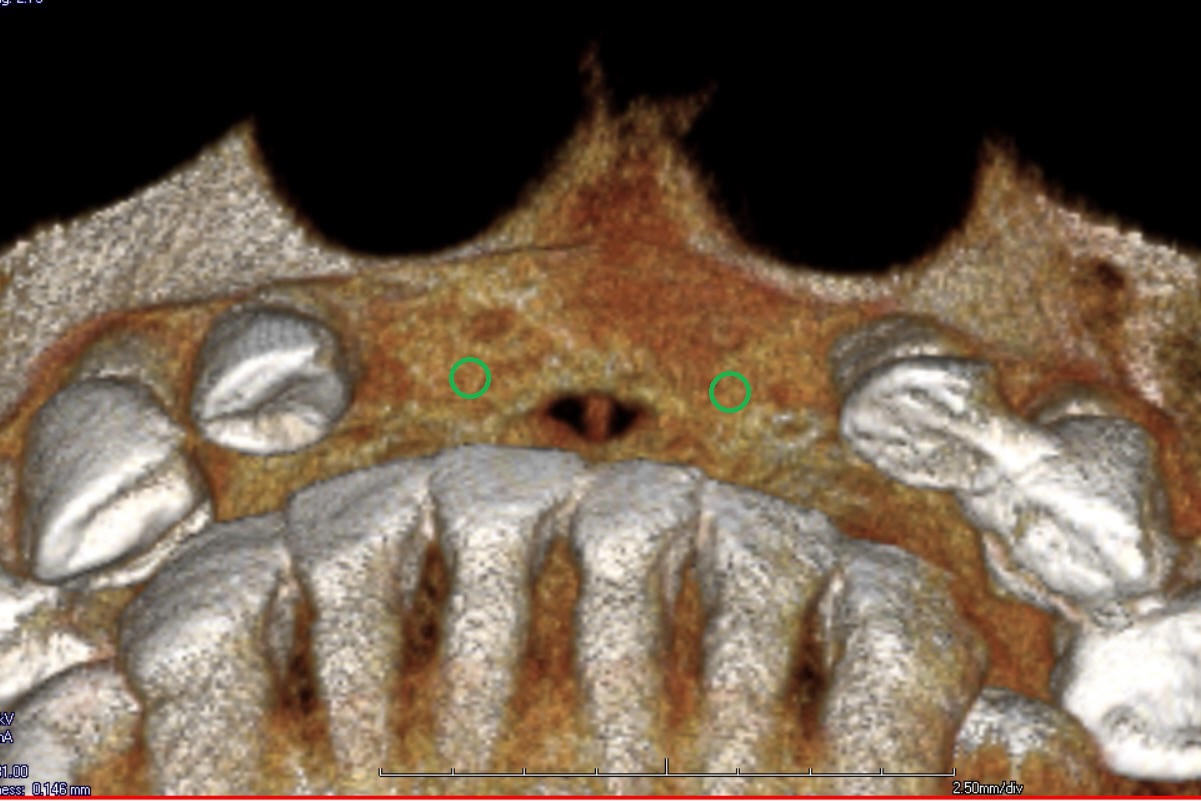
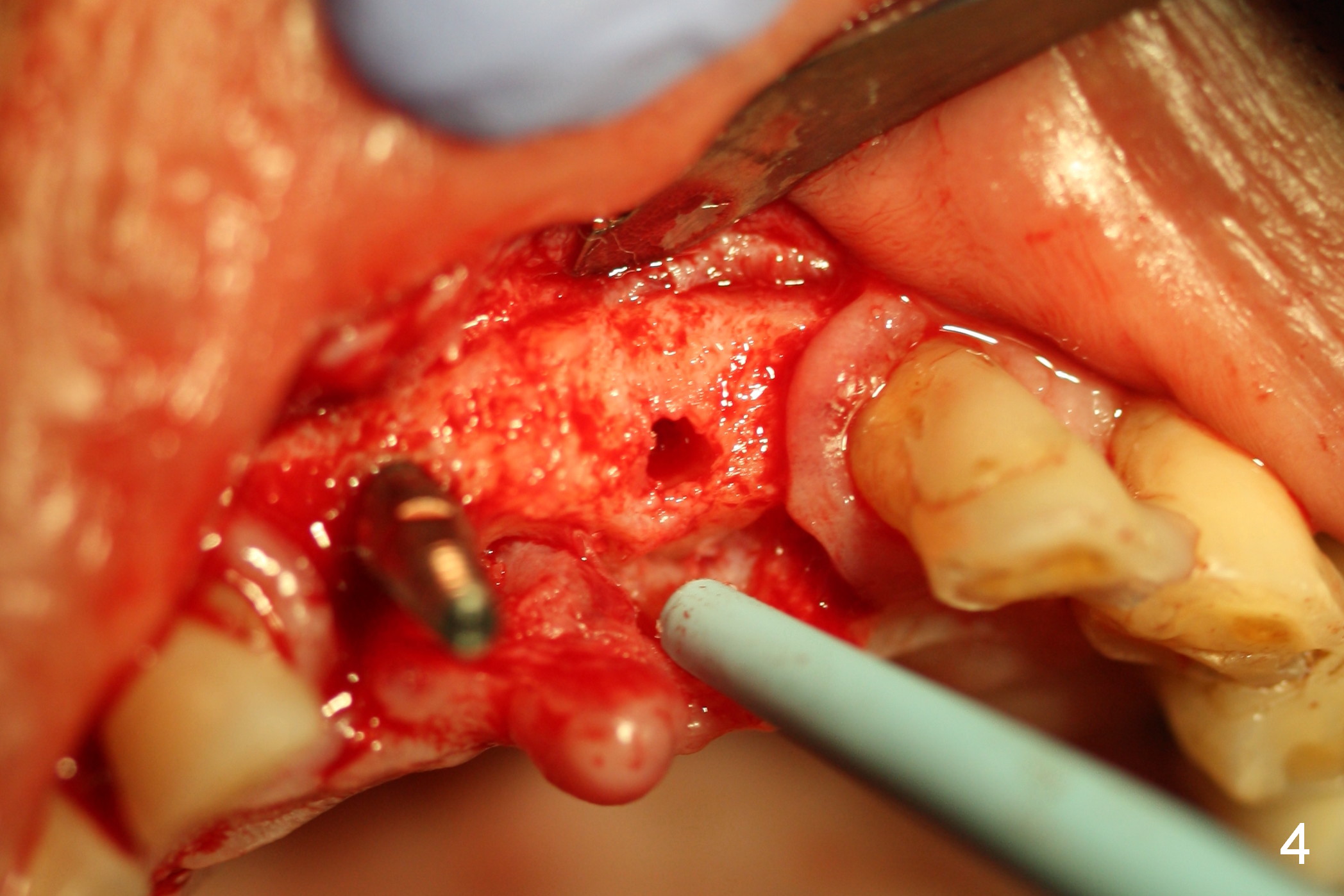
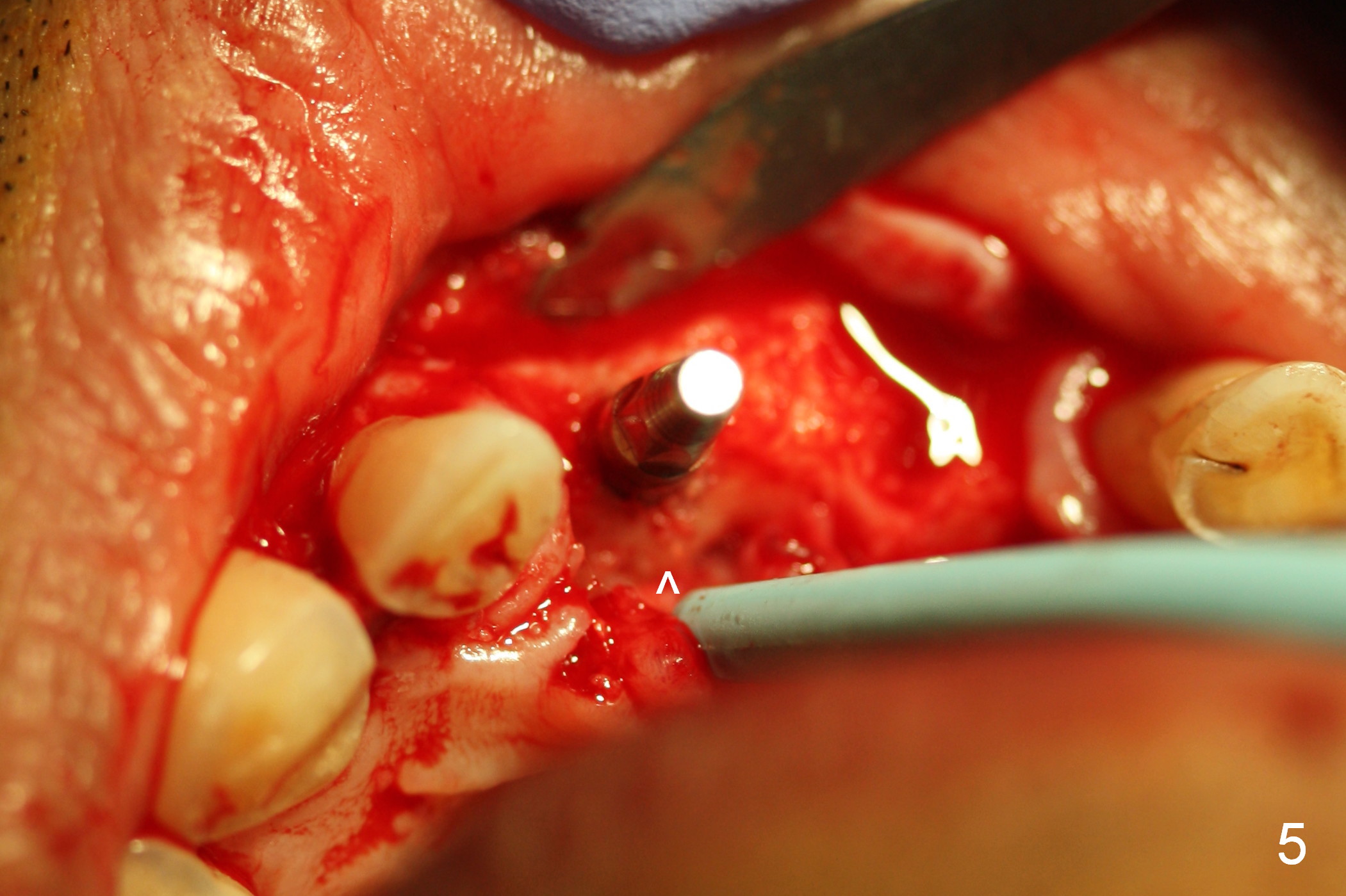
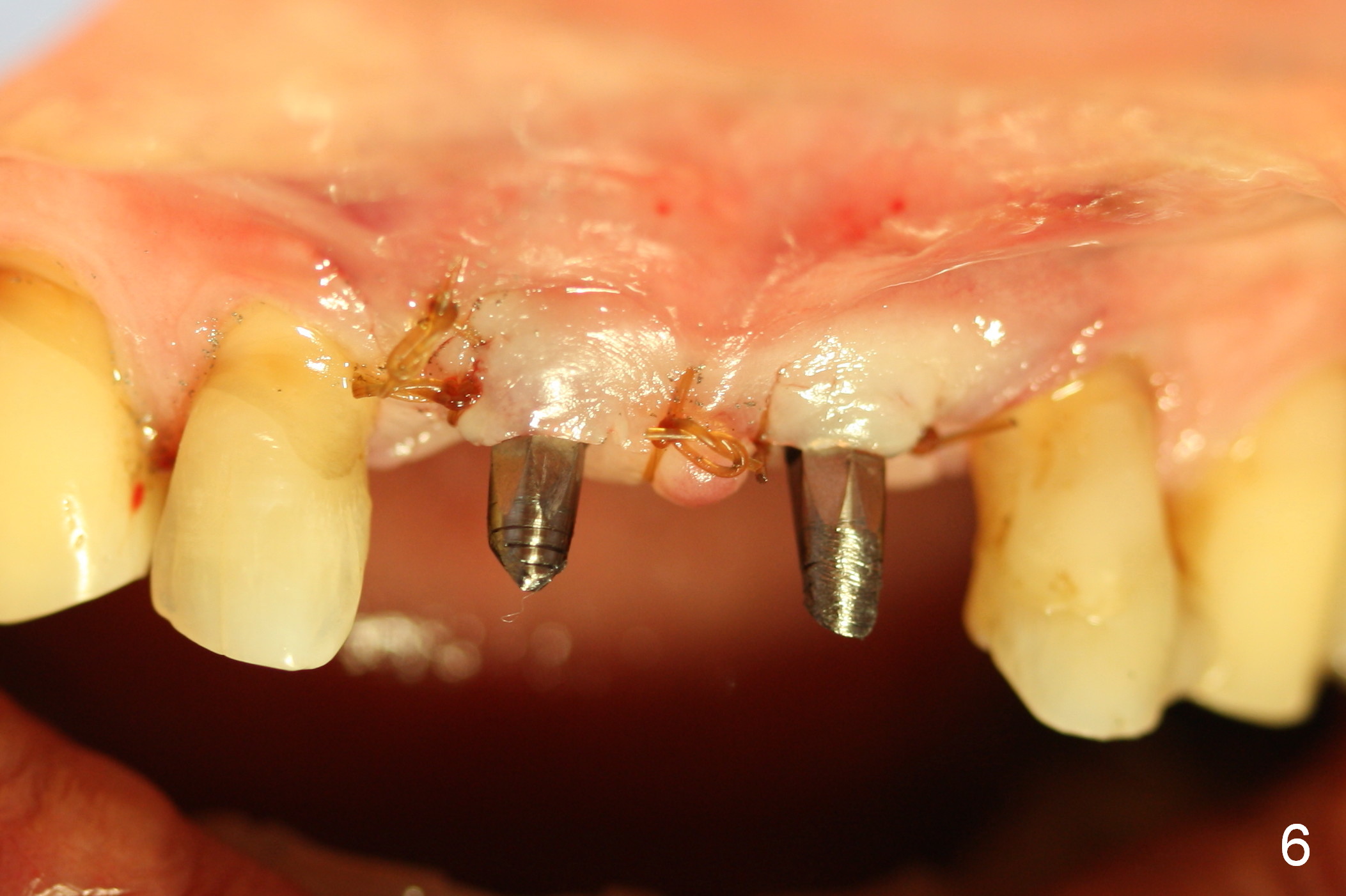
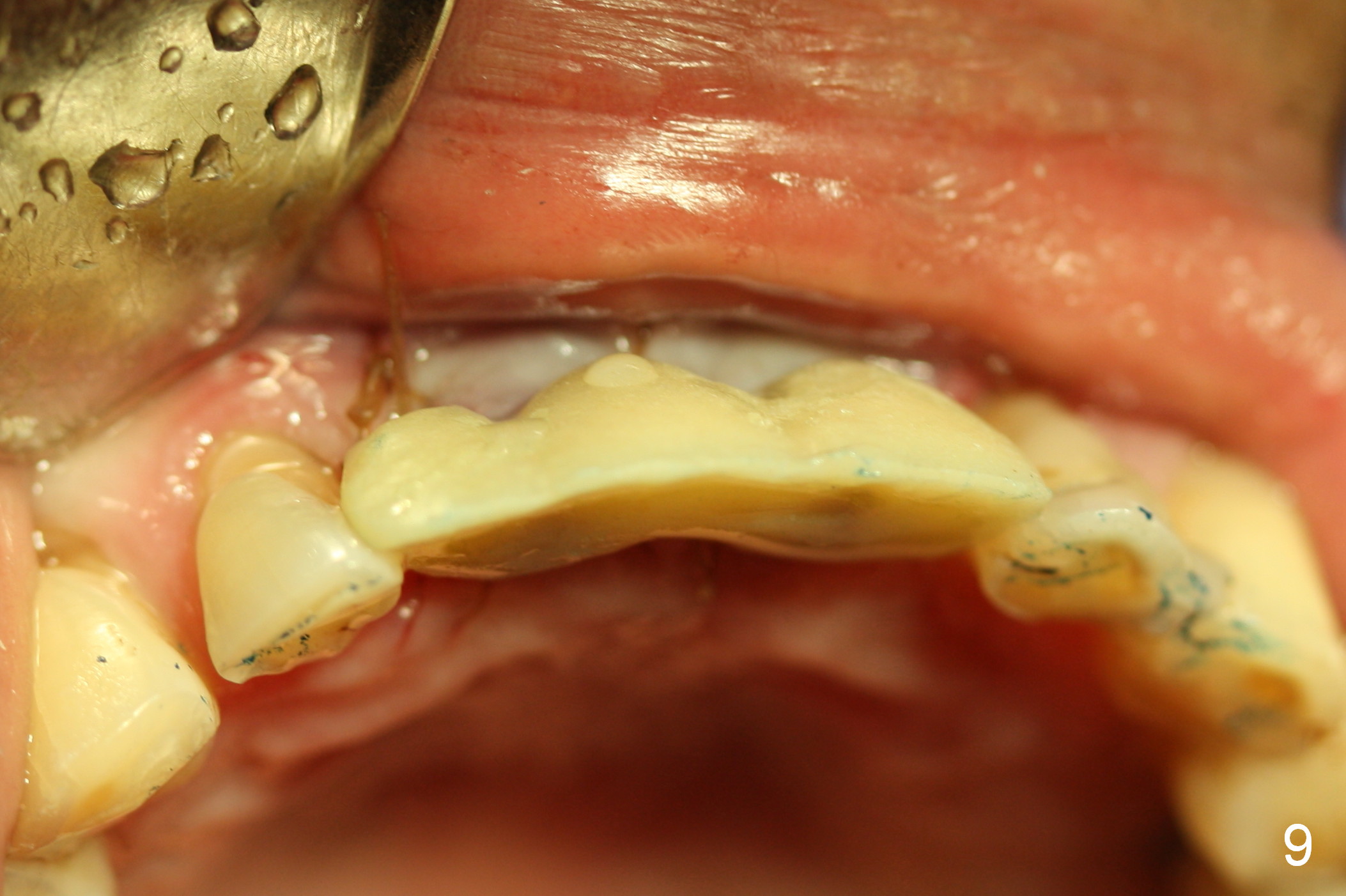
Following crestal bone exposure, osteotomy is initiated as palatal as possible (Fig.1 (CBCT 3-D image, green circles). The initial depth is 10 mm (Fig.2 with 1.2 or 1.5 mm drills) and later is extended to 12 mm (full length). There is no buccal plate vibration. When 3x14 (2) mm 1-piece implants are placed (Fig.3-5, 50 Ncm), there is no buccal or palatal plate perforation. After preparation at the coronal end of the 2.5 mm abutment (Fig.6,7, mainly buccopalatally), an immediate provisional is fabricated (Fig.8,9) to replace the existing partial (Fig.10).
Since the restorative space for the anterior teeth is limited (buccopalatal for the upper ones, mesiodistal for the lower ones), the abutment diameter of the 2-piece implant should be small, preferably 3.5 and 3.0 mm. The abutment screw should be smaller than the regular one (1.4 mm vs. 2.0 mm). Change in the diameter of the solid abutment for the narrow implants (3.0 and 3.5) should be easier.
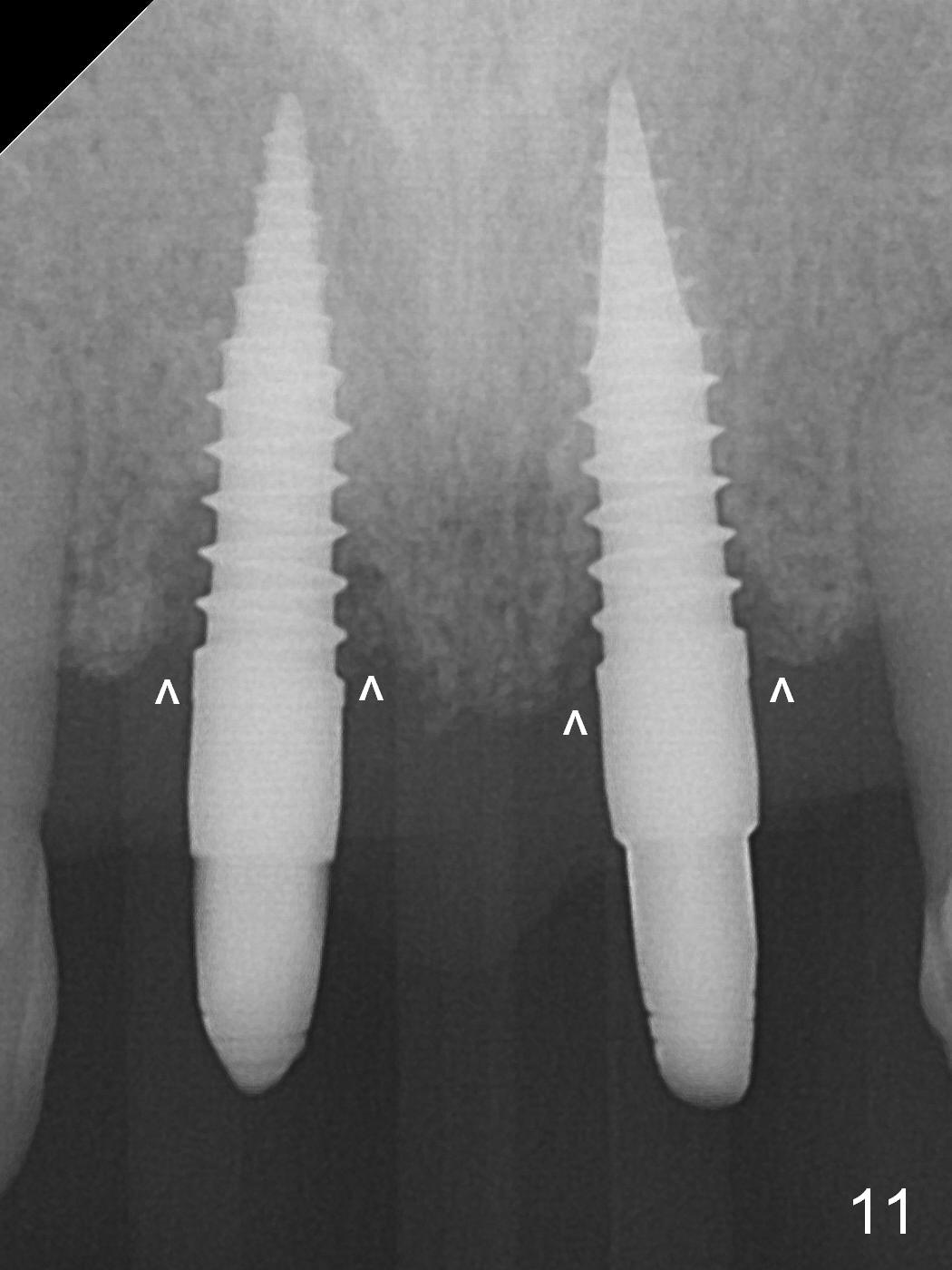
The patient returns with fractured 3-unit provisional 4 months postop. There is crestal bone loss, most likely palatal (Fig.11 ^). There are 4 papillae (Fig.12 *). A 2-unit provisional is fabricated. The right two "mini" papillae may fuse in a few weeks.
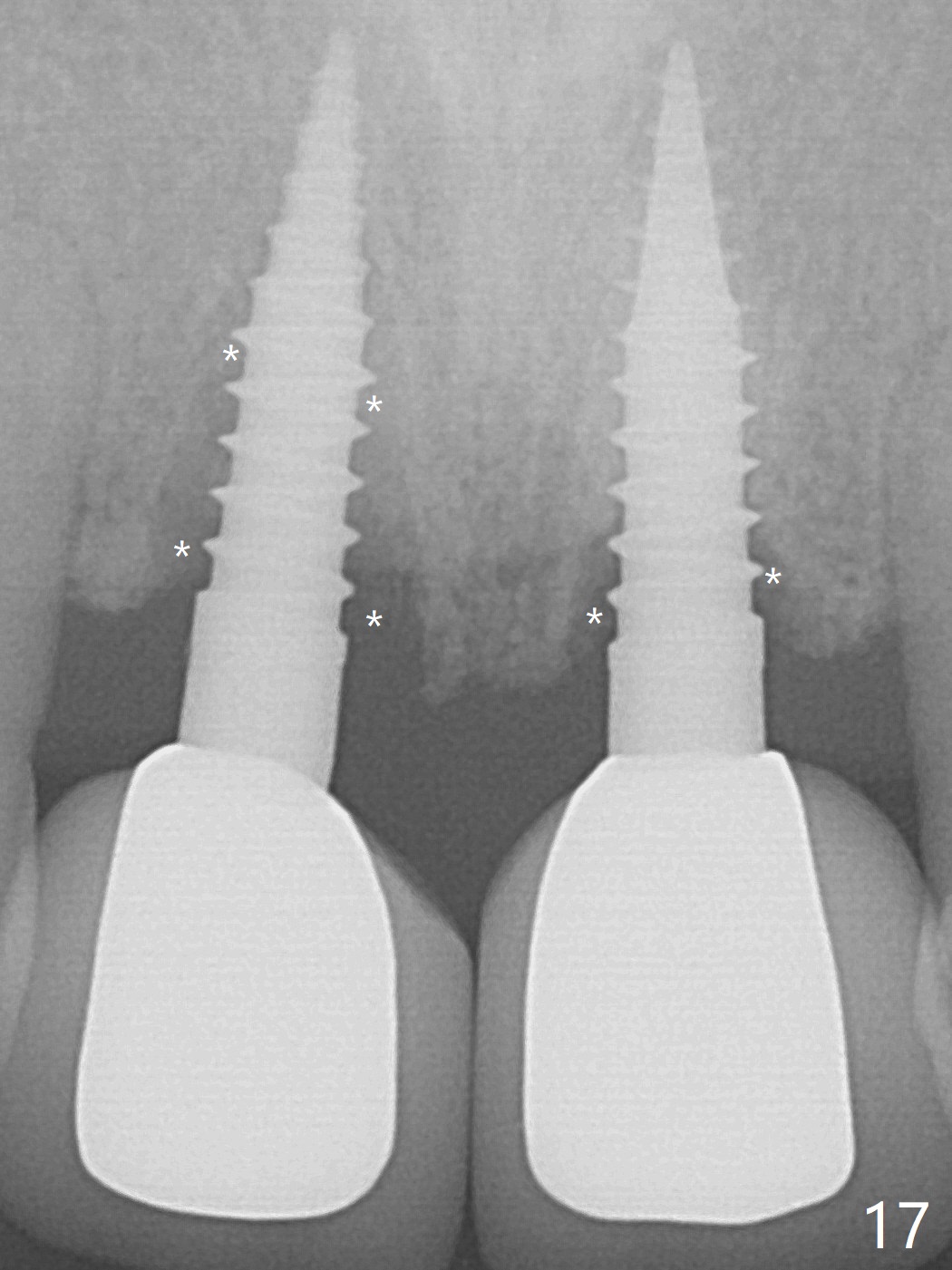
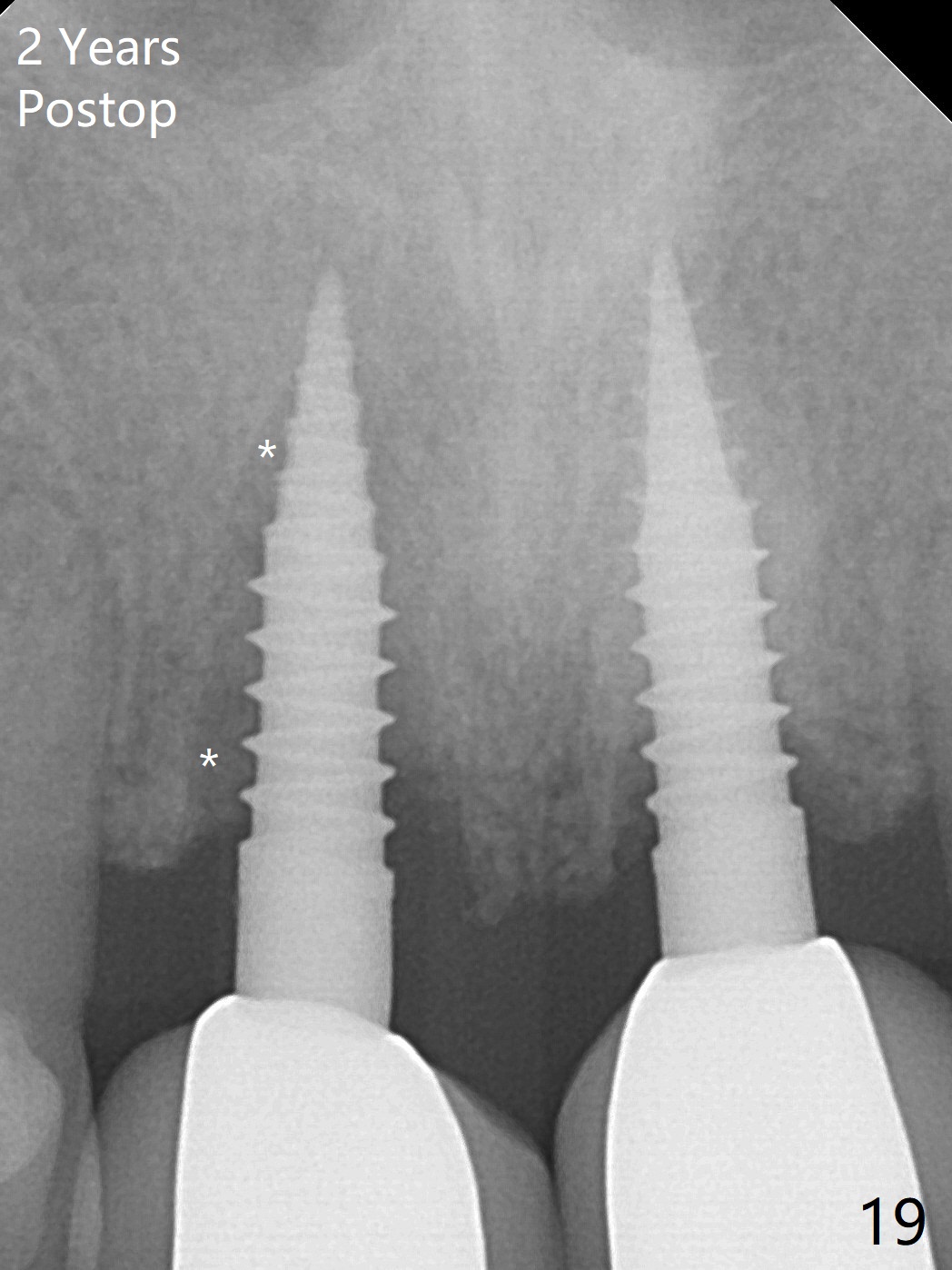
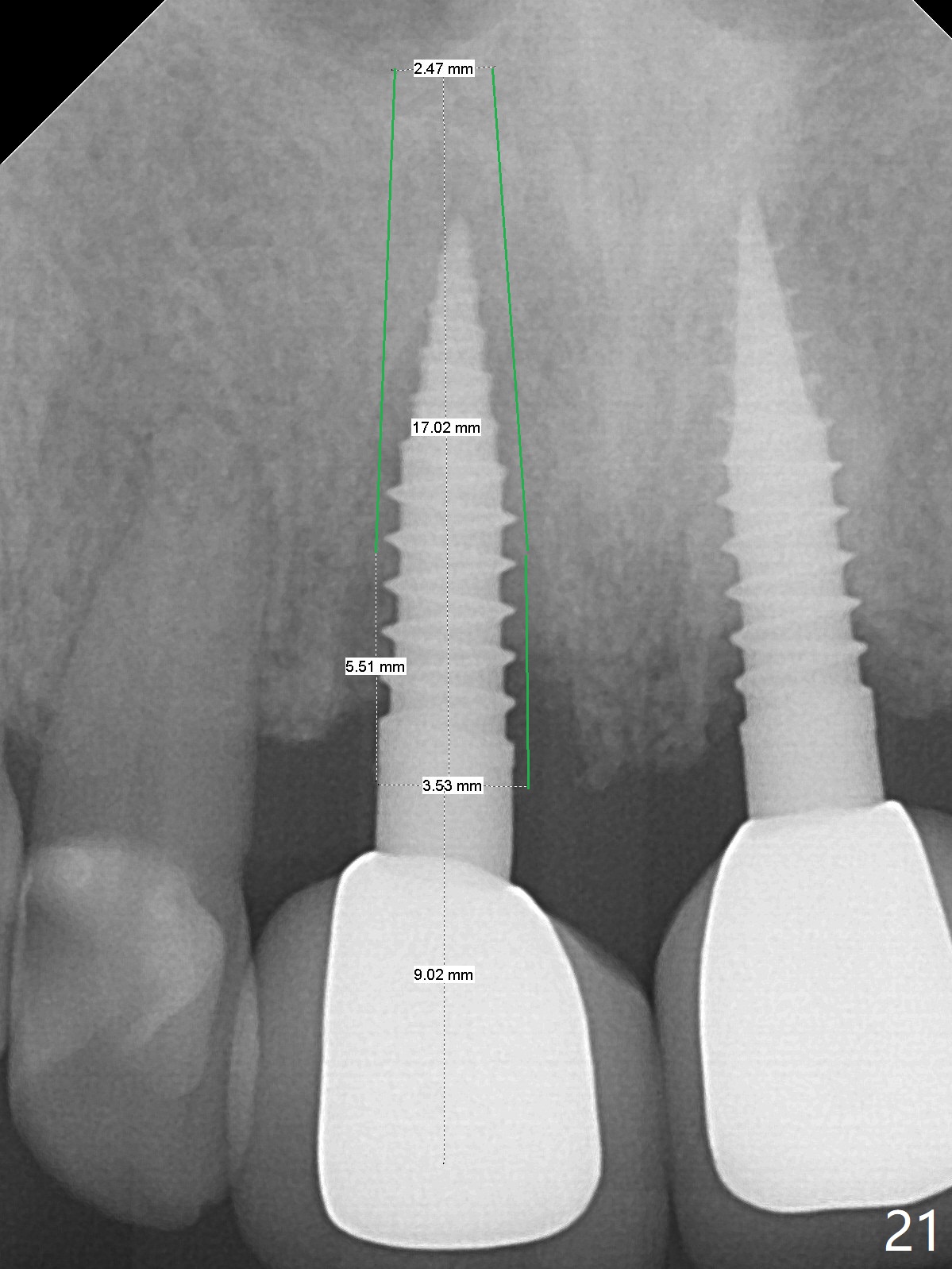
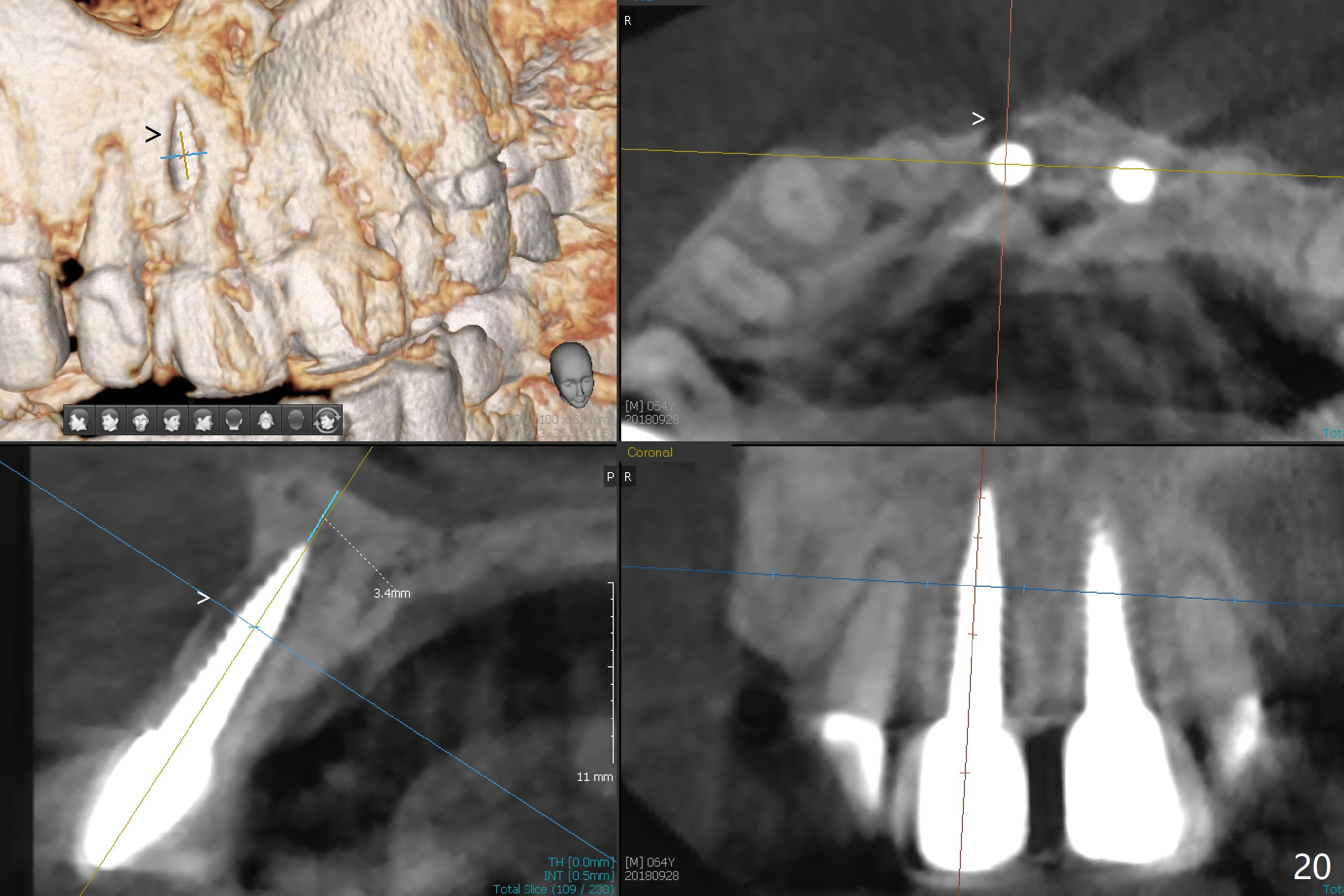
When the patient returns 3 weeks after the last appointment, the right two papillae appear less prominent (Fig.13,14 *). Impression is taken with shade selection (Fig.15). There is no black triangle between the central incisors immediately post cementation (Fig.16). There is increased bone loss 1 year 2 months post cementation (Fig.17, particularly at #8: *), although the gingiva remains healthy (Fig.18). Smaller 1-piece implants (2 or 2.5 mm) or lower torque (increase in osteotomy) may be associated with less bone resorption. The crown is loose with severe bone loss 2 years postop (1 year 9 months post cementation, Fig.19), especially buccal (Fig.20 >). Following implant removal and debridement, extend the osteotomy for 2 mm using 1.2, 1.5 and 2 mm drills. If the defect is not too extensive, bone graft will be done from inside the osteotomy out. Insert a 3x16(4) mm 1-piece or 3.5x17 mm 2-piece implant (Fig.21). Take Alginate impression when the patient returns for surgery in case of failure of implant re-placement.
Return to
Upper Incisor Immediate
Implant, IBS,
Improvement,
Atrophic Ridge,
3
10
14
15
19
30
Xin Wei, DDS, PhD, MS 1st edition 09/16/2016, last revision 10/16/2018