




|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|||||
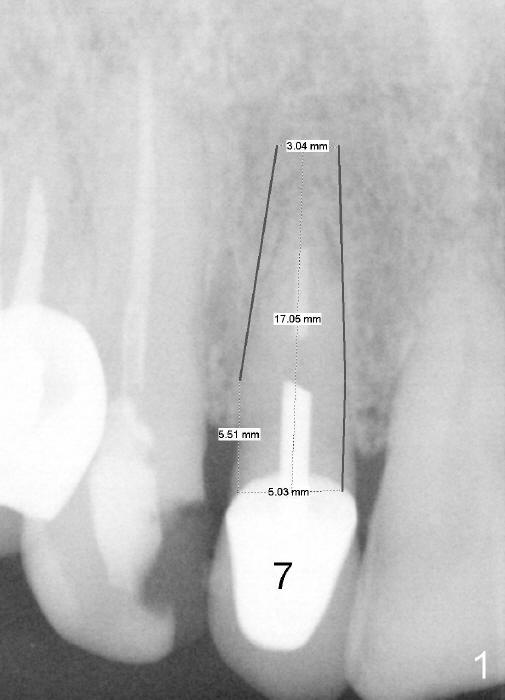
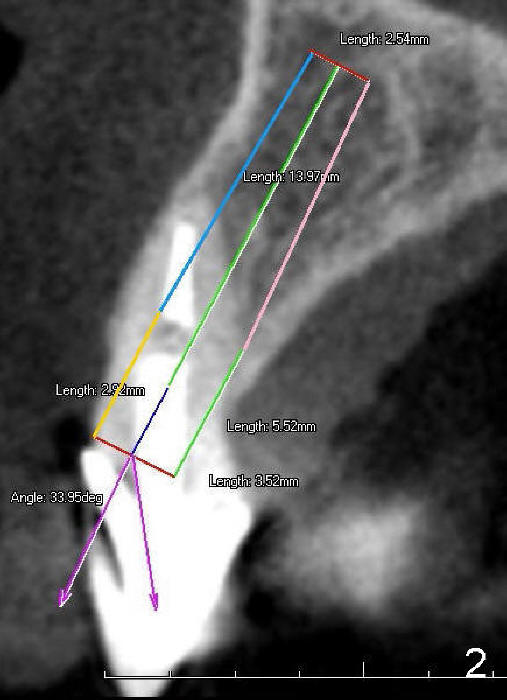
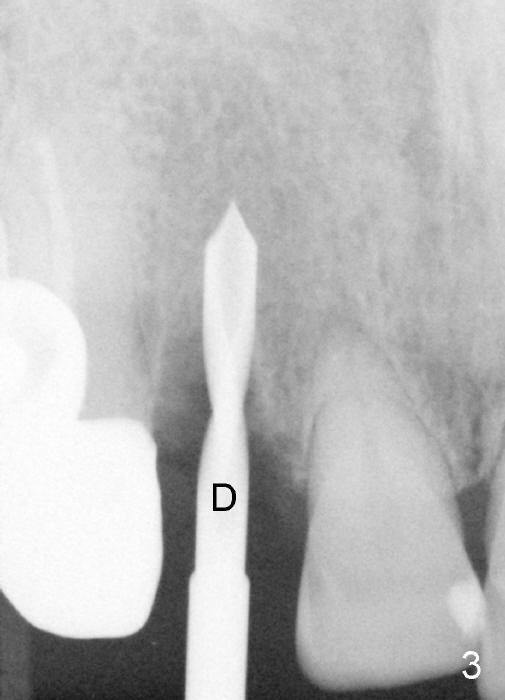
A 70-year-old Oriental lady has a history of osteoporosis and has just begun an oral Bisphosphonate once a week. The tooth #7 has fractured for a while. PA (Fig.1) and CBCT (Fig.2 coronal section) taken prior to fracture show that the diameter of the immediate implant can be 3.5 to 5.0 mm. The mesiodistal dimension of the extracted root is 3.5 mm, buccolingual 4 mm. Osteotomy starts in the middle palatal wall with a 2 mm pilot drill at the depth of 14 mm. The bone density is low. Minimal bone is harvested from the reamers. The depth increases to 17 mm. The osteotomy is initially under prepared (2.5x17, 3x14 mm reamers). A 4x17 tapered implant tends to go to the original socket (buccally). When the osteotomy increases (3x17, 3.5x14 mm), the implant has insertion torque <20 Ncm. It also deviates buccally coronally.
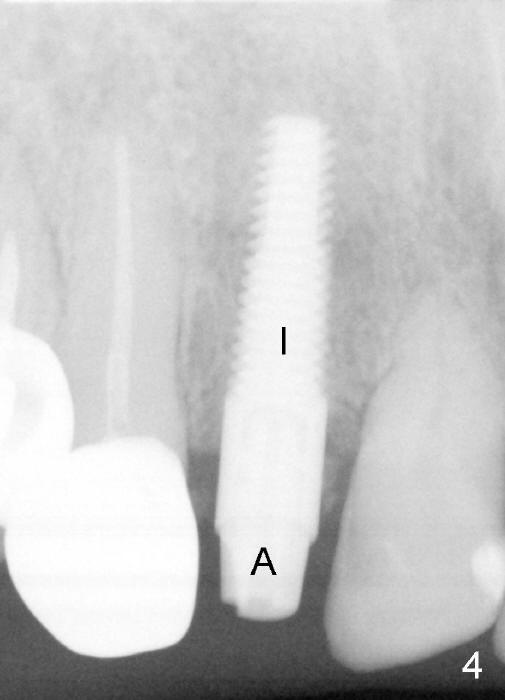
The implant is removed. Allograft and Osteogen are placed buccally and in osteotomy site. The implant is re-inserted. The trajectory improves, but the torque remains the same. A short abutment is placed to hold perio dressing in place. An immediate provisional is not fabricated.
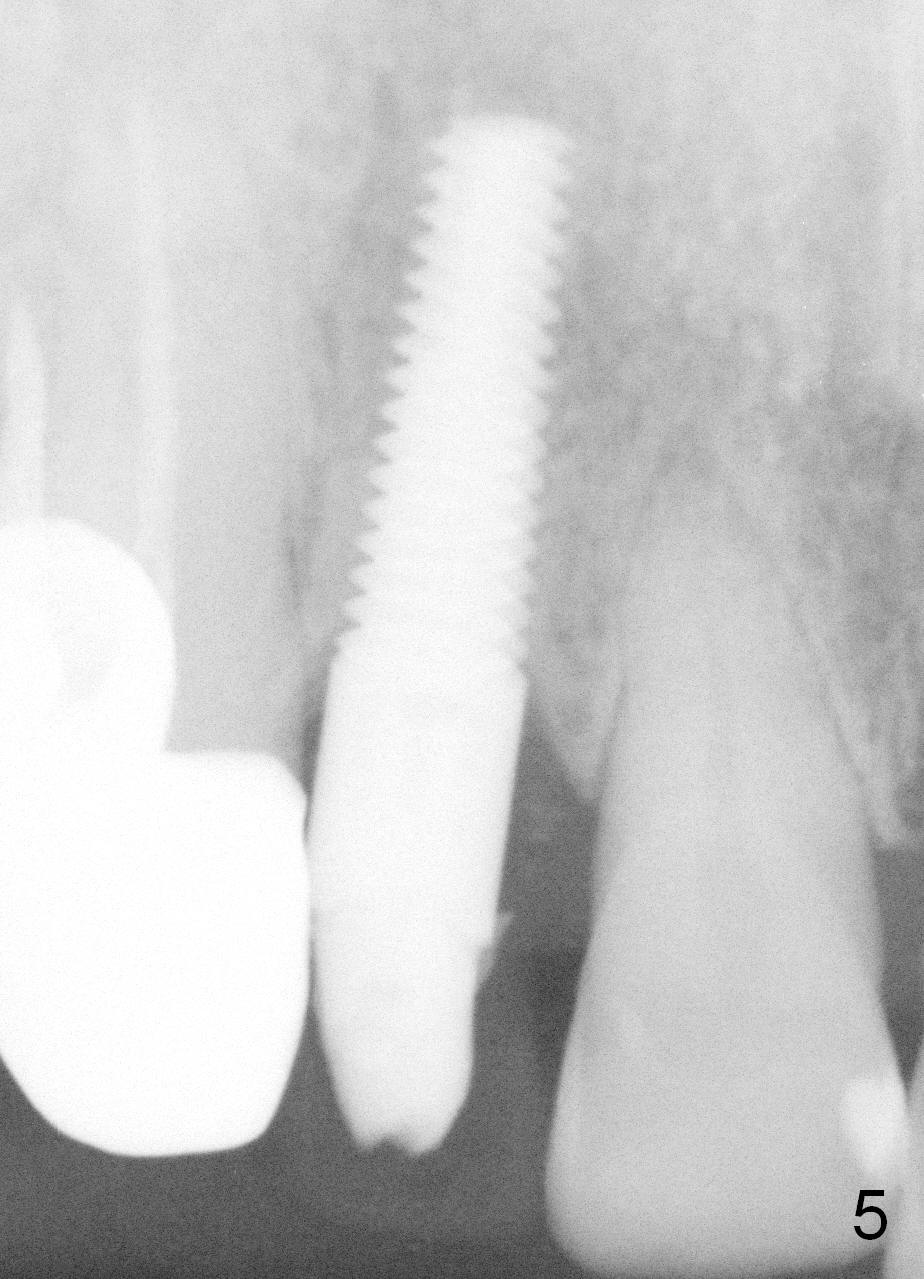
The implant appears normal postop. But the patient feels pain when the implant/abutment are prep for crown 3.5 months postop. A temporary crown is fabricated. A PA taken 7 months postop shows apparently normal healing (Fig.5). The implant/abutment are re-prep for impression (Fig.6). When the permanent crown is delivered, it looks bulky. The gingival margin is higher than that of the central incisor (Fig.7). The implant/abutment are heavily reduced labially. The gingival margin of the temporary crown is short so that the gingiva may grow coronally gradually (Fig.7). The buccal plate appears not atrophic (Fig.8 arrows).
The implant/abutment is re-prep with modification of the provisional 10 months postop (Fig.9,10).
In brief, it is difficult to achieve primary stability in a patient with osteoporosis. Osteotomy should be underdeveloped.
When the patient returns for final impression, the incisal edge of the provisional should be shortened. Remove it to determine whether the abutment height should be reduced. Take a photo before impression. Be critical on the labial reduction of the implant/abutment.
Return to Upper Incisor Immediate Implant, Dr. Wu
Xin Wei, DDS, PhD, MS 1st edition 07/21/2014, last revision 08/04/2018