







|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
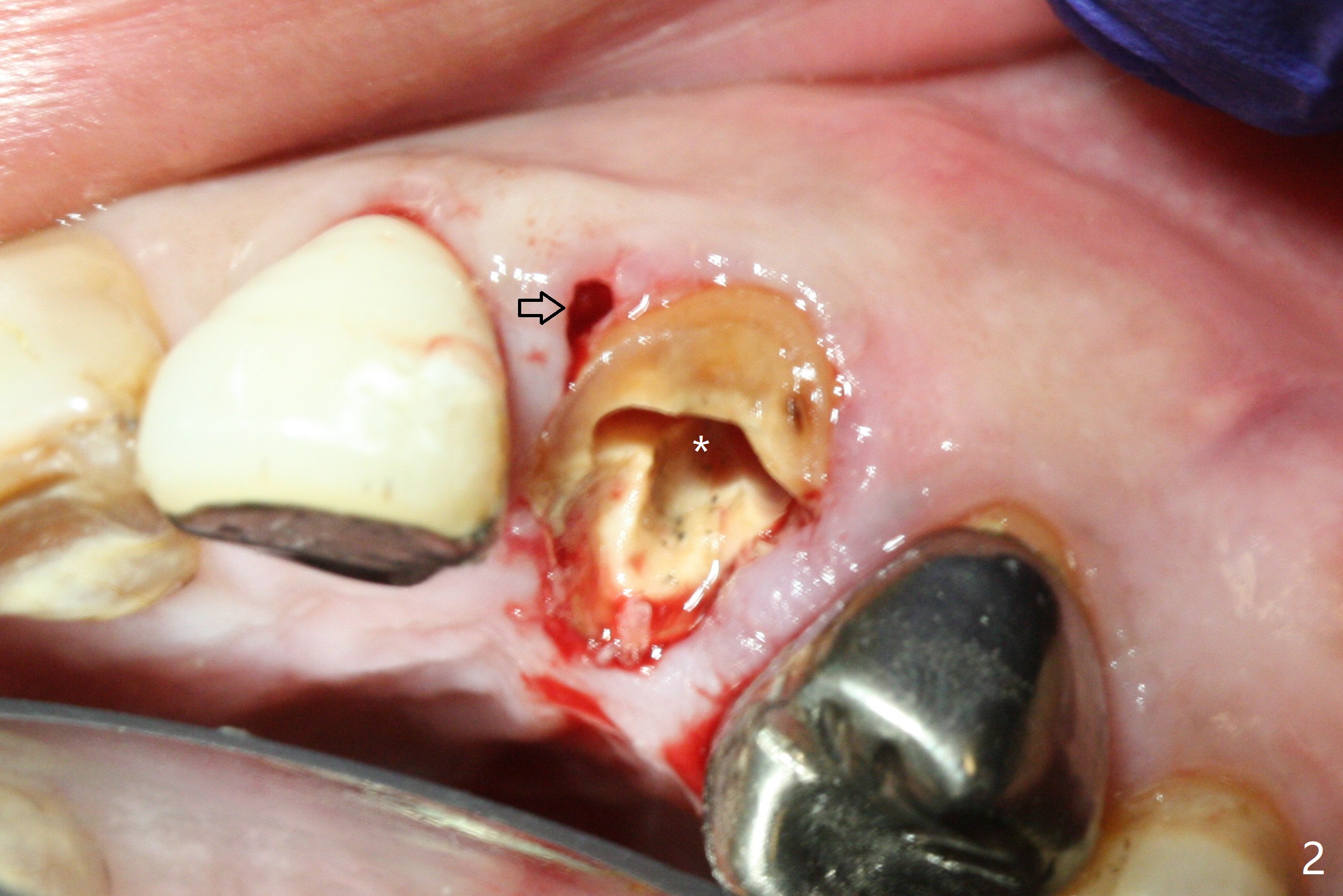
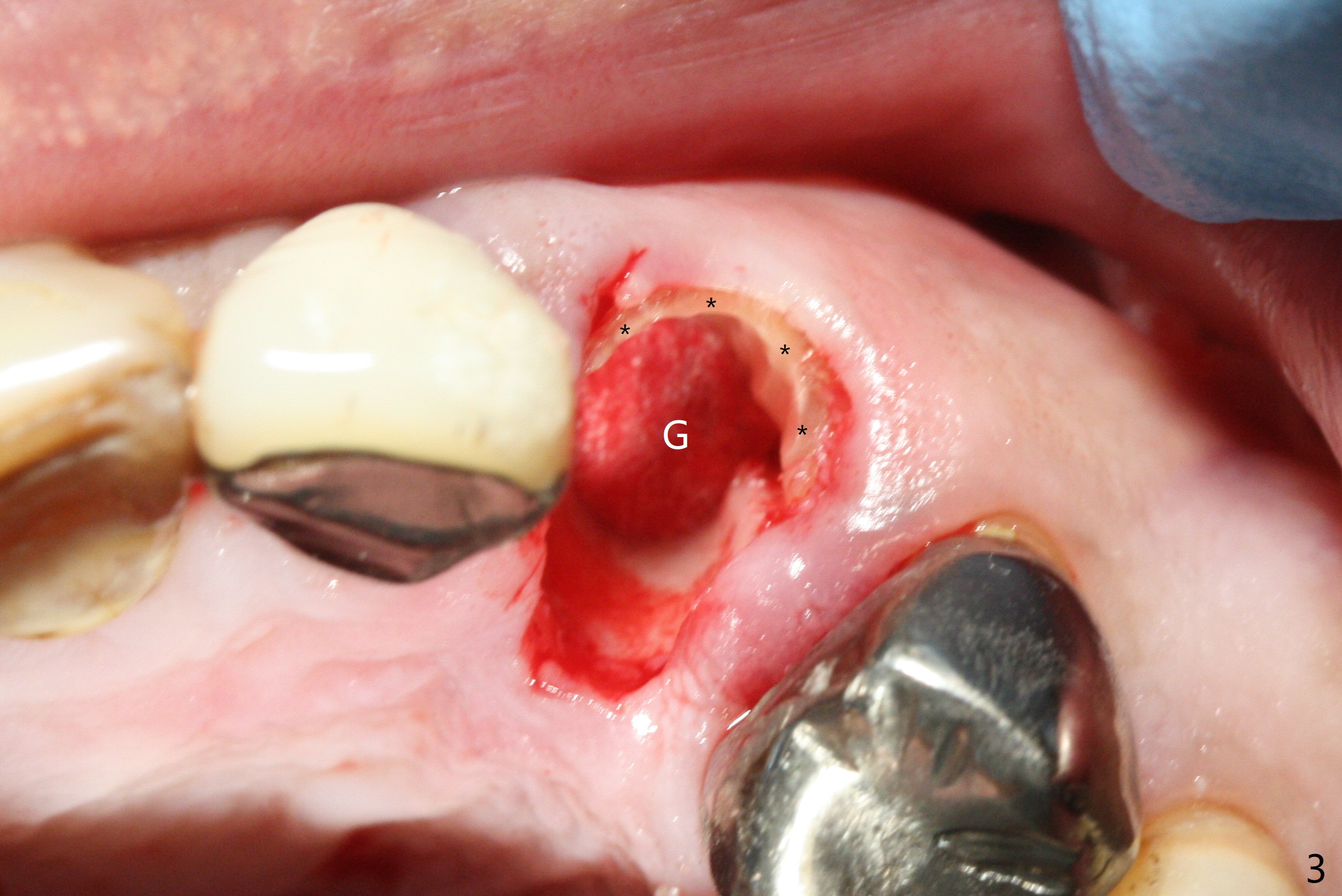
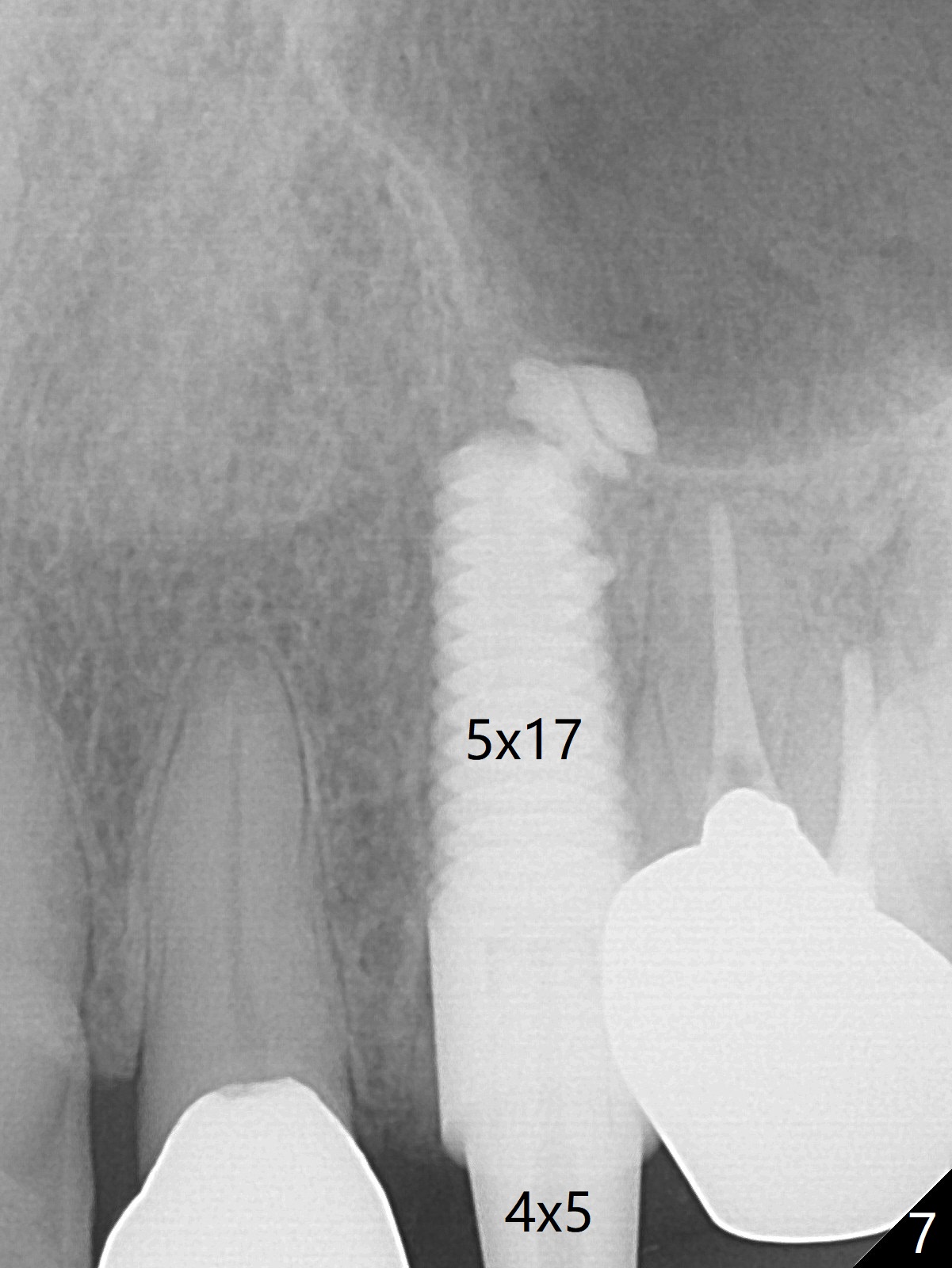
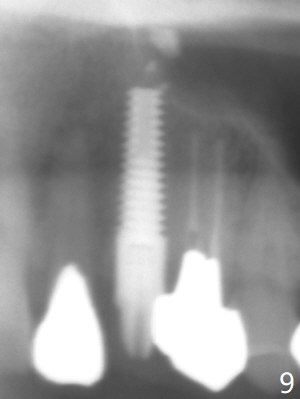
Socket Shield for Canine I
Extraction of the residual root at #11 (Fig.1) turns out to be difficult (Fig.2 (arrow: after use of small elevator). The tooth is sectioned (Fig.2 *); the palatal portion is removed, while the buccal one is trimmed until new moon-shaped and sub-gingival (Fig.3 * (gauze (G) packed in the socket while photo taking)). Initial osteotomy is 20 mm deep with nasal floor perforation (Fig.4). The subsequent depth is 17 mm (Fig.5). When a 5x17 mm tissue-level implant is placed (Fig.6,7; >60 Ncm), there is a gap between it and the socket shield (Fig.6 *). Gap-filling Vera Graft (Fig.8 *) also covers the shield prior to fabrication of an immediate provisional (Fig.9). There is no apparent bone loss 3.5 months postop (Fig.10). There is no buccal plate resorption 9 months postop (Fig.11). The implant is doing well 2 years postop (1 year 9 months post cementation, Fig.12).
Return to
Upper Canine
Immediate Implant,
IBS
Xin Wei, DDS, PhD, MS 1st edition 09/19/2017, last revision 03/14/2020