
|
|
|
|
|
|
|
|
|
|
||
Implants in Wide Crest
The bone at the sites of #3 and 5 is wide with wide keratinized gingiva. A 4 mm tissue punch is used for access. When a 8 mm long pilot drill is being used at #3, there is empty feeling. A parallel pin protrudes into the sinus (Fig.1). Nose blowing test or CAS kit hydrolic lifter does not reveal sign of sinus membrane perforation.
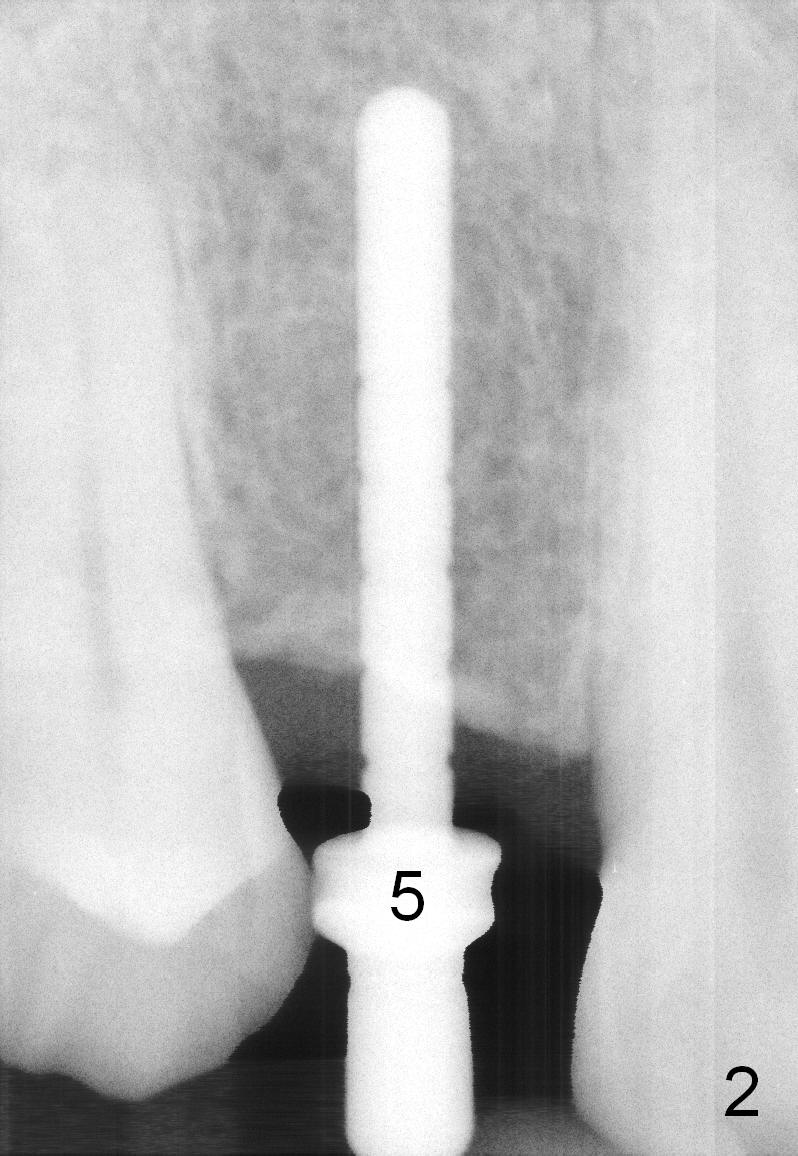
There is more apical bone when a 12 mm long parallel pin is inserted at #5 (Fig.1,2). The bone density is not high. The site of #5 is under prep (3.8x14 mm) for a 4.1x14 mm implant (Fig.3; > 50 Ncm).
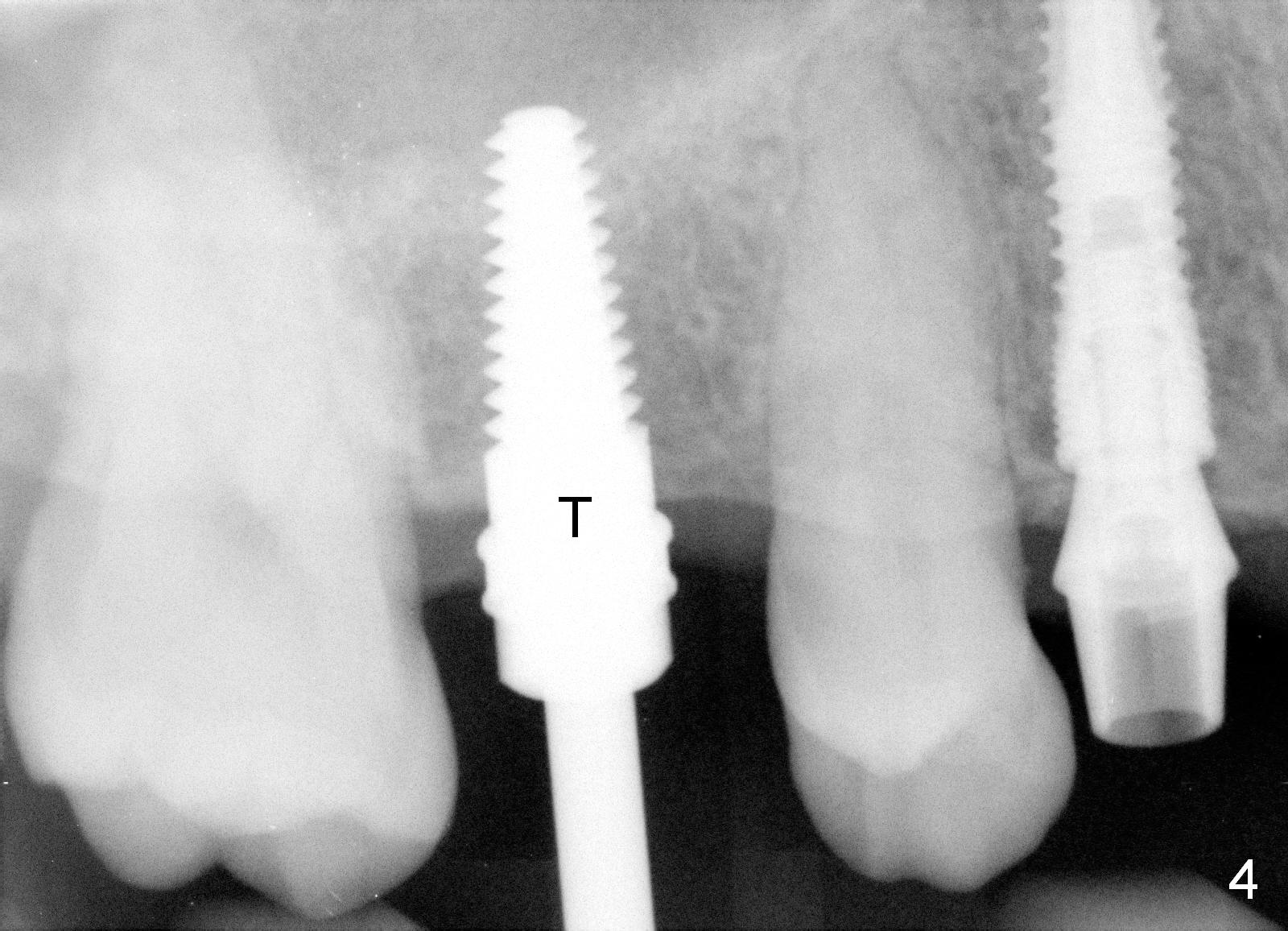
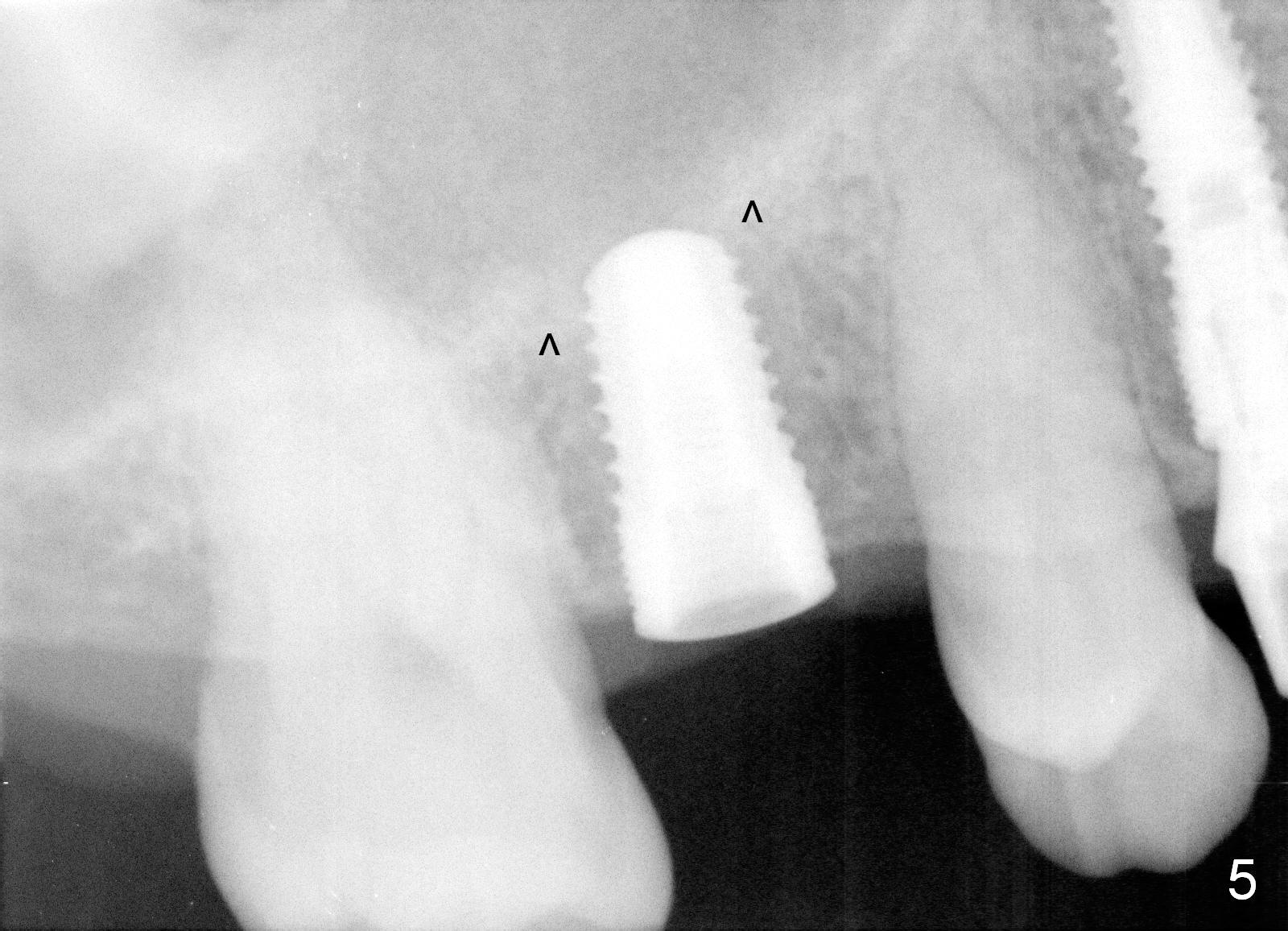
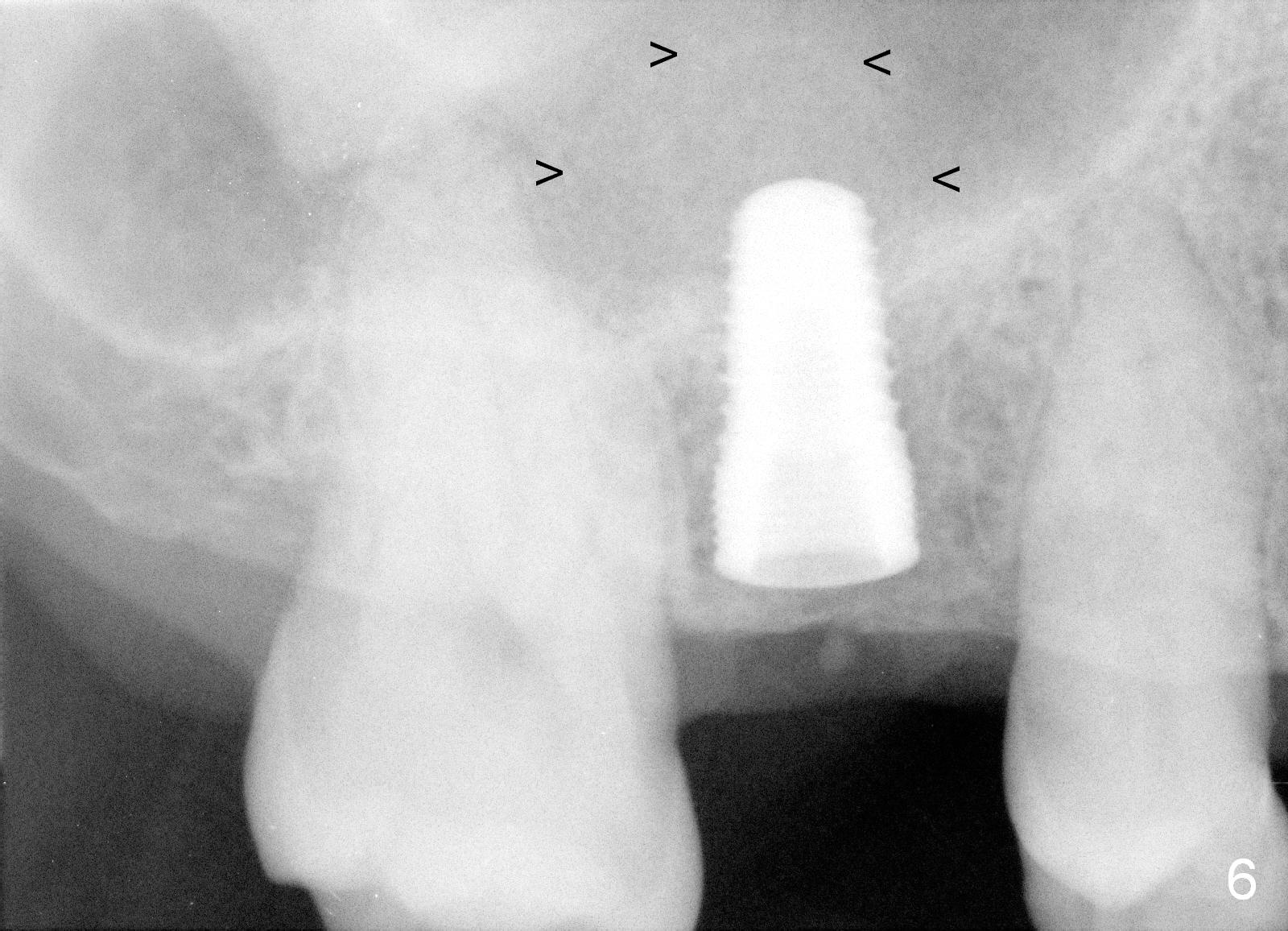
CAS kit is used for sinus lift, followed by insertion of 4.5x14 mm tap for 11 mm (Fig.4). After using 5x14 mm tap at 11 mm, a 5.3x10 mm SM implant is placed (Fig.5). It is not completely seated and spinning with low insertion torque (<35 Ncm). It appears that the sinus floor penetration is not wide enough for implant placement. After reuse of 4.5 and 5x14 mm taps at 14 mm, the SM implant is seated with insertion torque of 35 Ncm (Fig.6) with sign of sinus lift (arrowheads (autogenous bone, allograft and Osteogen)).
Probably due to subcrestal placement, there is no bone loss 4.5 months postop (Fig.7). Equi-crestal placement may be associated with thread exposure.
Return to Upper Premolar Immediate Implant
#9
Xin Wei, DDS, PhD, MS 1st edition 12/09/2015, last revision 02/27/2018