,%20later%20changed%20to%204.5x4(4)%20for%2012,%204.5x4(5)%20at%2013.jpg)
|
|
|
|
|
|
|
|
|
|
||
Low Stability
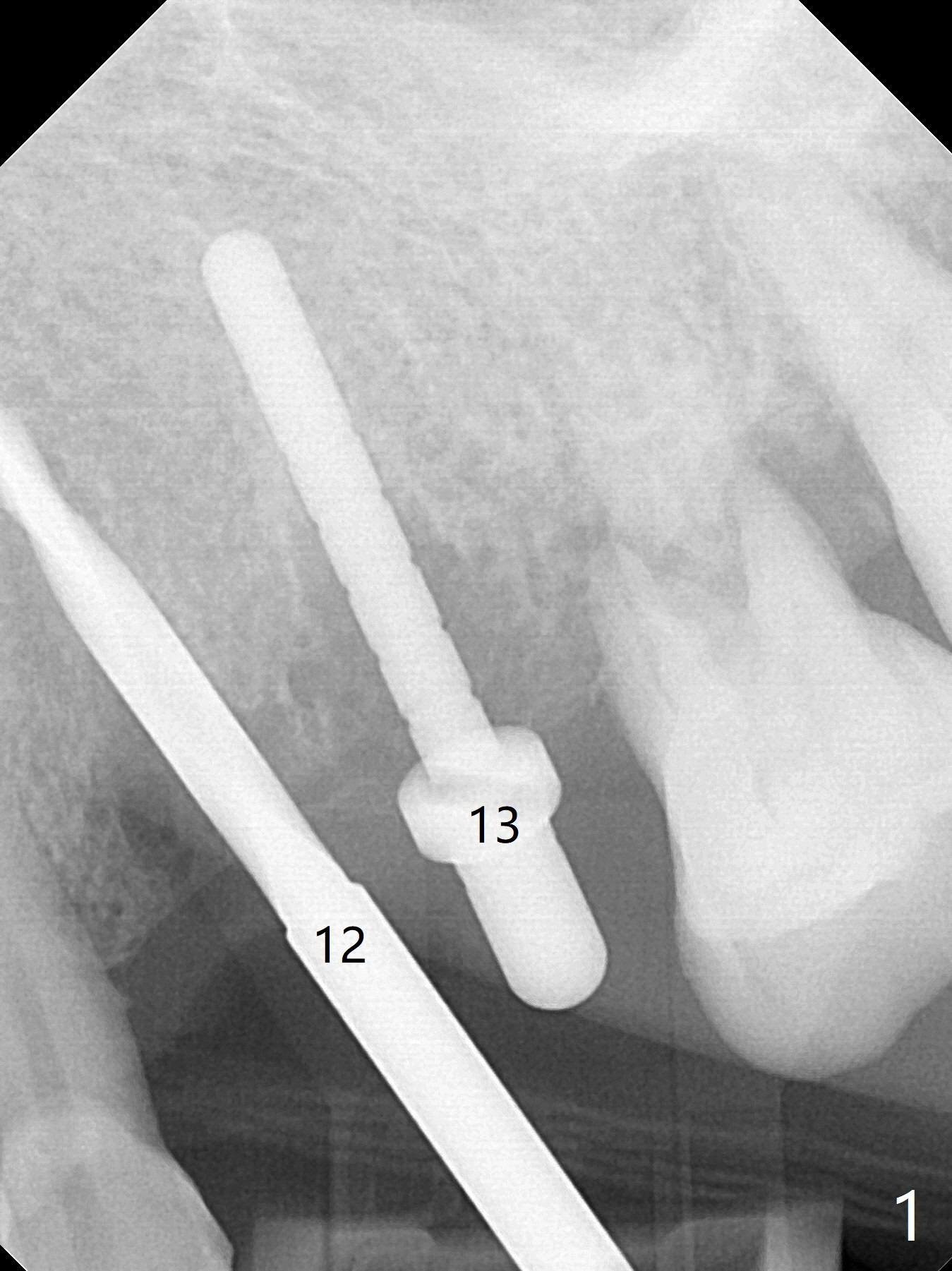
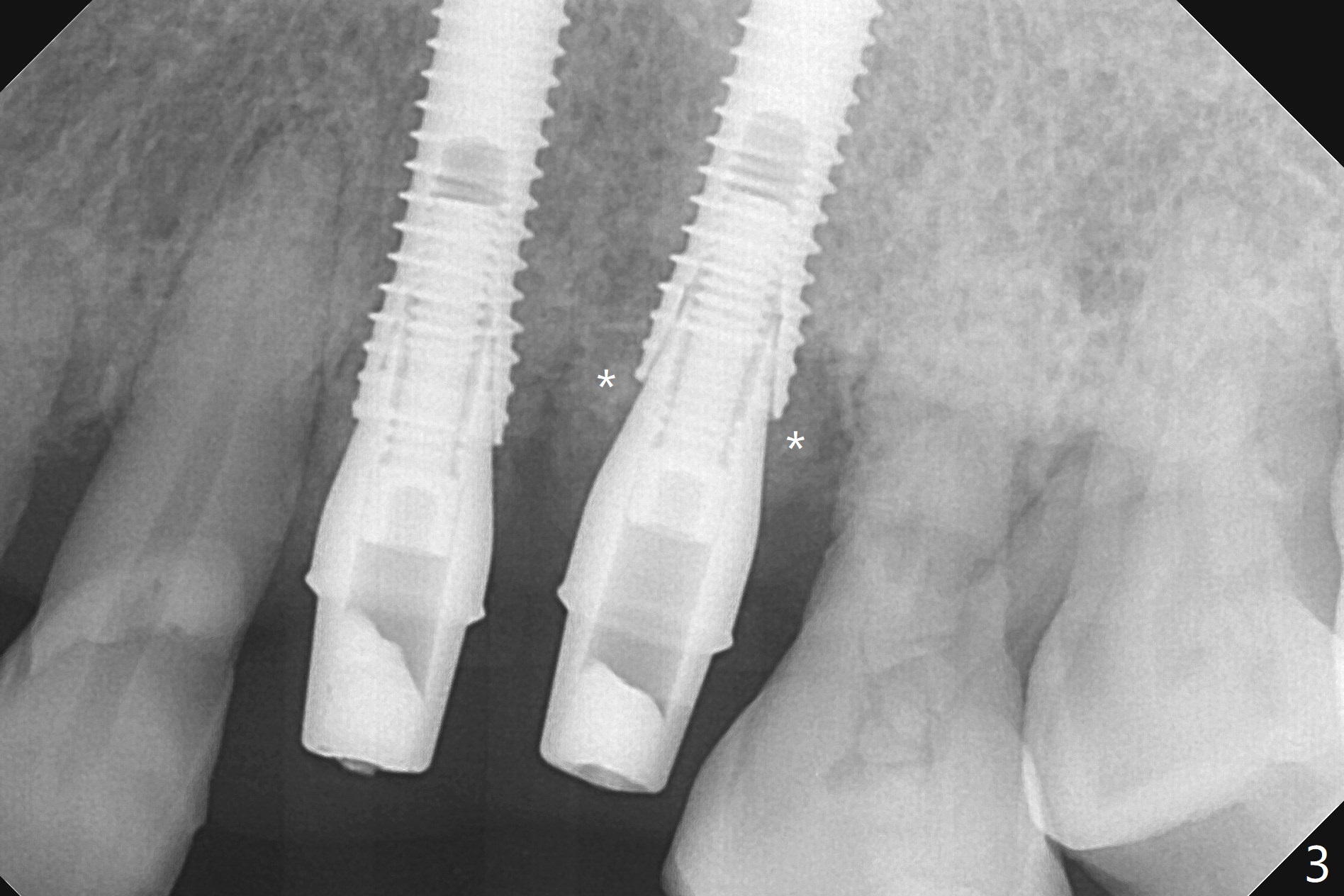
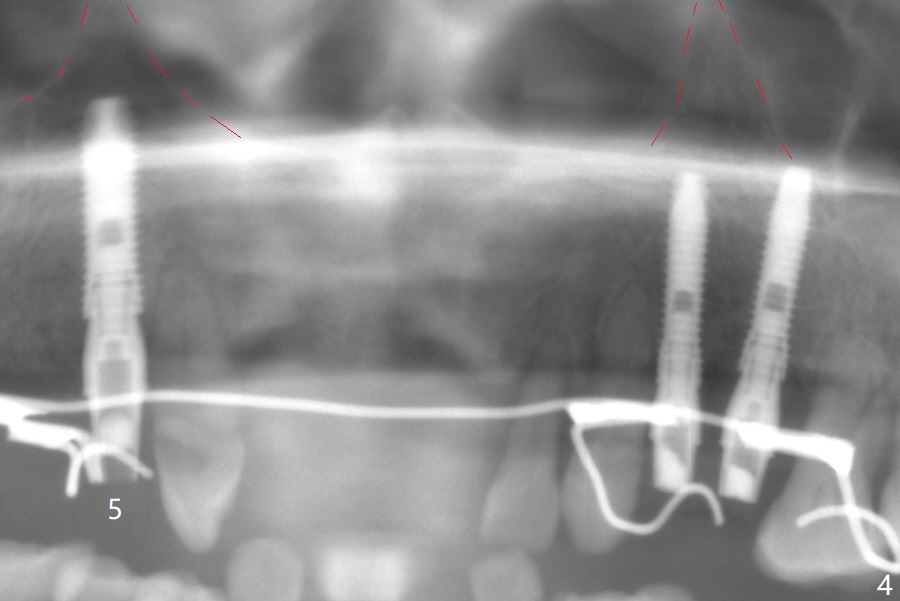
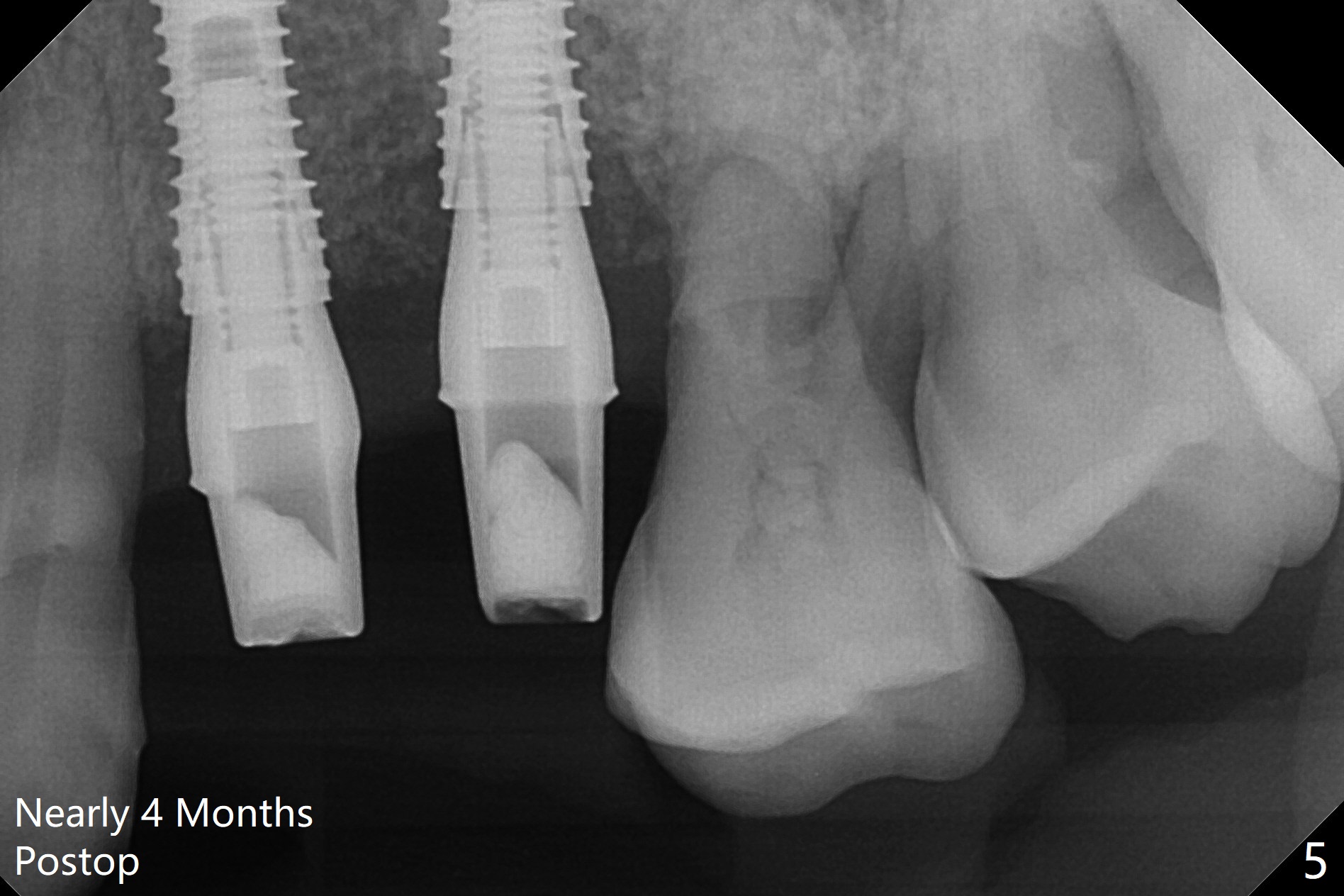
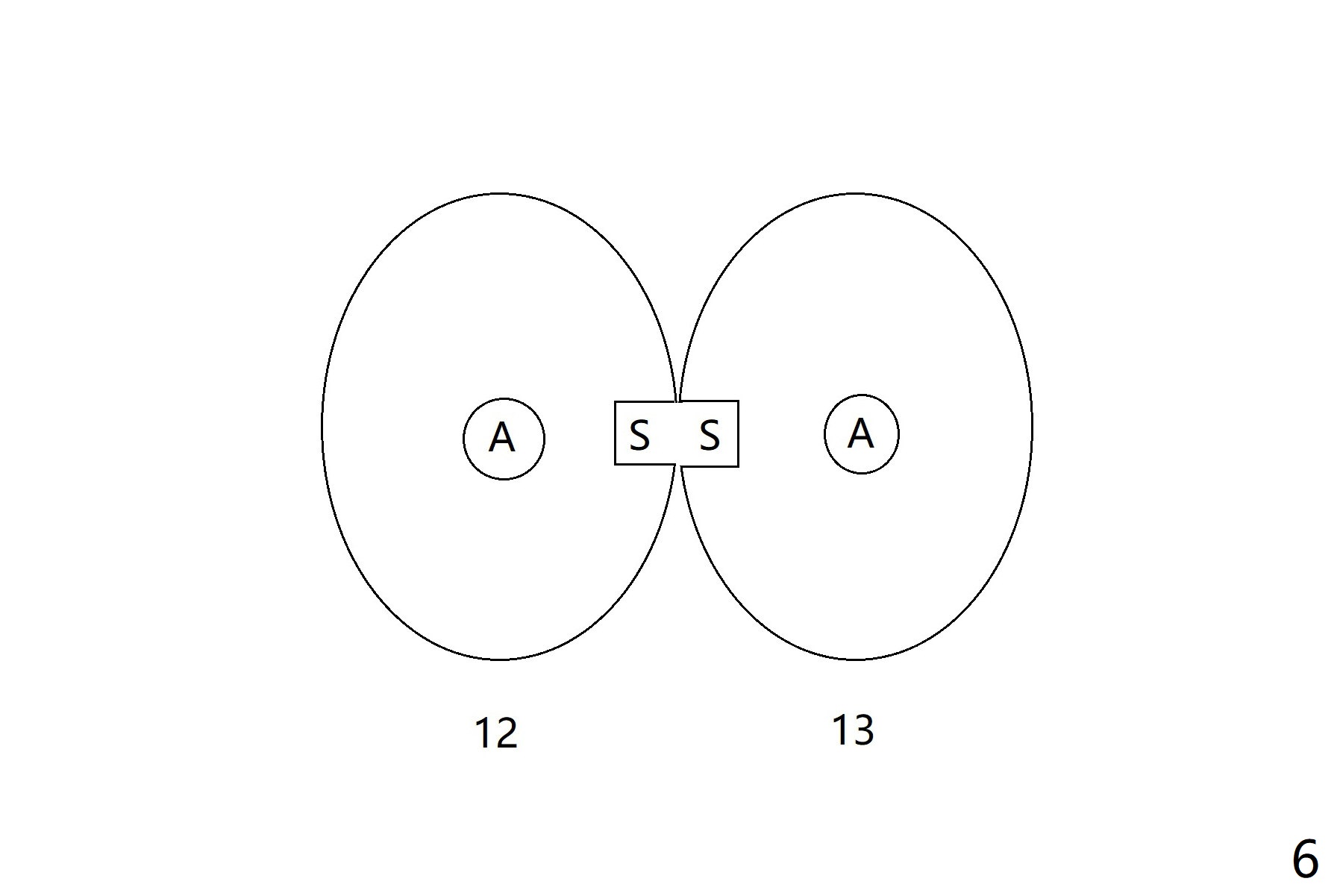
A 66-year-old woman returns to office requesting implant placement at #12 and 13 at an appointment supposed for #5 impression. Depth of osteotomy is 20 mm (gingival level, Fig.1 ( 2mm)). After correction of trajectory at #12 and 3 mm drill for 16 mm at the sites, two of 3.8x16 mm implant are placed with insertion torques of 35 and 15 Ncm, respectively (Fig.2). Before and after change into shorter abutments (4.5x4(4) and (5)), Vera Graft is placed (Fig.3 *). To increase stability, either increase the diameter (4 (Fig.4 at #5) or 4.5 mm instead of 3.8) or length of the implants (red dashed line: sinus floor). Or use dummy implants. The allograft appears to have been incorporated into the host bone nearly 4 months postop (Fig.5). The abutment of the isolate implant at #5 becomes loose twice (Fig.4). To reduce the chance of abutment loosening at #12 and 13, can you make splinted crowns? If the two separate crowns have been fabricated, can you make a slot (with light undercut) in the proximal area of each crown (Fig.6 (occlusal view): S) in addition to access hole (A)? After cementation, composite will be placed in the slots (lock) so that the crowns will not rotate and become loose.
Return to
Upper Premolar Immediate Implant,
IBS,
Clindamycin
Xin Wei, DDS, PhD, MS 1st edition 10/13/2017, last revision 02/12/2018