,%20no%20graft.jpg)


.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Change in Trajectory
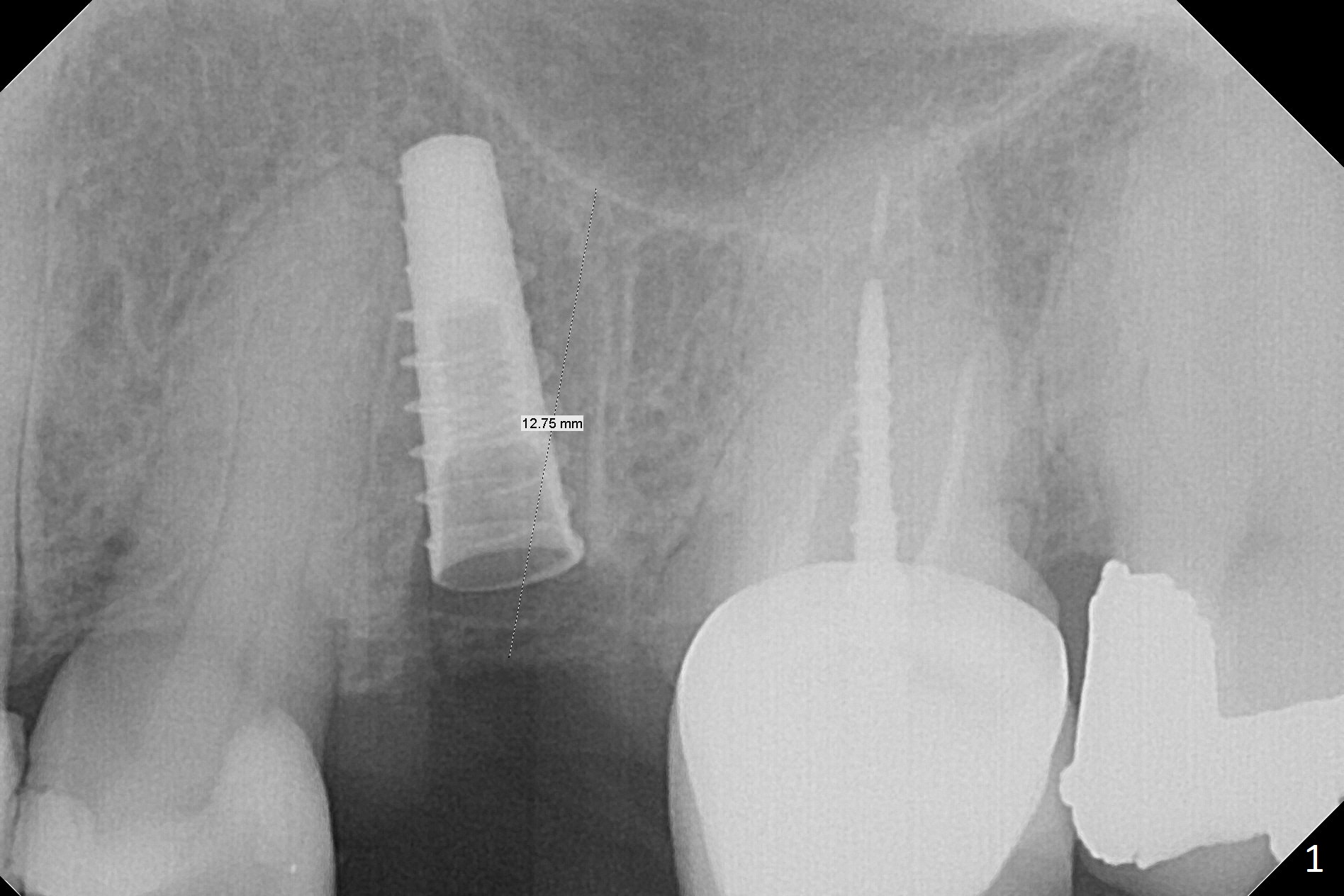
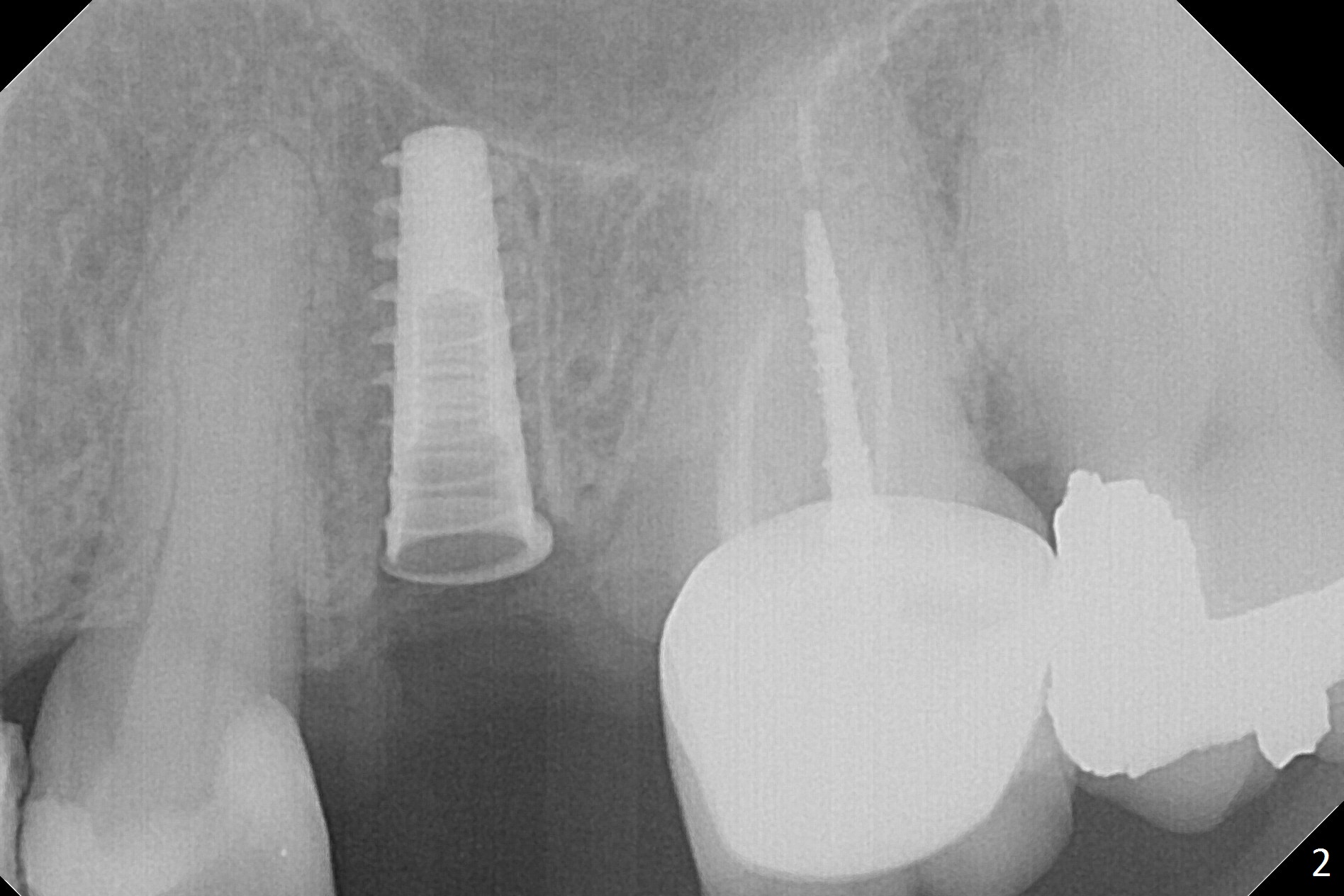
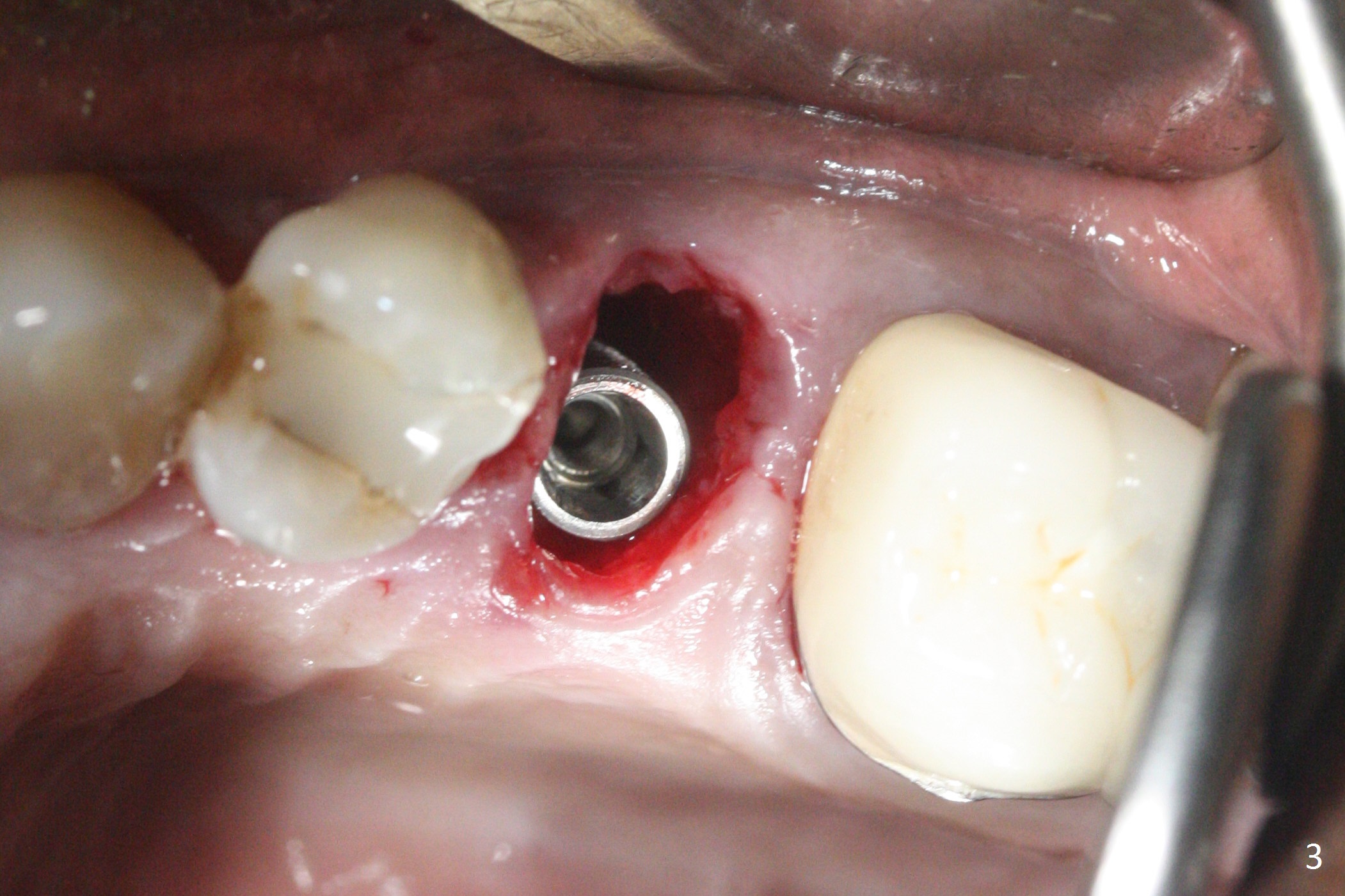
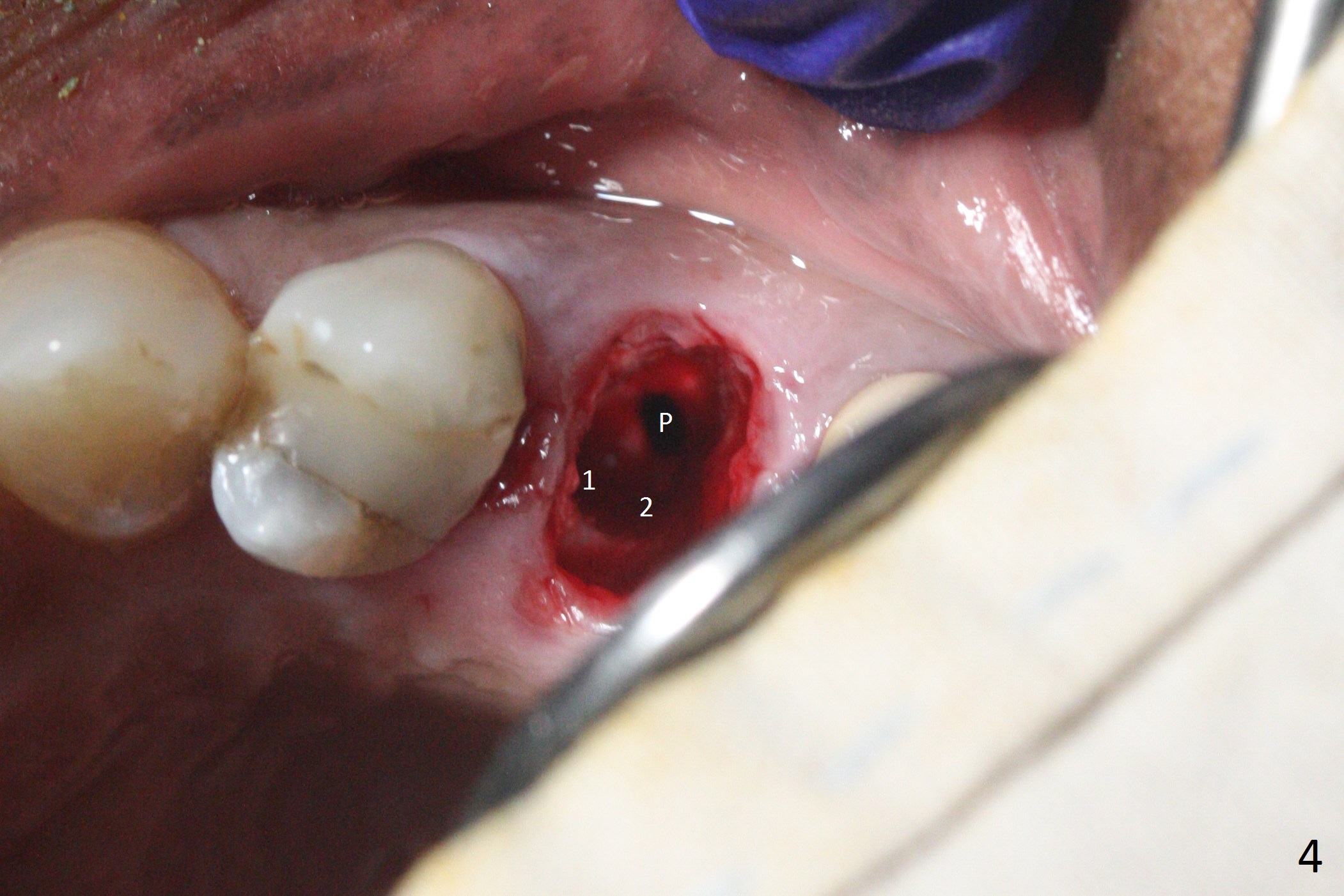
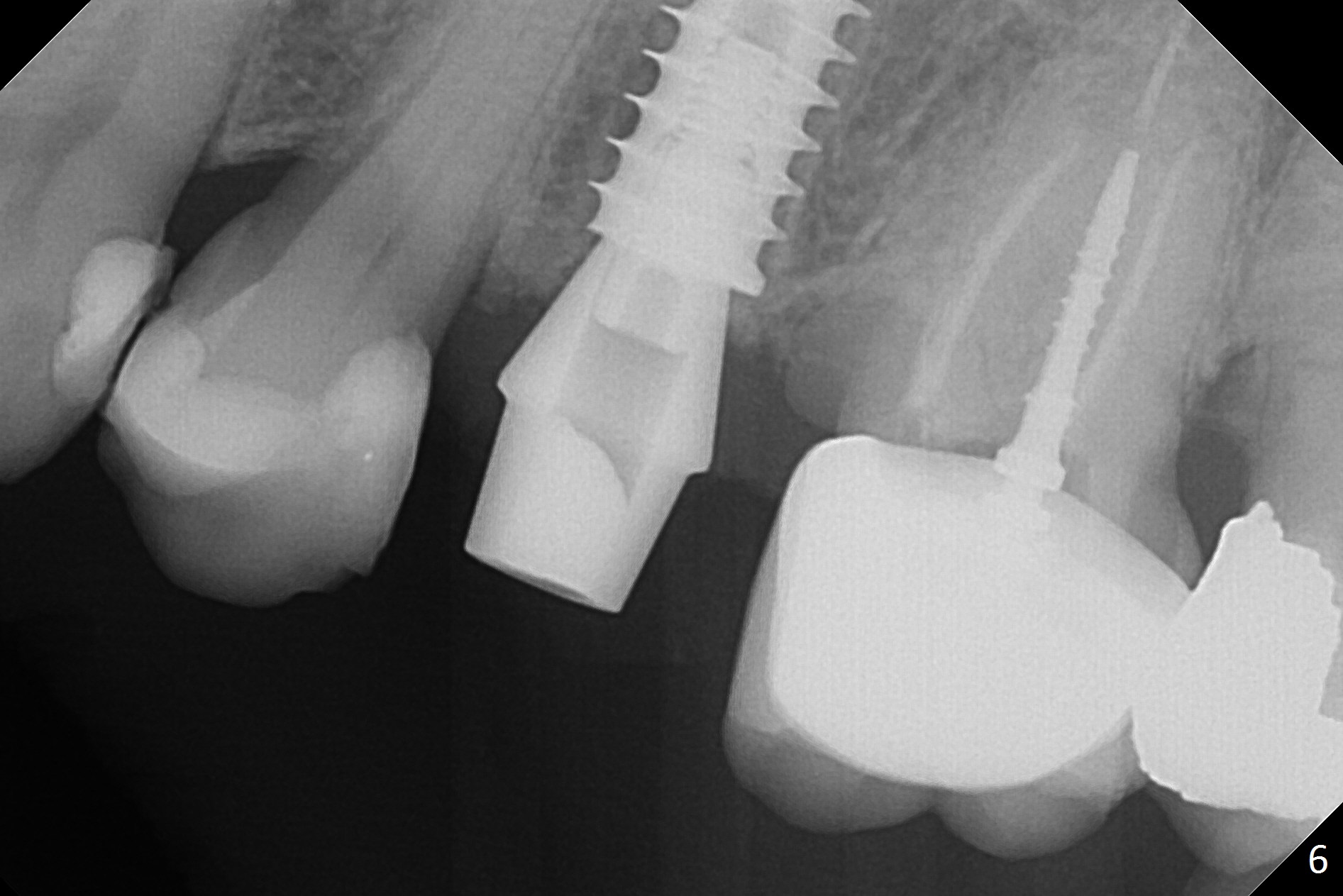
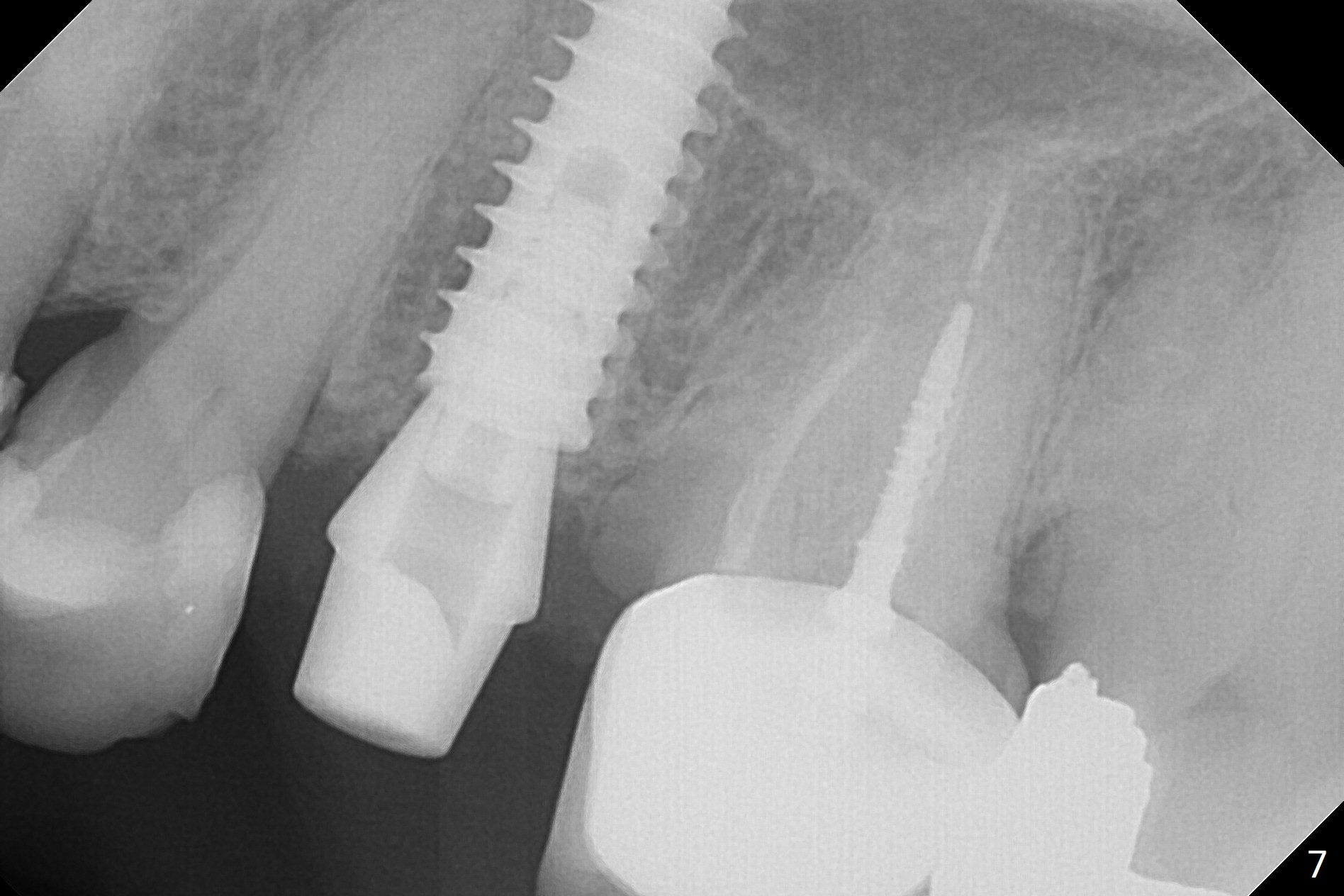
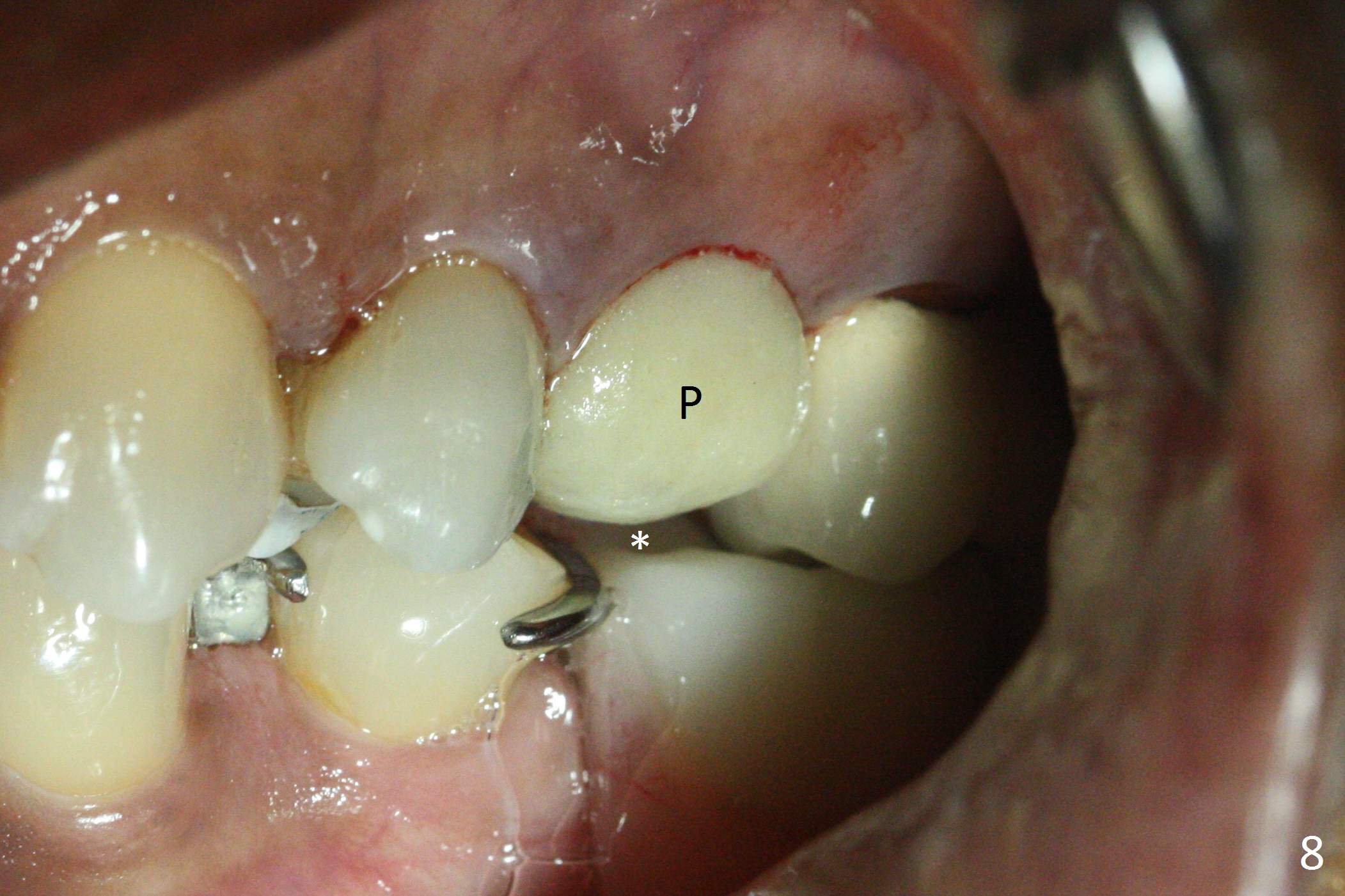
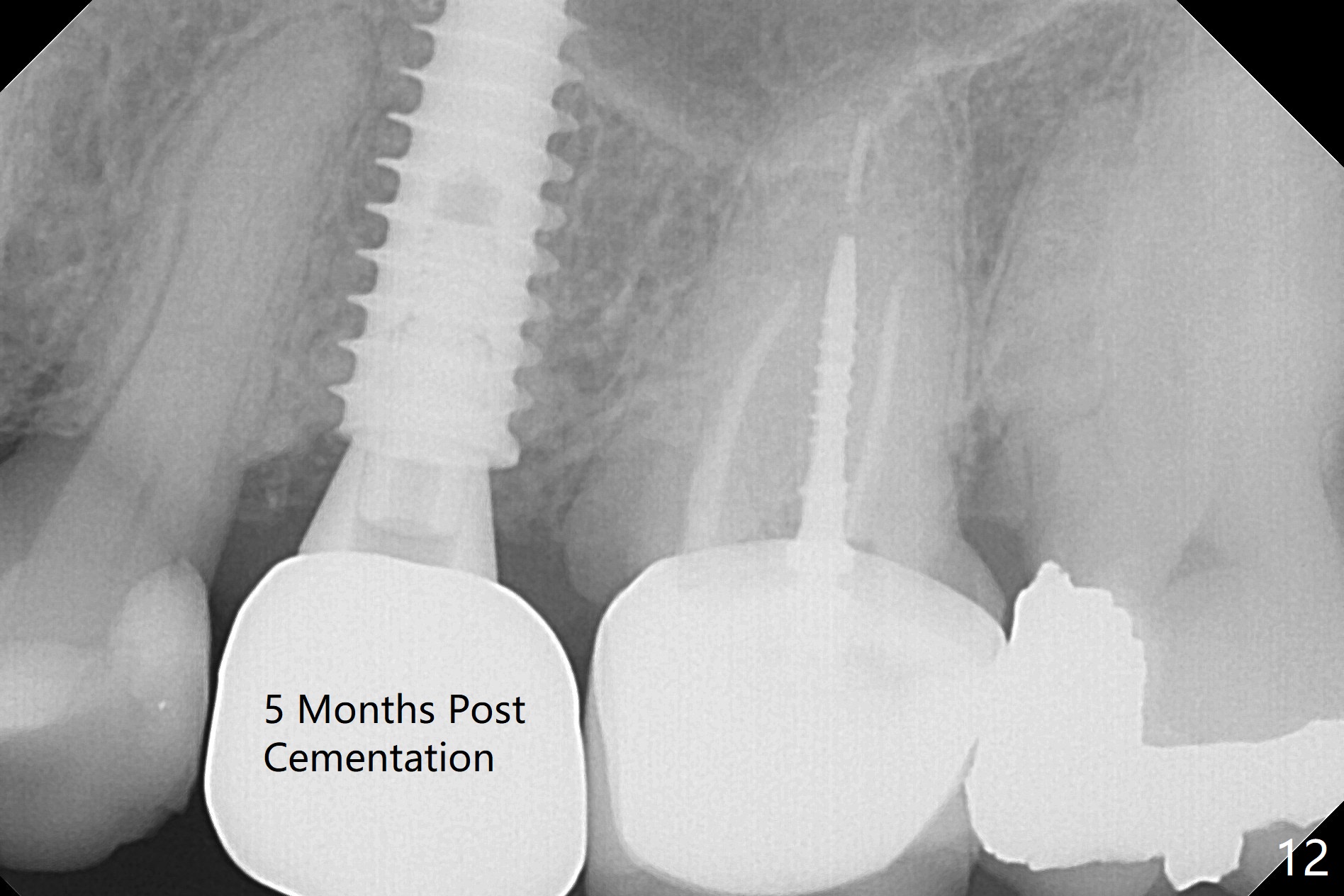
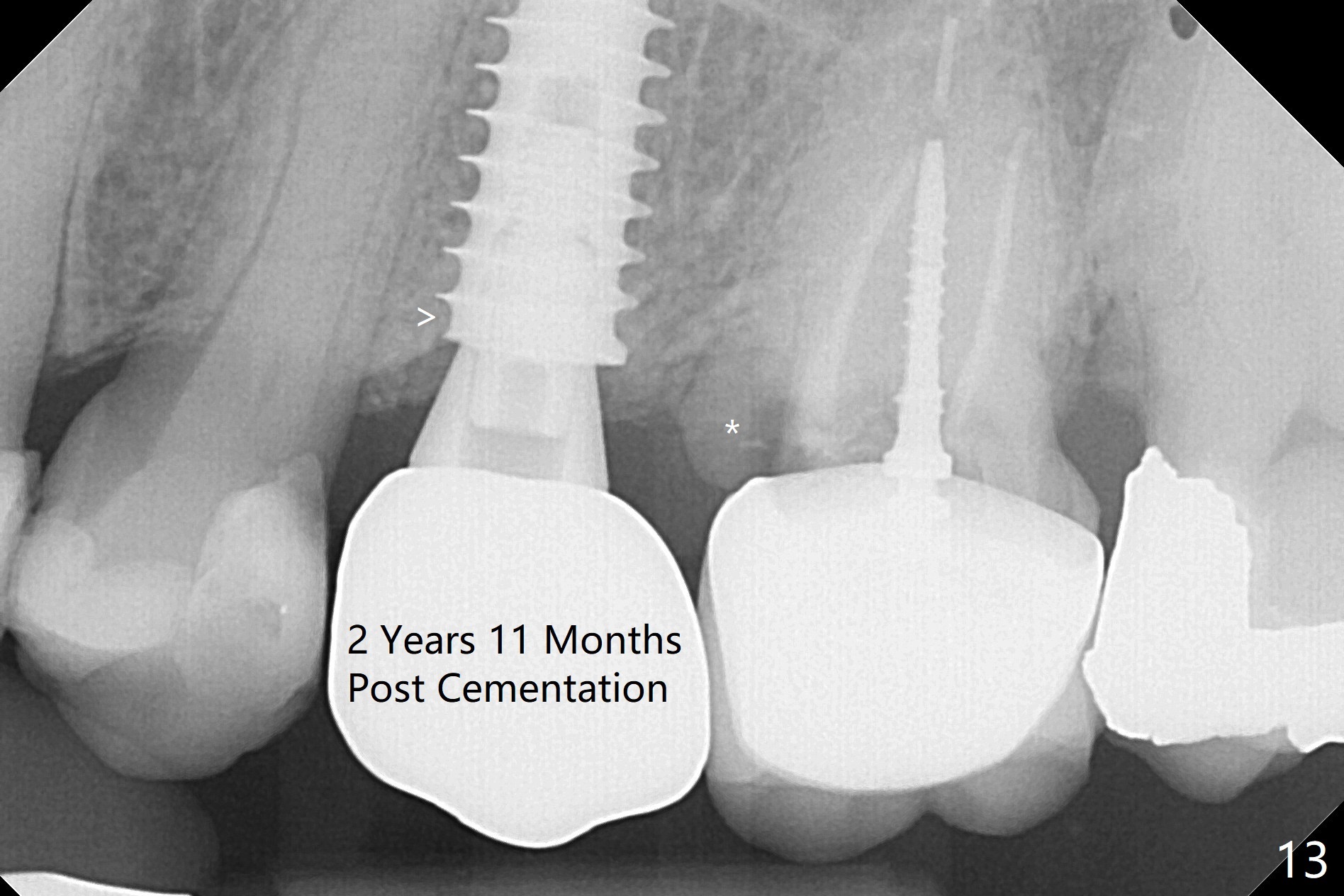
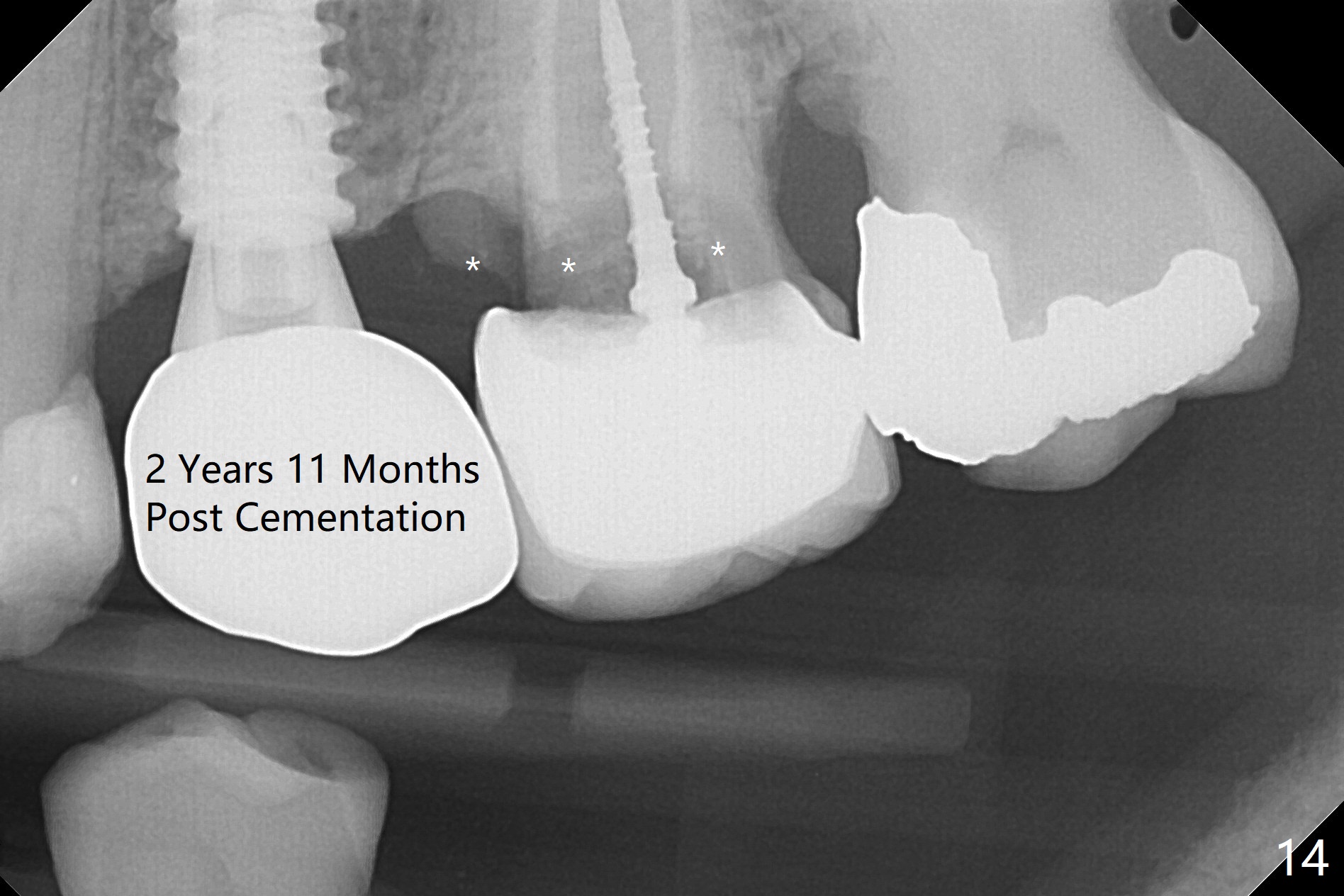
Since the apical native bone is limited at #13 after extraction, no PA is taken until a 4x11 mm dummy implant is placed after 1.6 mm and 3.3 mm drills for 13 mm (Fig.1). After using Lindamann bur to move the osteotomy distal and reusing 3.3 mm drill, the trajectory of a 4.5x11 mm IBS dummy implant improves (Fig.2,3 with low stability). When the implant is removed, the buccal portion of the socket is found to be perforated (Fig.4 P). Although the reason for the perforation is unknown, it is repaired by insertion of a piece of PRF plug, followed by allograft. #1 and 2 in Fig.4 represent the 1st and 2nd osteotomies, as shown in Fig.1 and 2, respectively. The trajectory of the final 5x13 mm implant is acceptable (Fig.5-7, different angulations), so is insertion torque (45 Ncm). After placing a 5.5x4(4) mm abutment, an immediate provisional is fabricated (Fig.8 P) with occlusal clearance (*). The interdental papillae remain in place 12 days postop (Fig.9 *). There is no sign of postop sinus infection. The provisional is loose 18 days postop; the abutment is changed to 5x4(3) mm (Fig.10). It is difficult to catch the mesial margin of the abutment for impression 4 months postop, due to poor oral hygiene and the short cuff (3 mm, Fig.11). The appointment for impression is rescheduled with emphasis on oral hygiene and no wearing the provisional for a few days prior to next appointment. Bone has grown into the space between the 1st and 2nd threads 5 months post cementation (Fig.12) and the bone is normal, solid and dense 2 years 11 months post cementation (Fig.13 >). There is mesial open margin of the tooth #14 (Fig.13,14 *).
Return to
Upper
Premolar Immediate Implant
MAGIC
FC 植入方法
Chinese
7
手术
29
Xin Wei, DDS, PhD, MS 1st edition 05/01/2017, last revision 12/12/2020