


|
|
|
|
|
|
|
|
|
|
Depth of Osteotomy through Gingiva
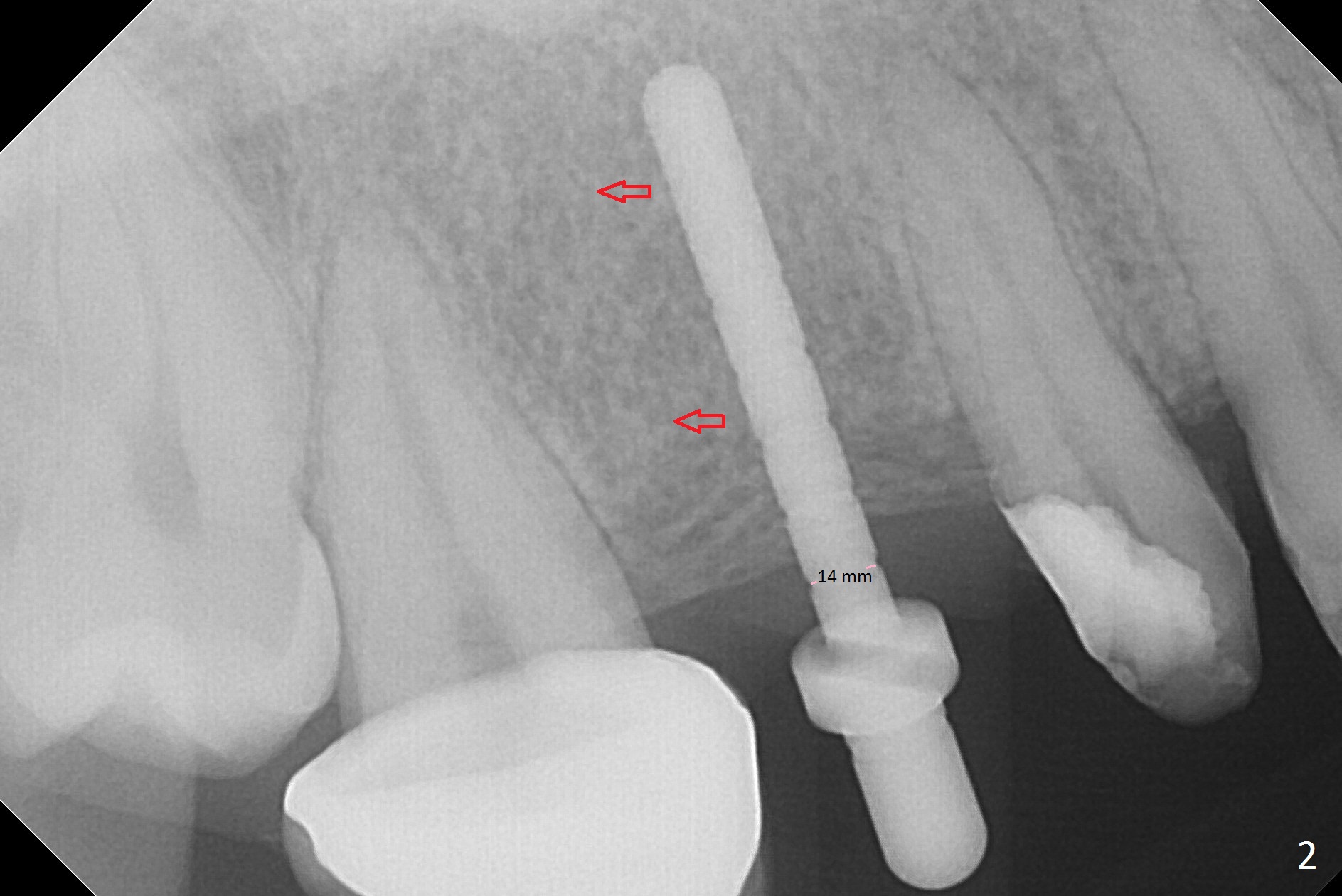
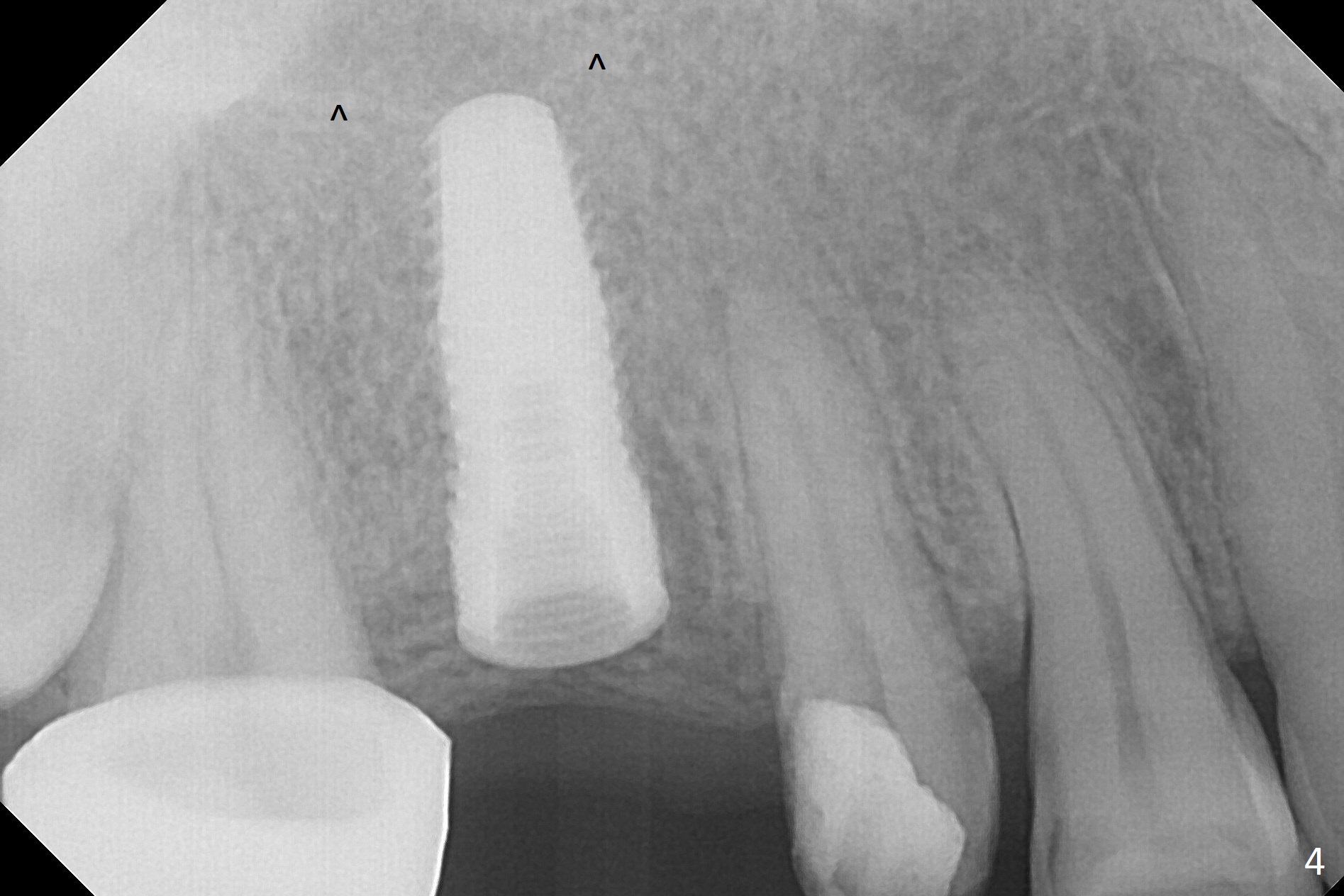
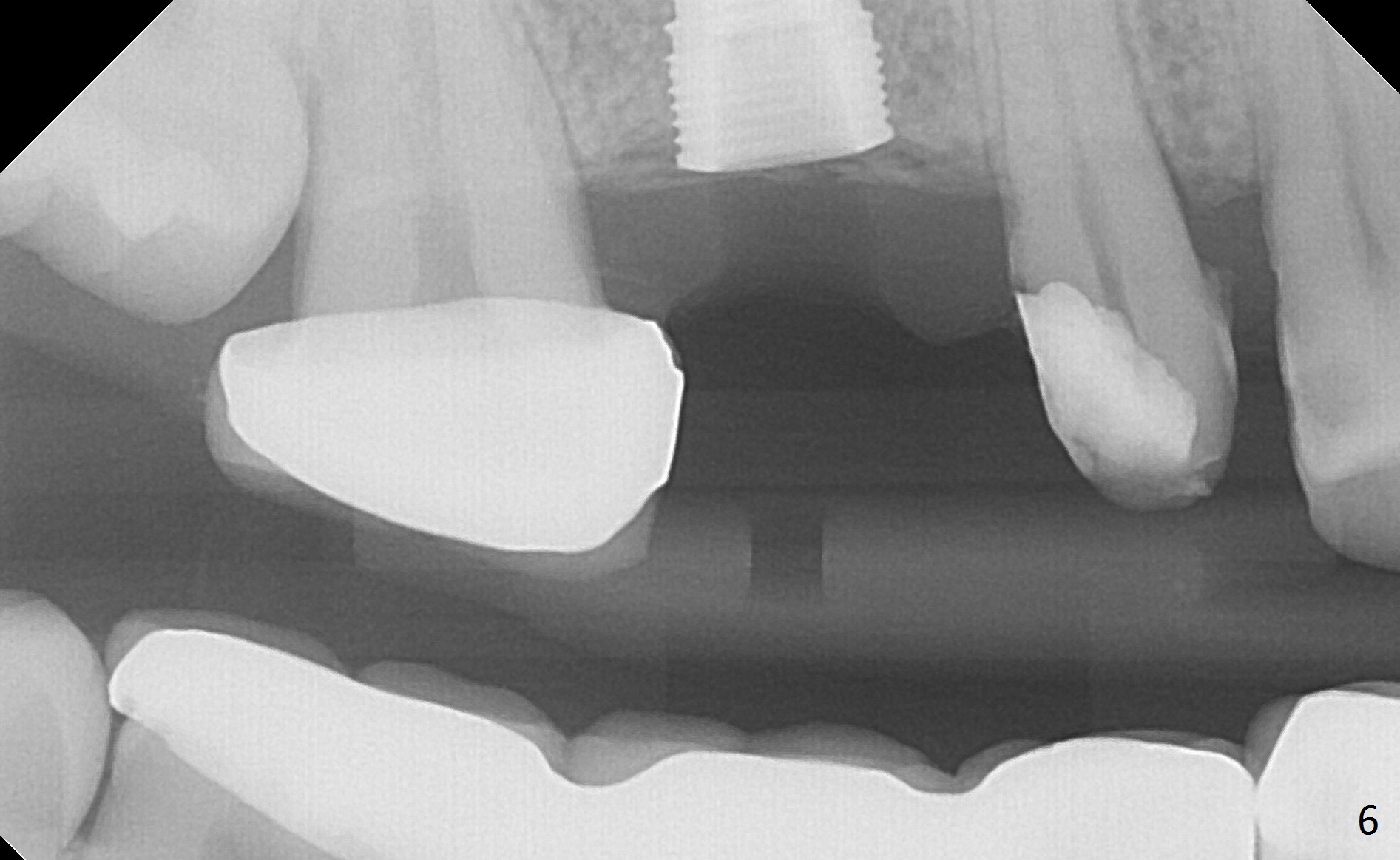
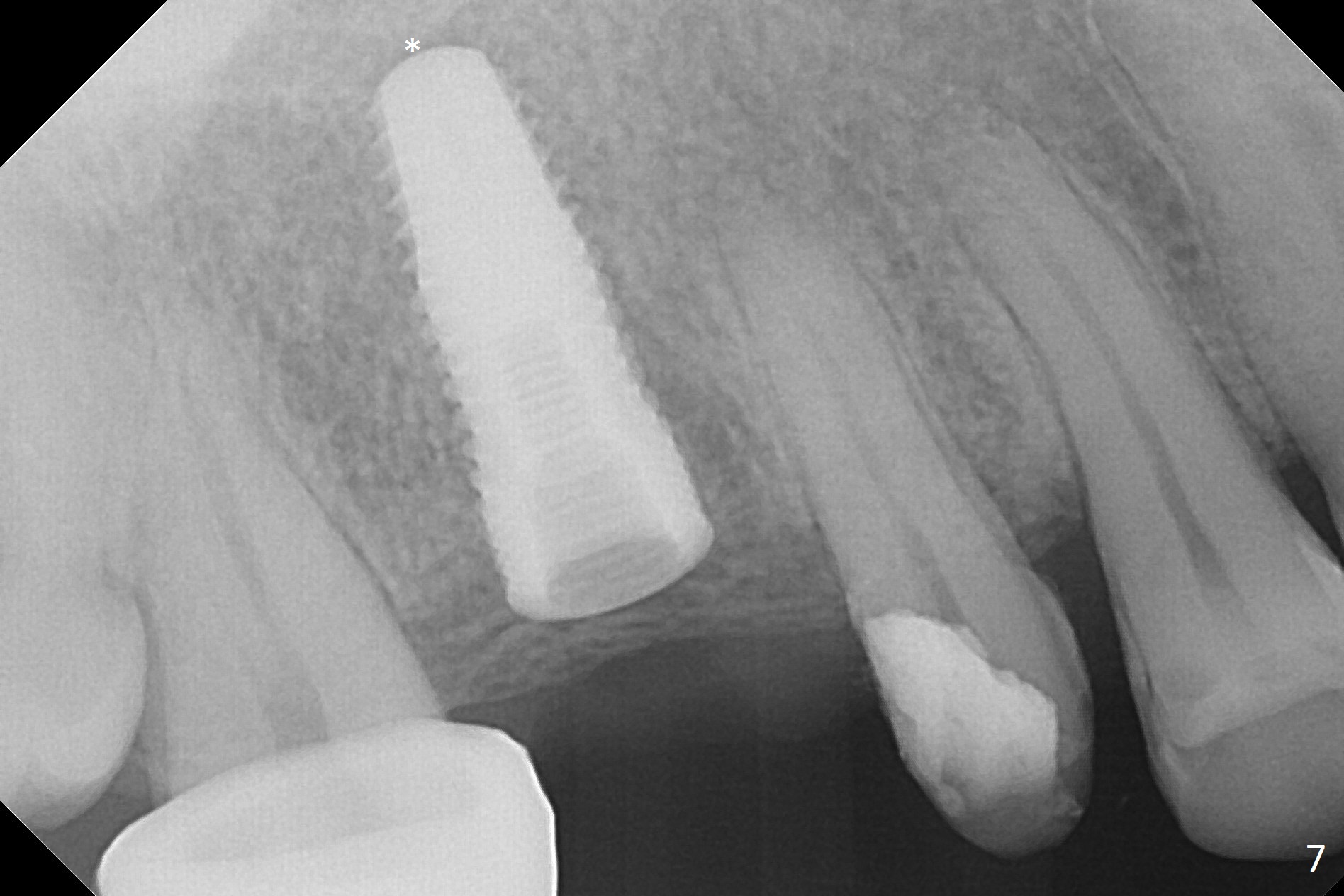
When the bridge is partially removed, the tooth #4 is found to have extensive caries. IRM is placed following carious removal (Fig.1). Magic Split testing shows that the bone density is high (flapless). Osteotomy is initiated by 1.6 mm drill, but the handle of the drill needs to shift mesial (Fig.1 red arrow). When the latter is done, the whole drill (2 mm) needs to move distal (Fig.2 double red arrows). When a 4.5x14 mm drill finishes the osteotomy, it is in the middle of the edentulous space (Fig.3). After use of 5 mm tap, a 5.3x14 mm implant cannot reach the depth (Fig.4,5). Following increase in osteotomy depth from 16 to 18 mm (gingival margin) until 5 mm drill in diameter, the implant placement level is more ideal (Fig.6,7, slightly subcrestal) with insertion torque maintaining at >55 Ncm. The sinus floor (Fig.4 arrowheads) may be penetrated when the osteotomy depth increases (Fig.7 *), but the sinus membrane remains intact.
In brief, osteotomy depth using flapless approach should be 4 mm more than the intended implant length (2 mm for gingival thickness and 2 mm for complete implant seating).
Return to
Upper
Molar Immediate Implant, IBS
Xin Wei, DDS, PhD, MS 1st edition 04/11/2017, last revision 04/11/2017