

,%204.5x4(2).jpg)
%20at%204.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
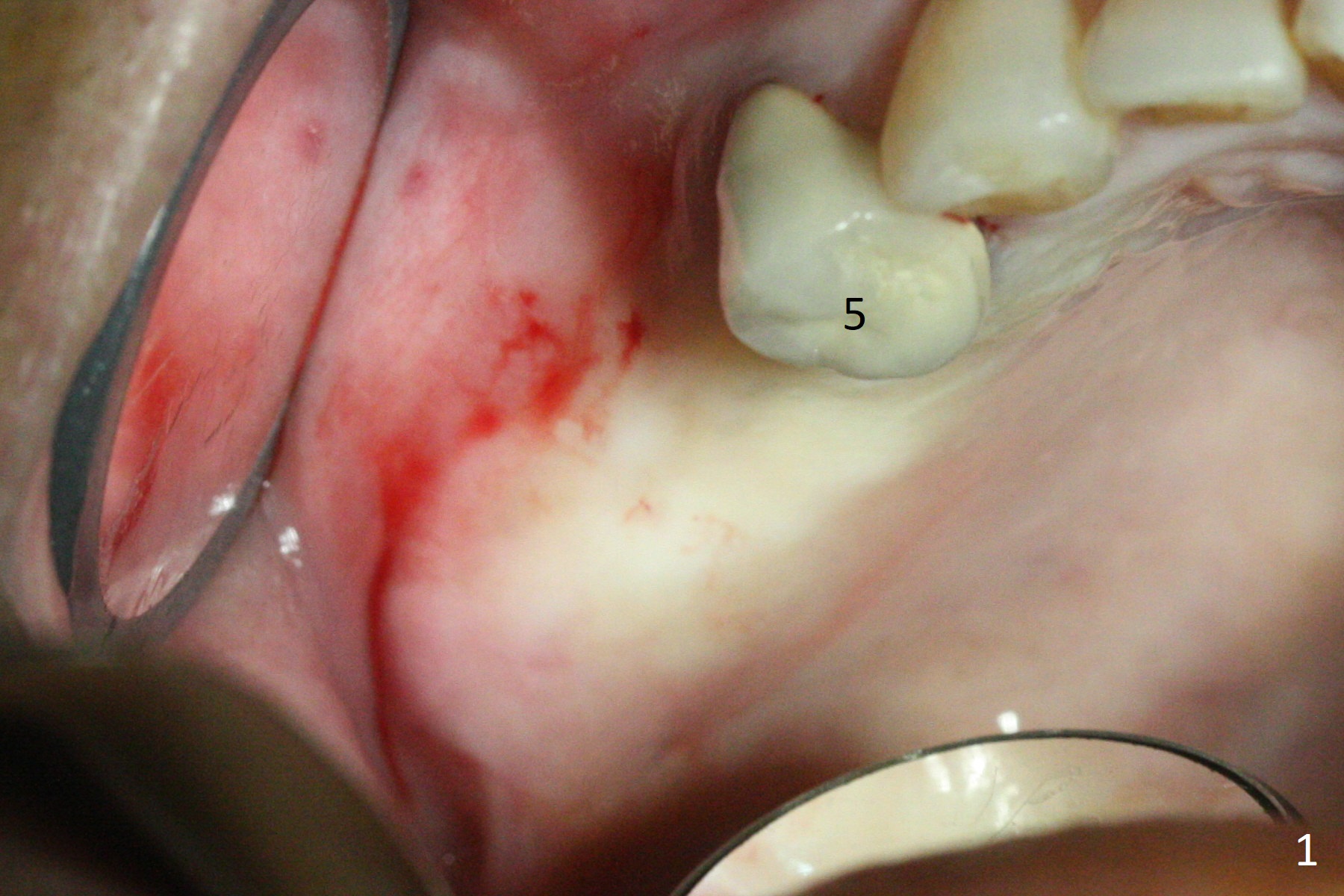
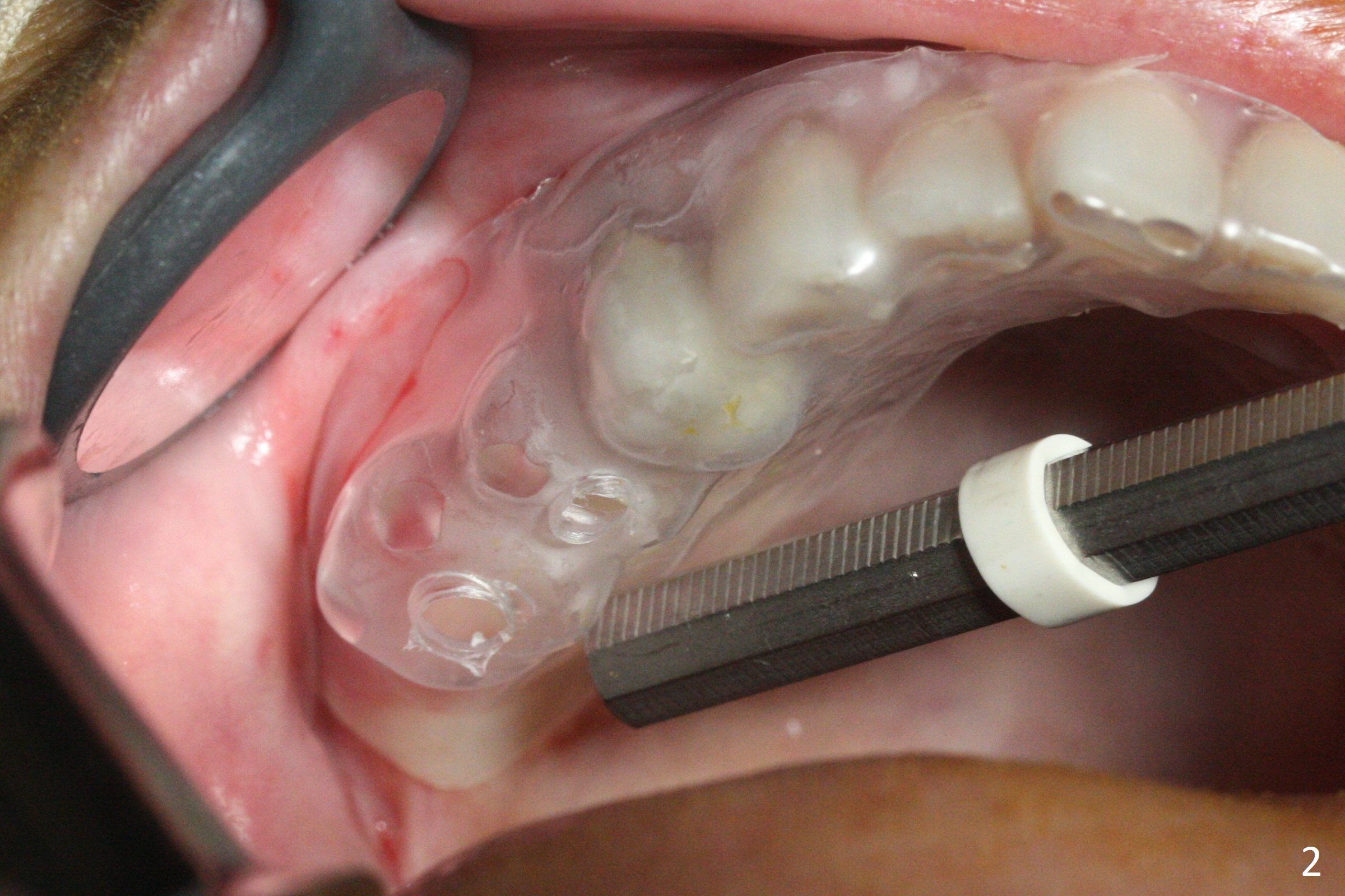
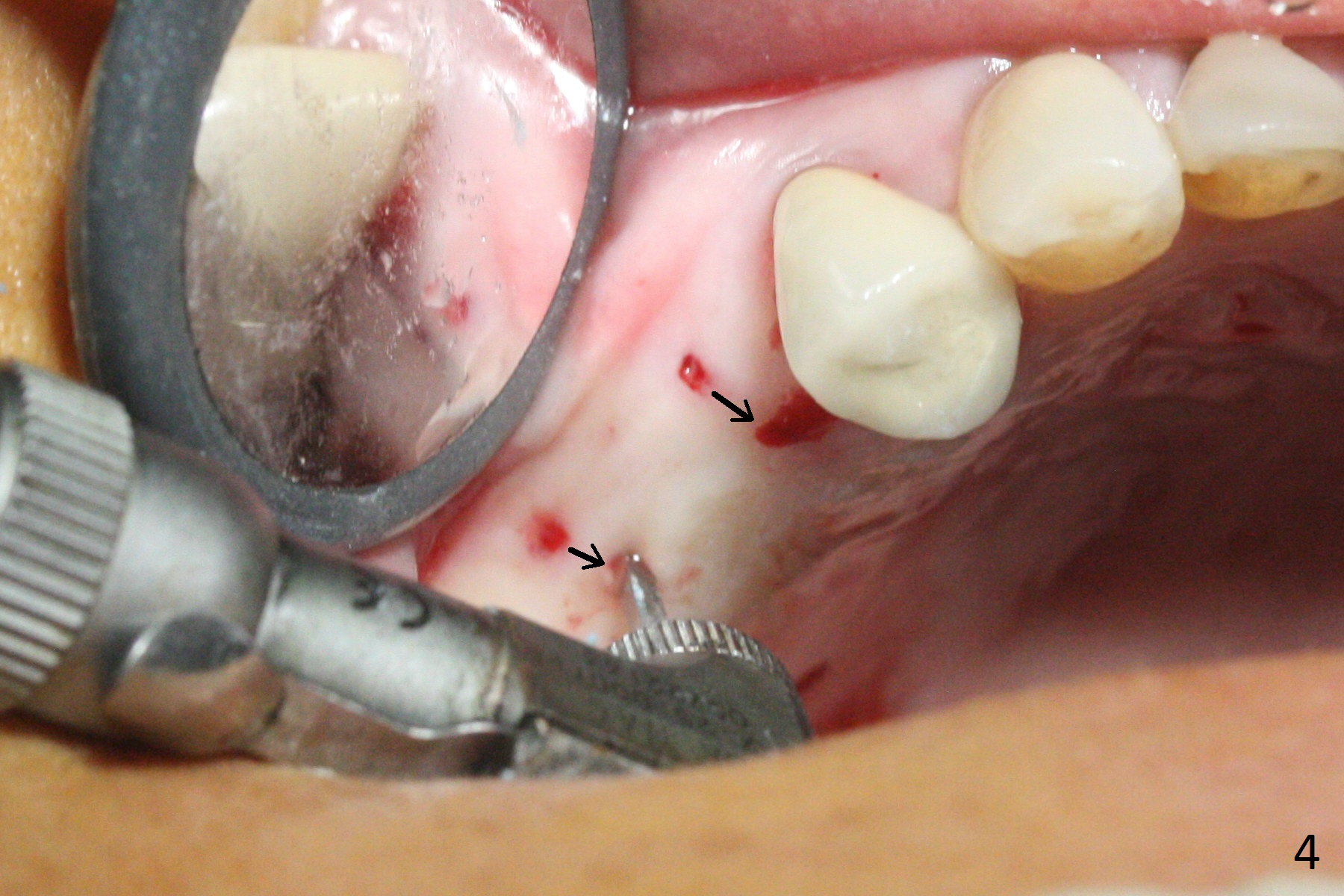
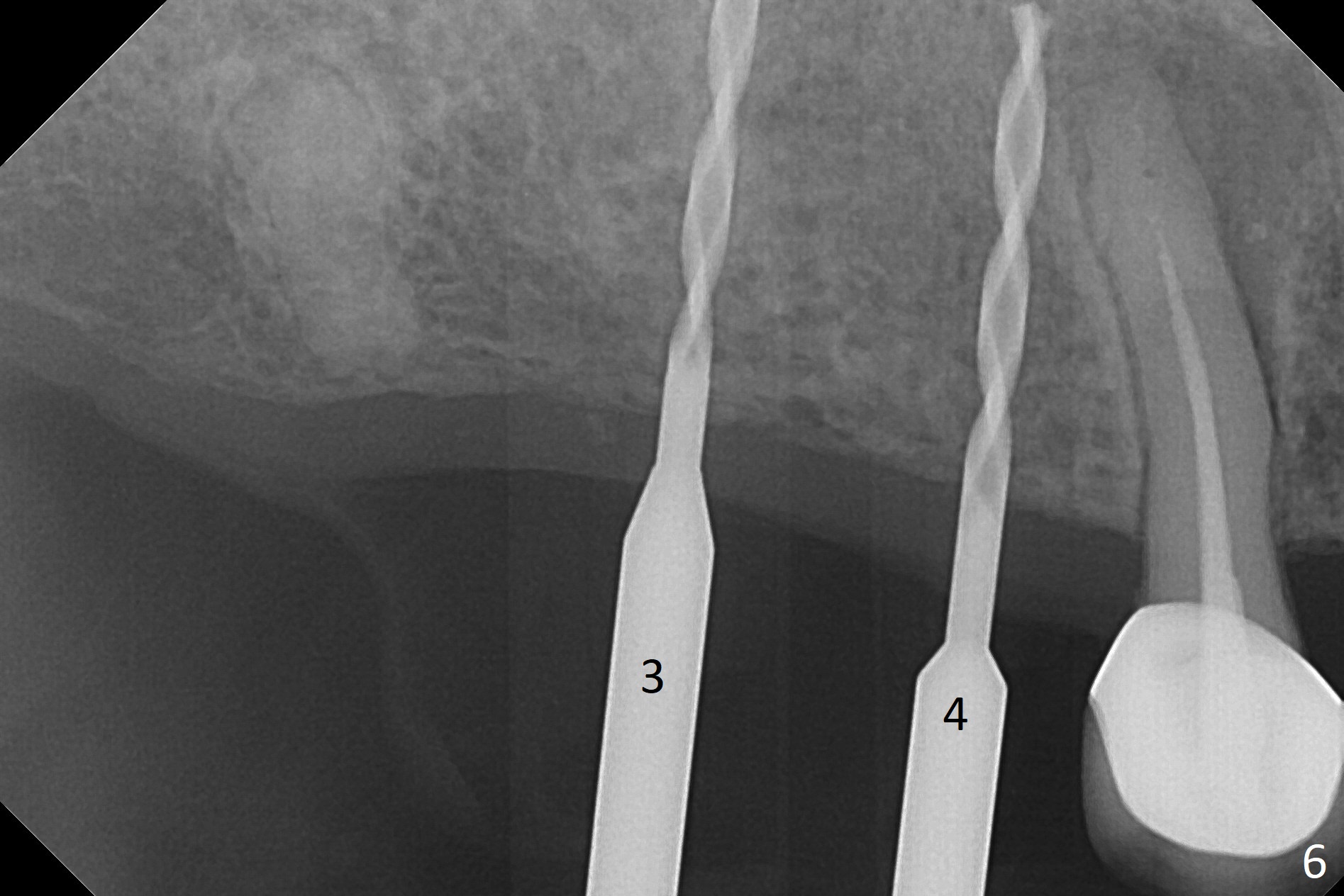
Time for Surgical Guide
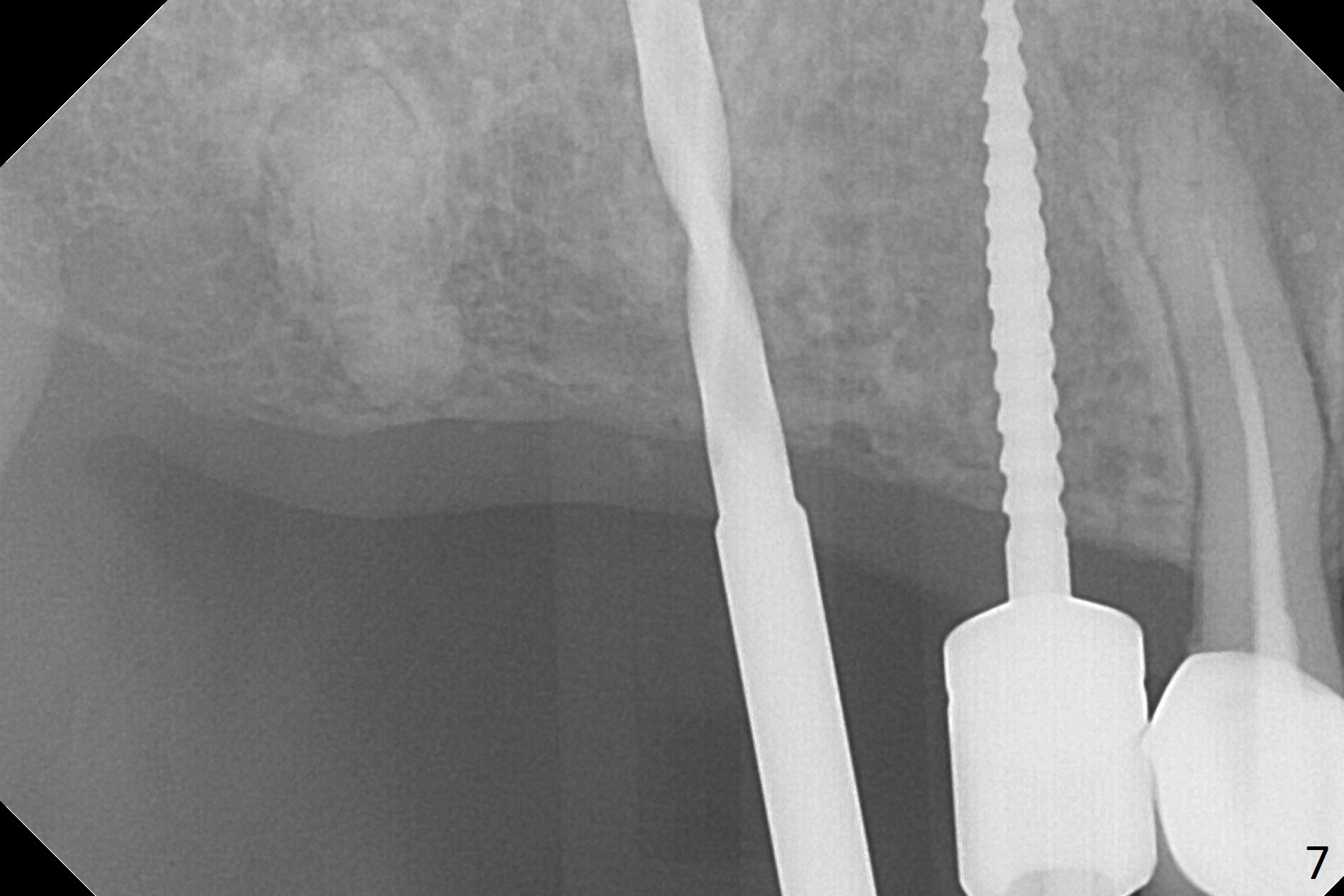
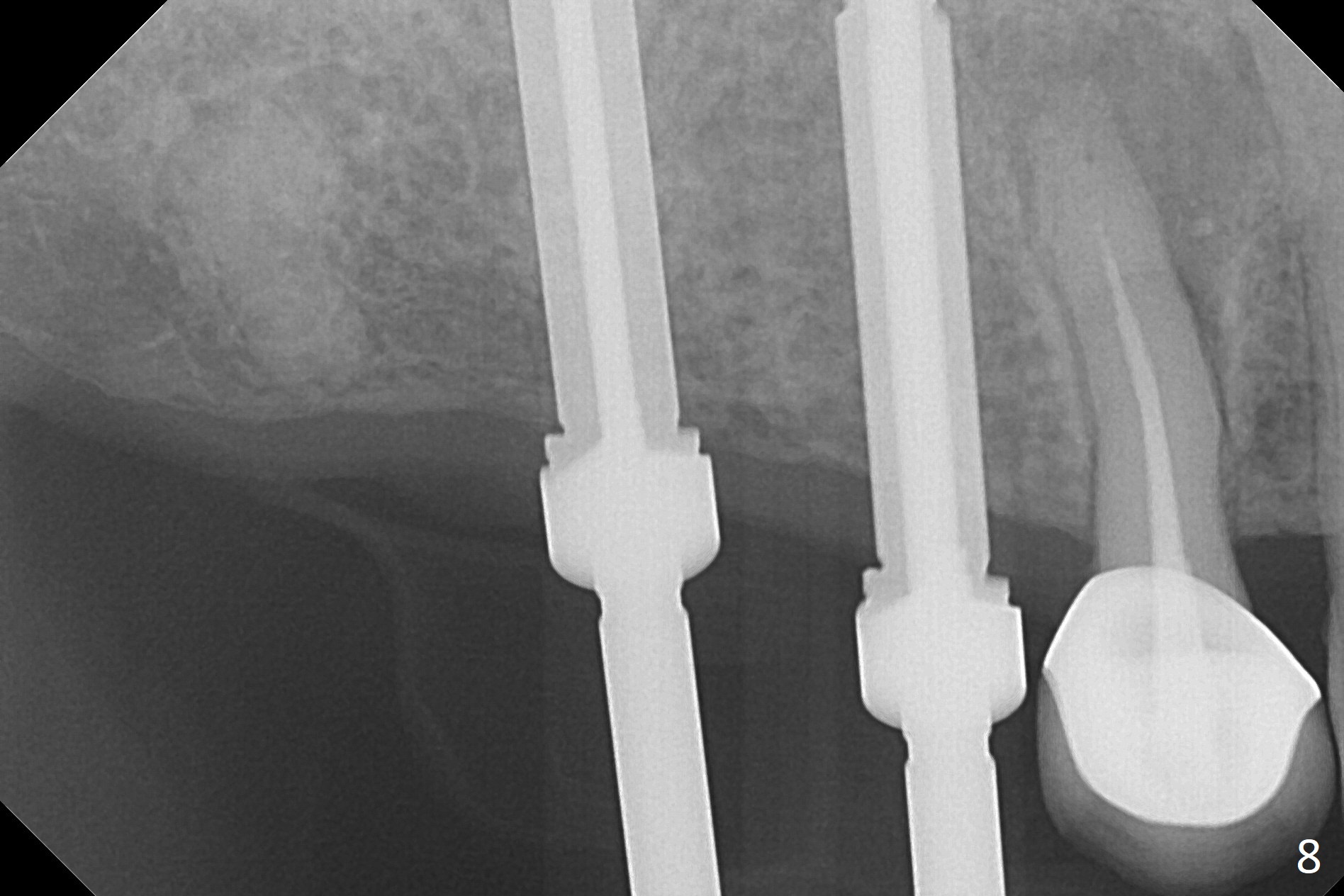
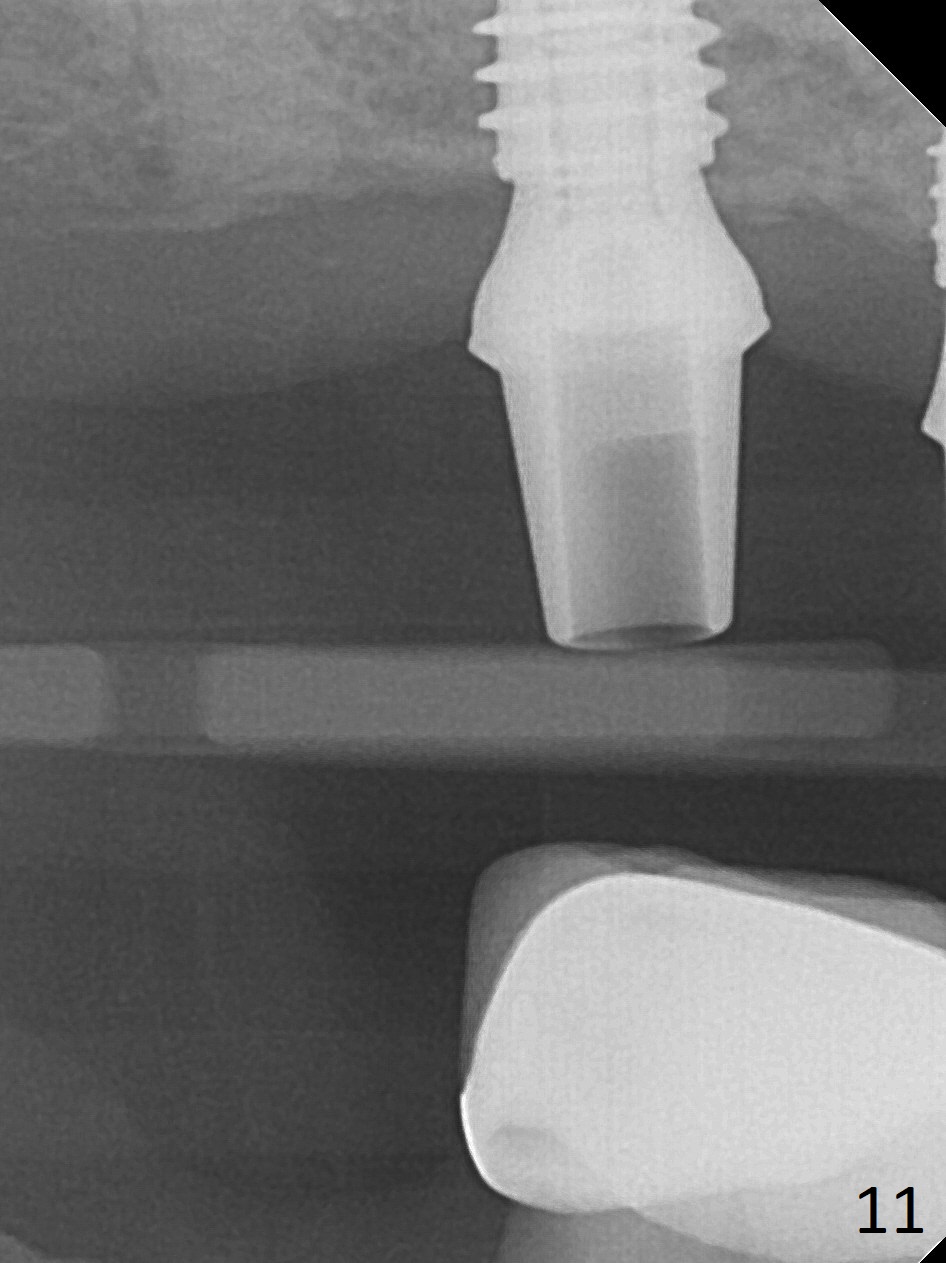
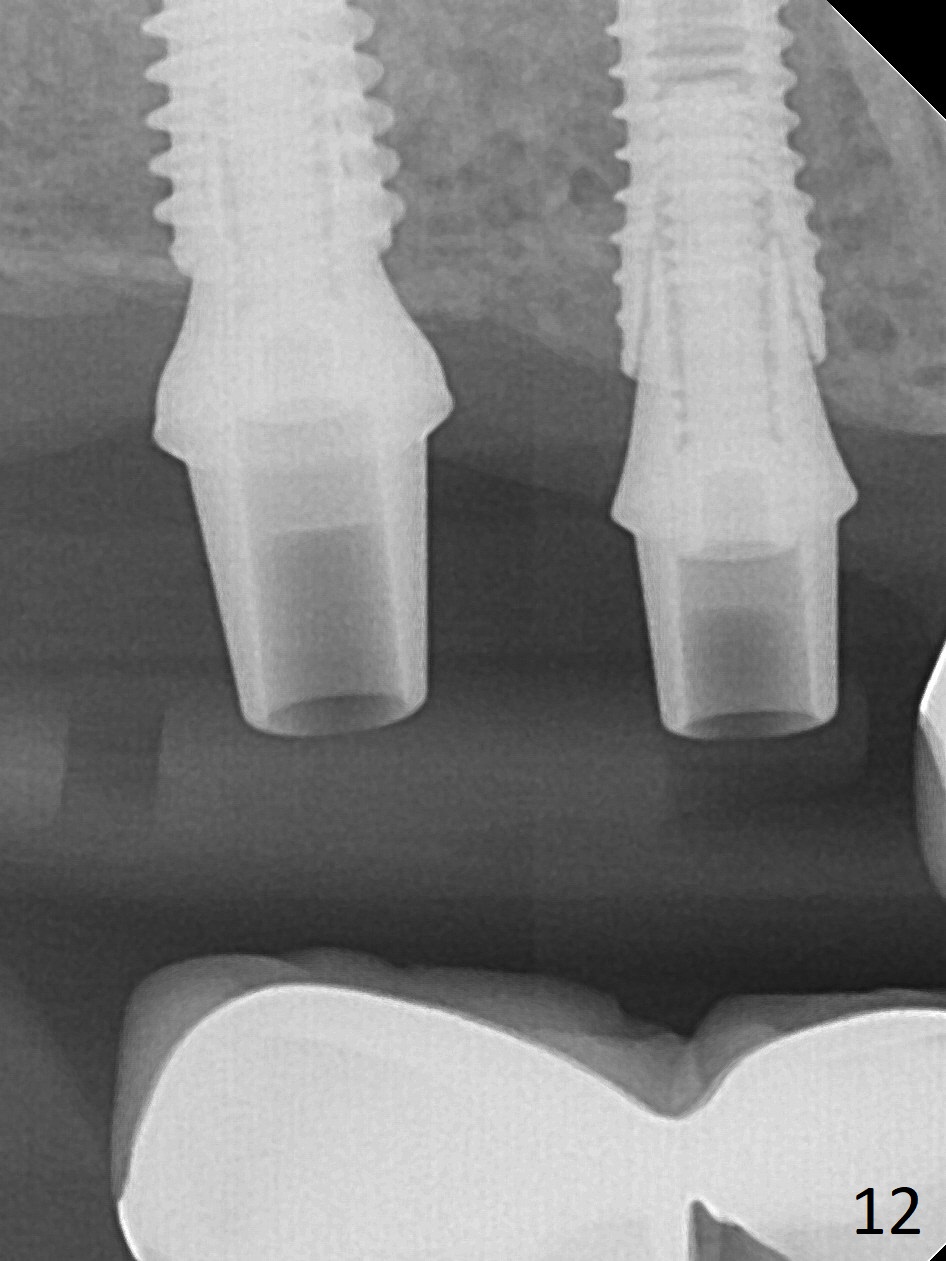
The ridge at #3,4 is wide (Fig.1). A surgical stent is placed (Fig.2) for initial osteotomy (Fig.3). When the stent is removed, the osteotomies need to move palatal (Fig.4 arrows). As two of 1.2 mm drills are in place (Fig.5), mesiodistal trajectories are found off (Fig.6). After the trajectories are corrected (Fig.7), the depth cannot be determined with PA (Fig.8, as compared to Pan (Fig.9)). Following 4.3 and 3.2 mm final drills at #3 and 4, 4.5x13 and 3.8x15 mm implants are placed with insertion torque of 35 and 50 Ncm, followed by 5.5x4(3) and 4.5x4(2) mm abutments (Fig.10). BWs show incomplete placement of the implant at #4 distal (Fig.11,12). Later the implant is placed ~ .5 mm deeper. Periodontal dressing is applied postop. CT-assisted surgical guide must be more efficient for this case with wide ridge. There is no bone loss around the implants 3 moths postop
(Fig.13).
Return to
Upper Molar,
Premolar Immediate Implant,
IBS
Xin Wei, DDS, PhD, MS 1st edition 06/22/2017, last revision 10/01/2017