

.jpg)
,%20more%20graft%20later.jpg)


|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
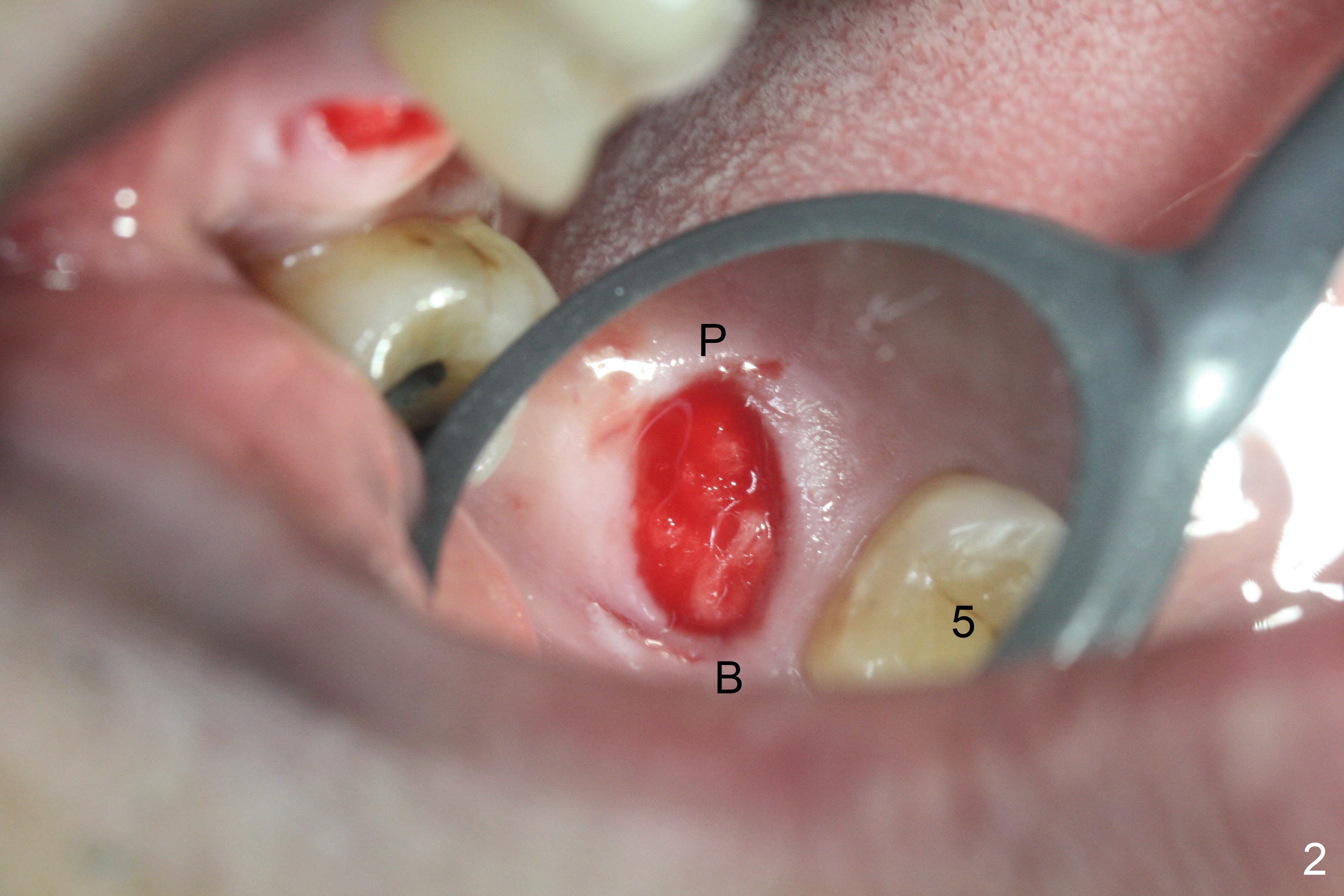
Shift Osteotomy Distal
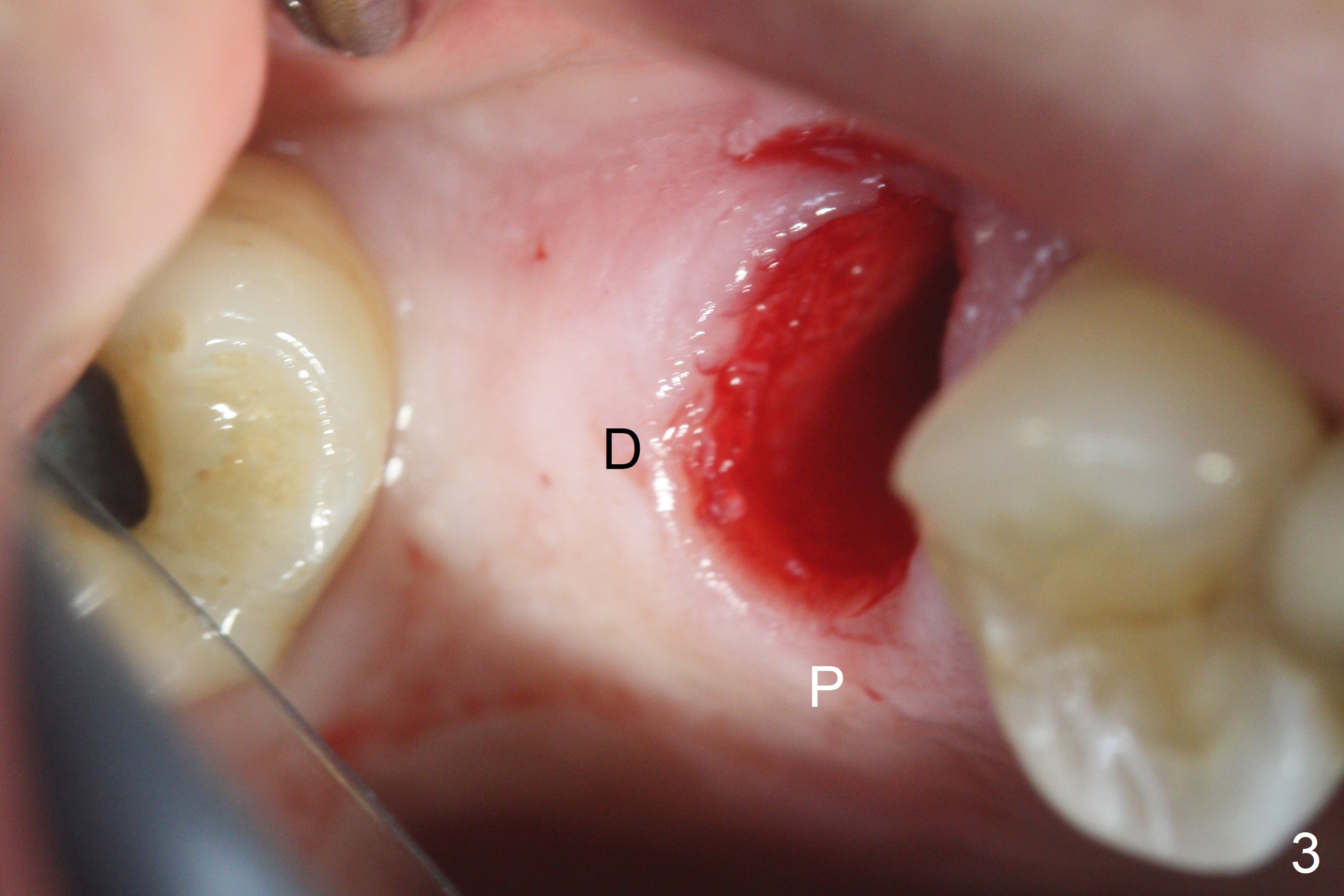
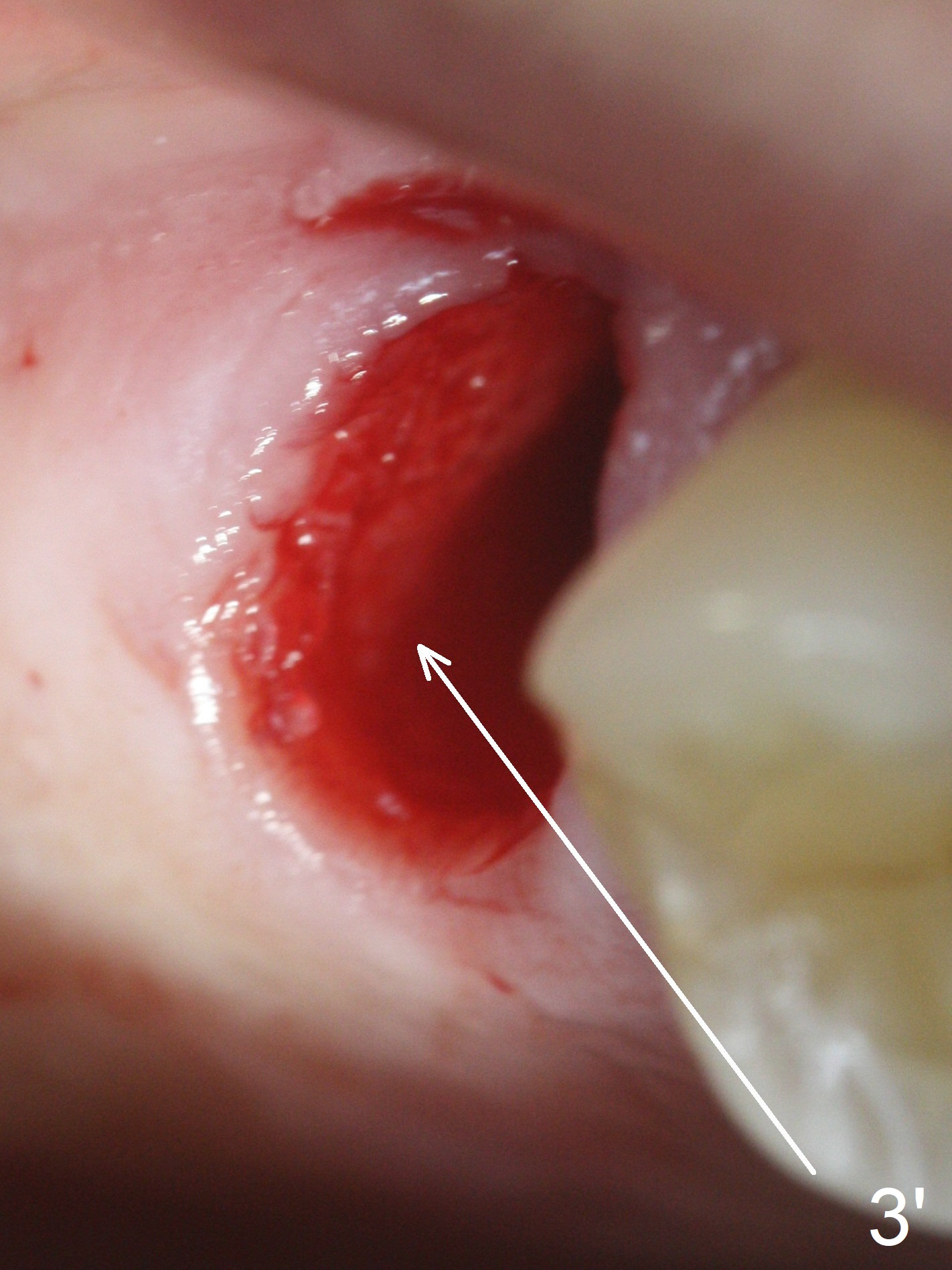
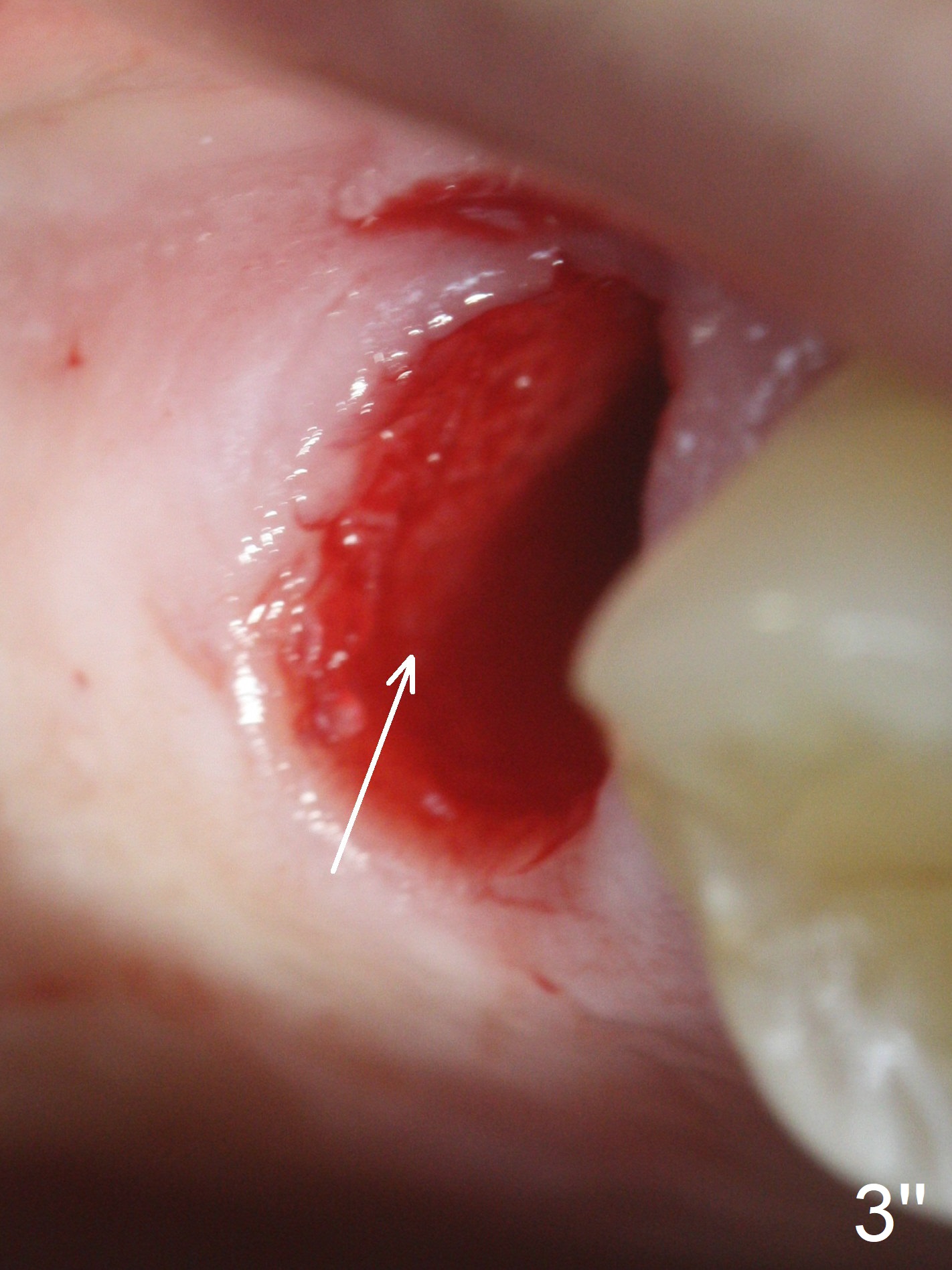
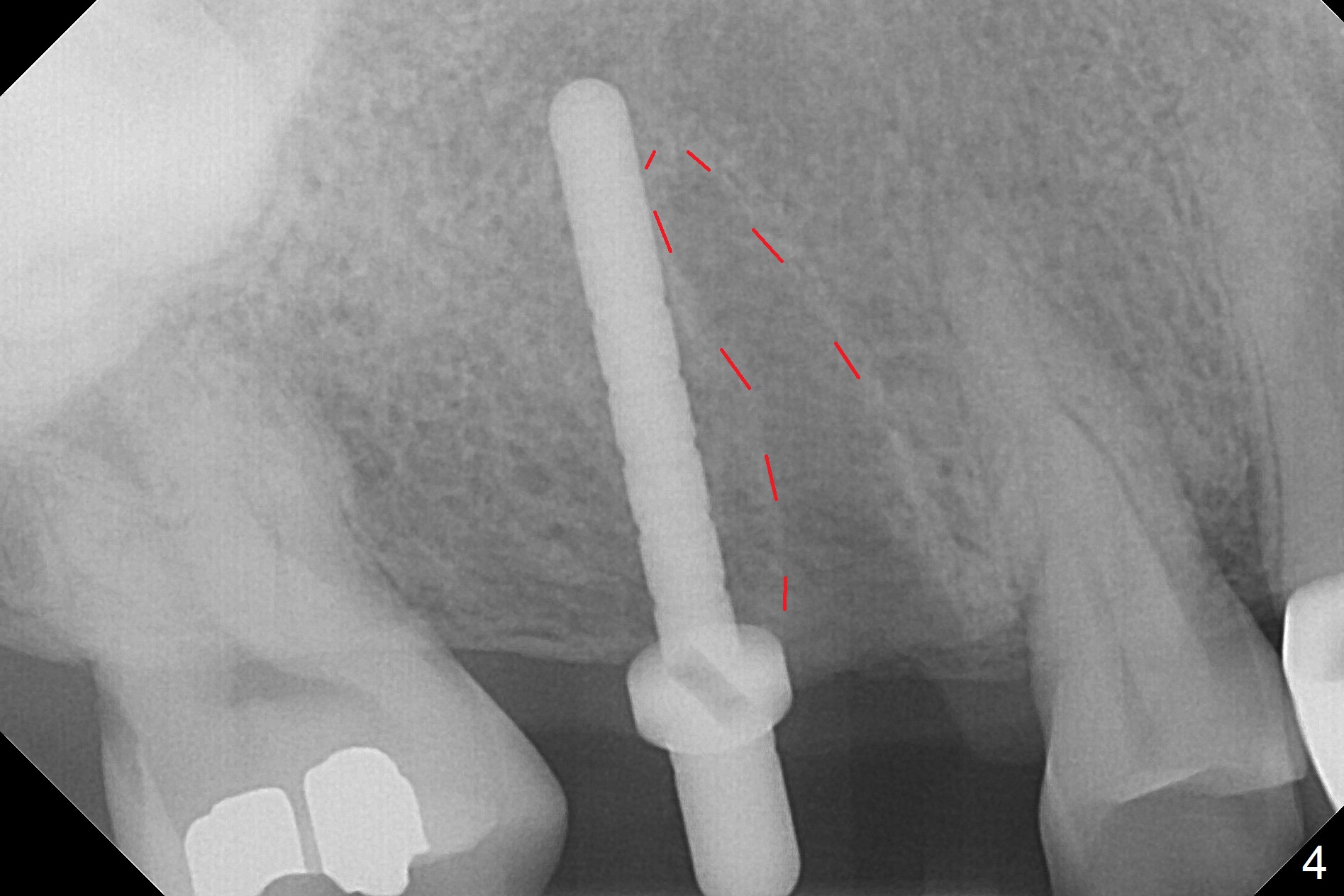
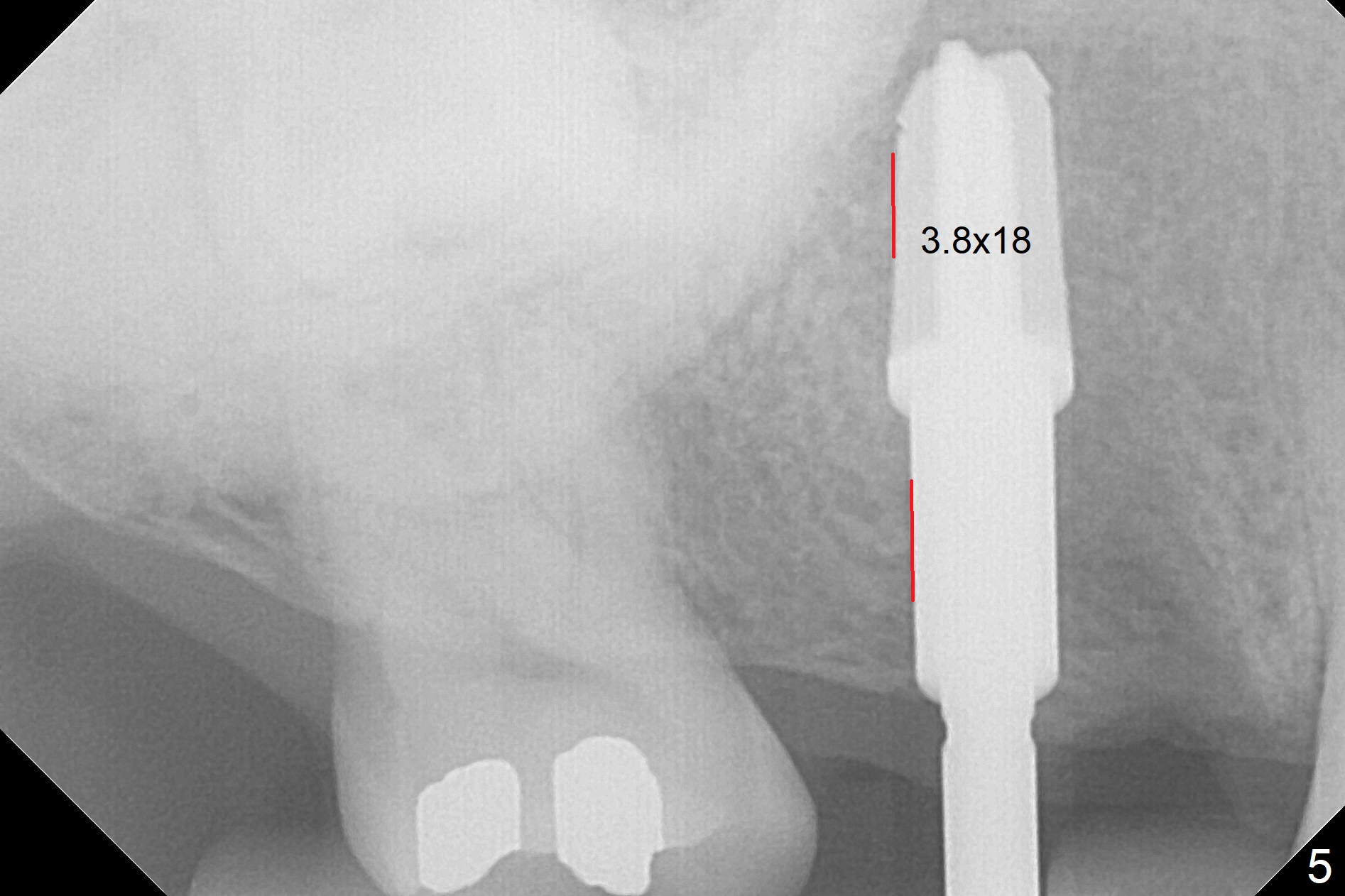
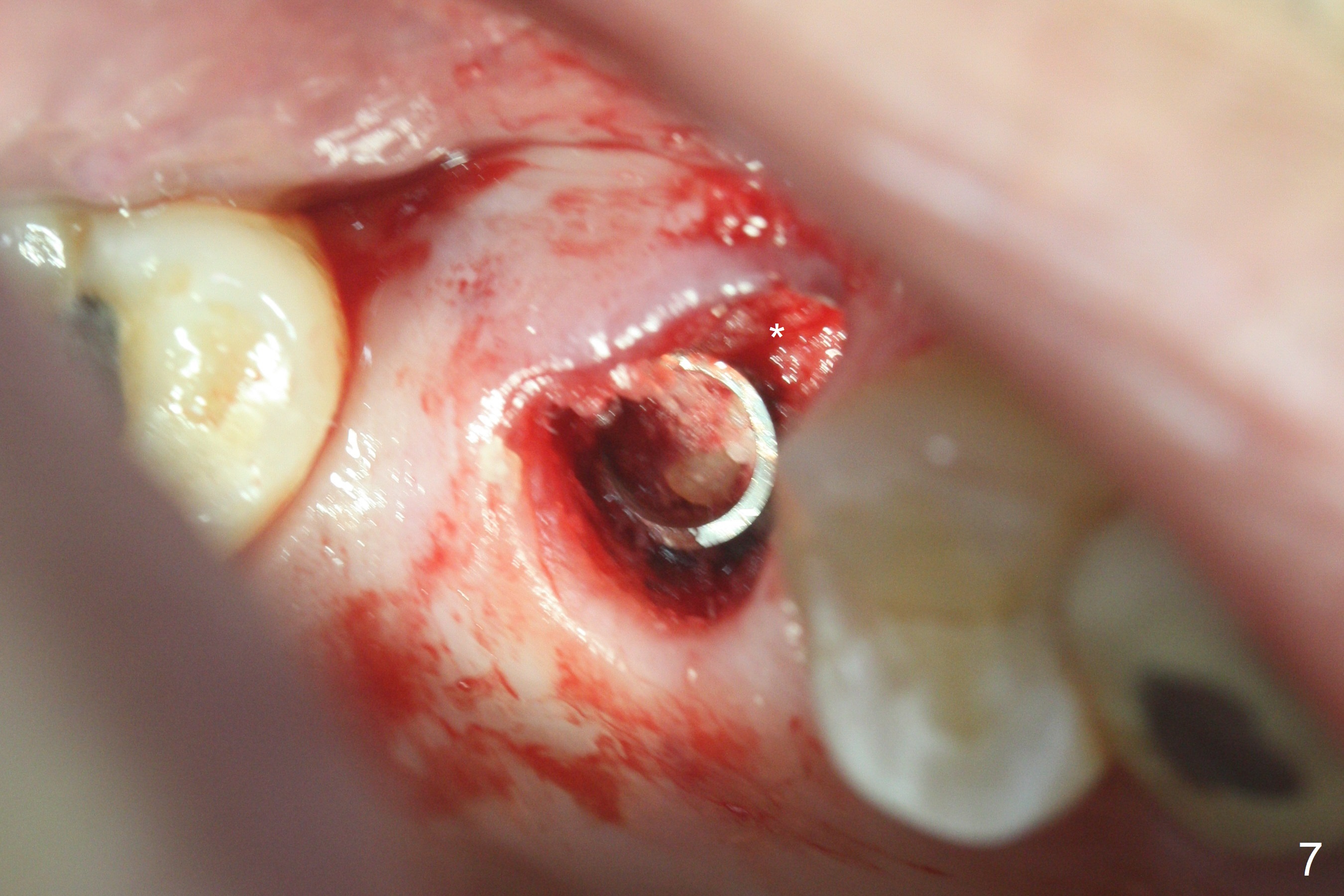
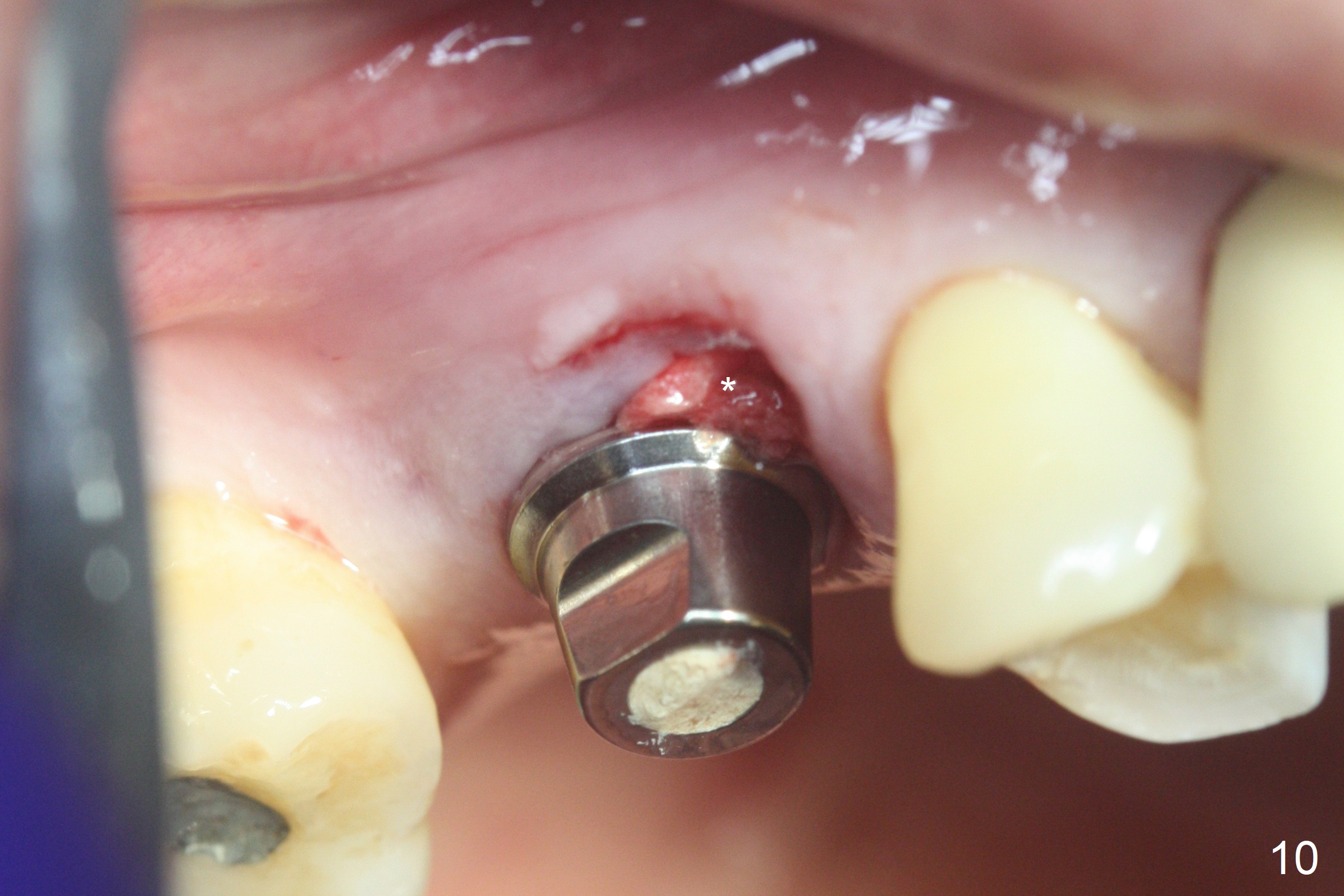
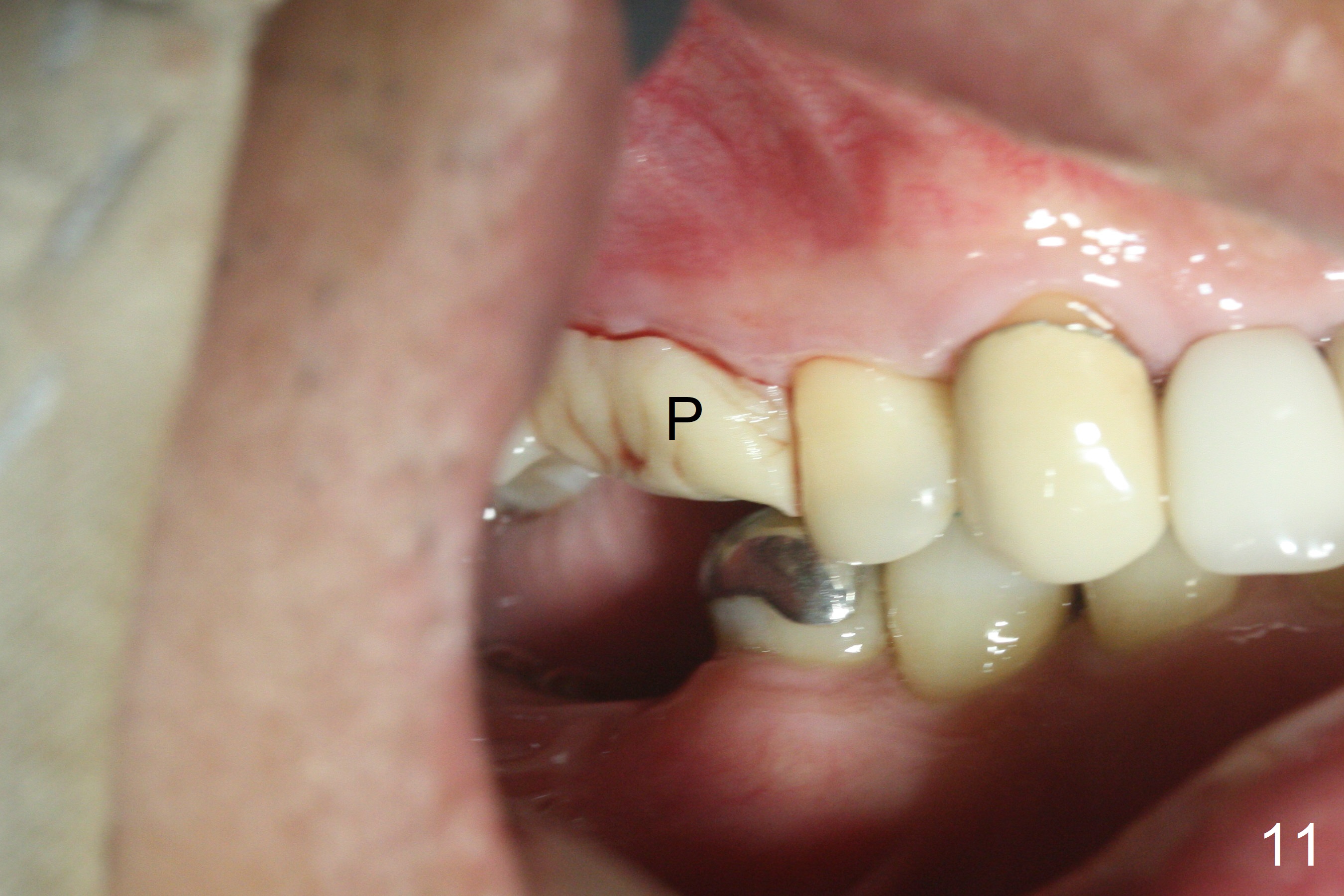
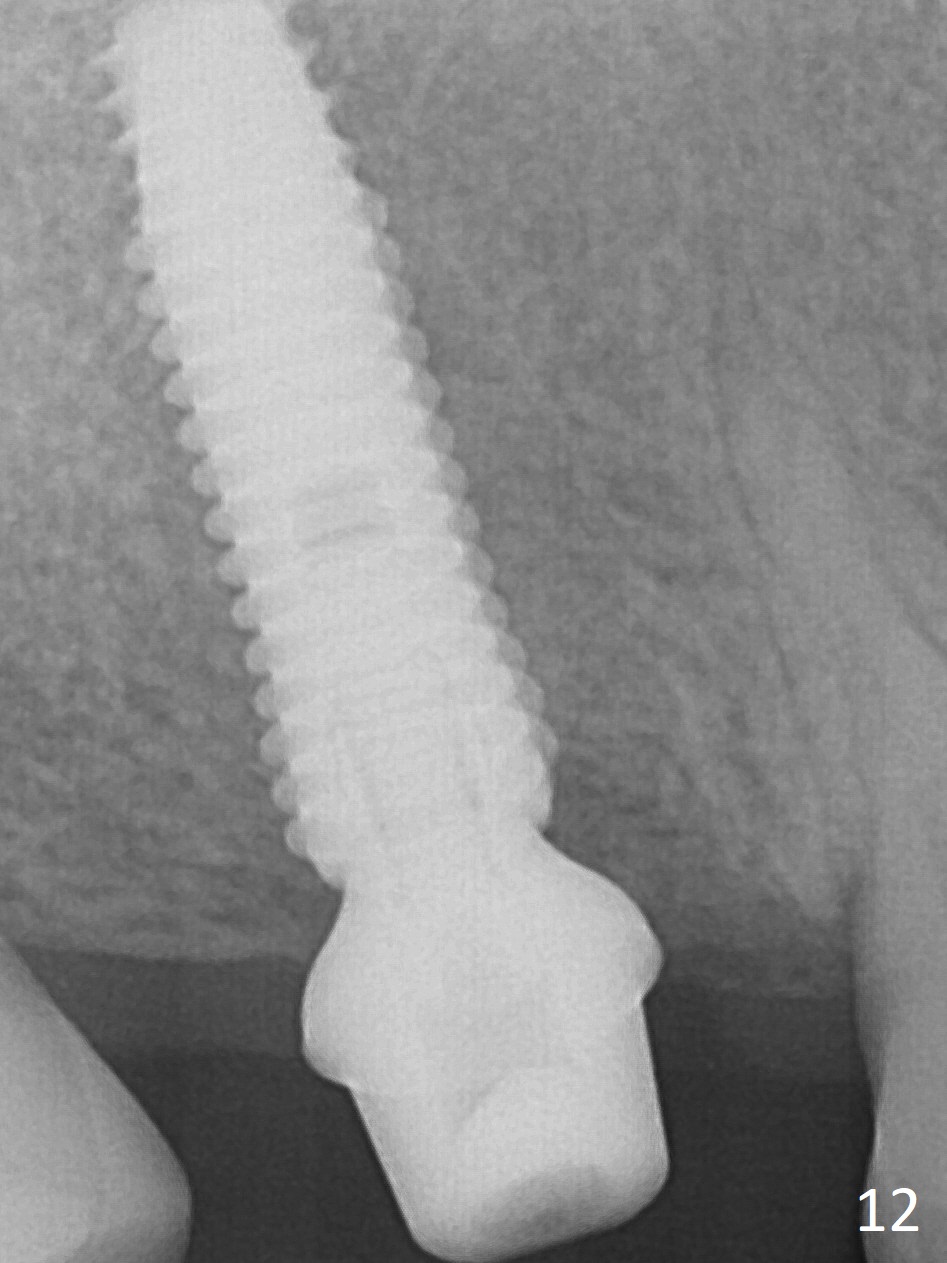
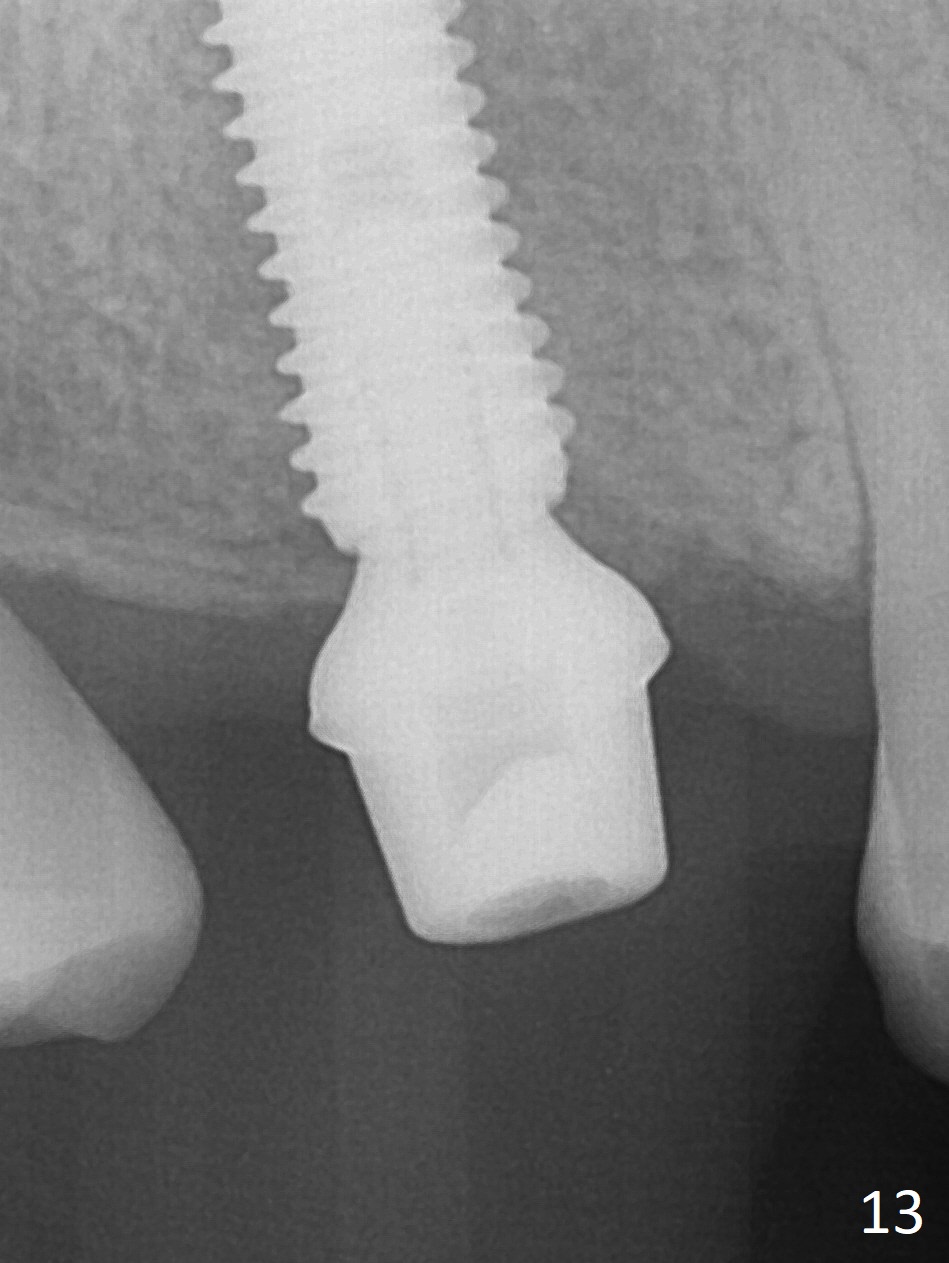
The palatal cusp of the affected 2nd premolar is apparently rotated distal (Fig.1). It is more obvious for the socket (Fig.2): the palatal (P) portion of the socket is more distal than the buccal (B) one. When the gauze is removed (Fig.3), Lindamann bur is used to remove the disto(D)palatal bone of the socket (data not shown), followed by starter drill in the DP wall obliquely (Fig.3'). Once the drill enters the bone for 1-2 mm, the bur is straightened and pushed slightly distal (Fig.3''). Fig.4 shows a parallel pin distal (overcorrect) to the original socket (Fig.4 red dashed line). Sequential osteotomy is conducted until 3.8x13 mm drill for 18 mm (Fig.5): note the 2 steps of the osteotomy (red lines). Since the apical portion of the osteotomy is larger than the drill, a larger implant than expected (5x16 mm) is placed. The implant ends up in the middle of the edentulous area (due to the stepped osteotomy; Fig.6-9; >60 Ncm). Vera allograft is placed (Fig.7-9 *) prior to and after placement of a 6.5x4(3) mm abutment (Fig.8-10). The remaining socket opening is sealed with a piece of Collagen plug (Fig.10 *). The socket is then closed by an immediate provisional (Fig.11 P). The abutment is retightened 2 months postop (Fig.12,13). The crown is cemented 4.5 months postop. Panoramic X-ray and CT are taken nearly 7 months post cementation (Fig.14,15) when the patient is ready for #30 implant guide preparation.
Return to
Upper Premolar
Molar Immediate Implant,
IBS, #7-10
Chinese
Xin Wei, DDS, PhD, MS 1st edition 09/05/2017, last revision 08/09/2018