











|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Increase Vertical Height with Tooth and Implant Provisional
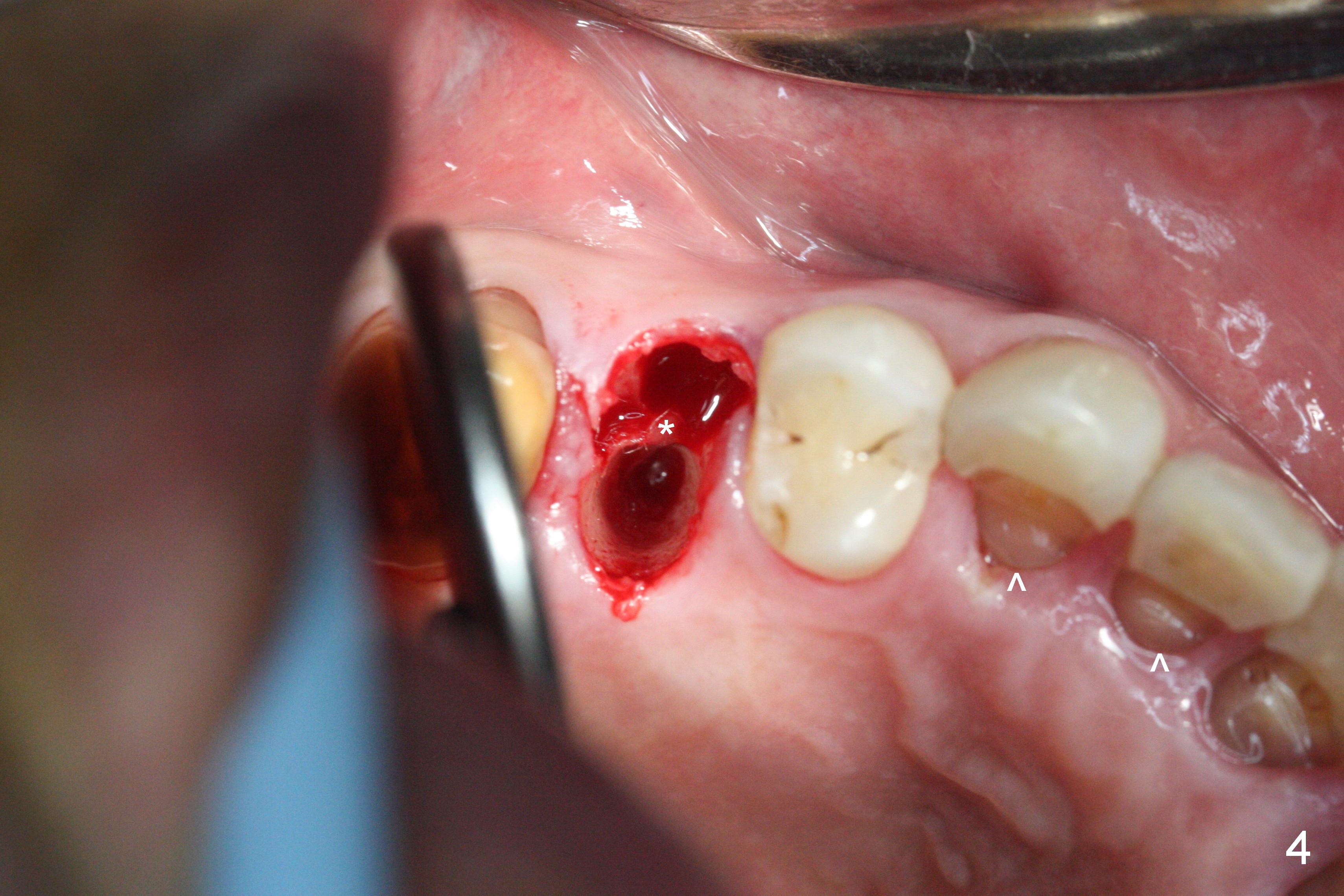
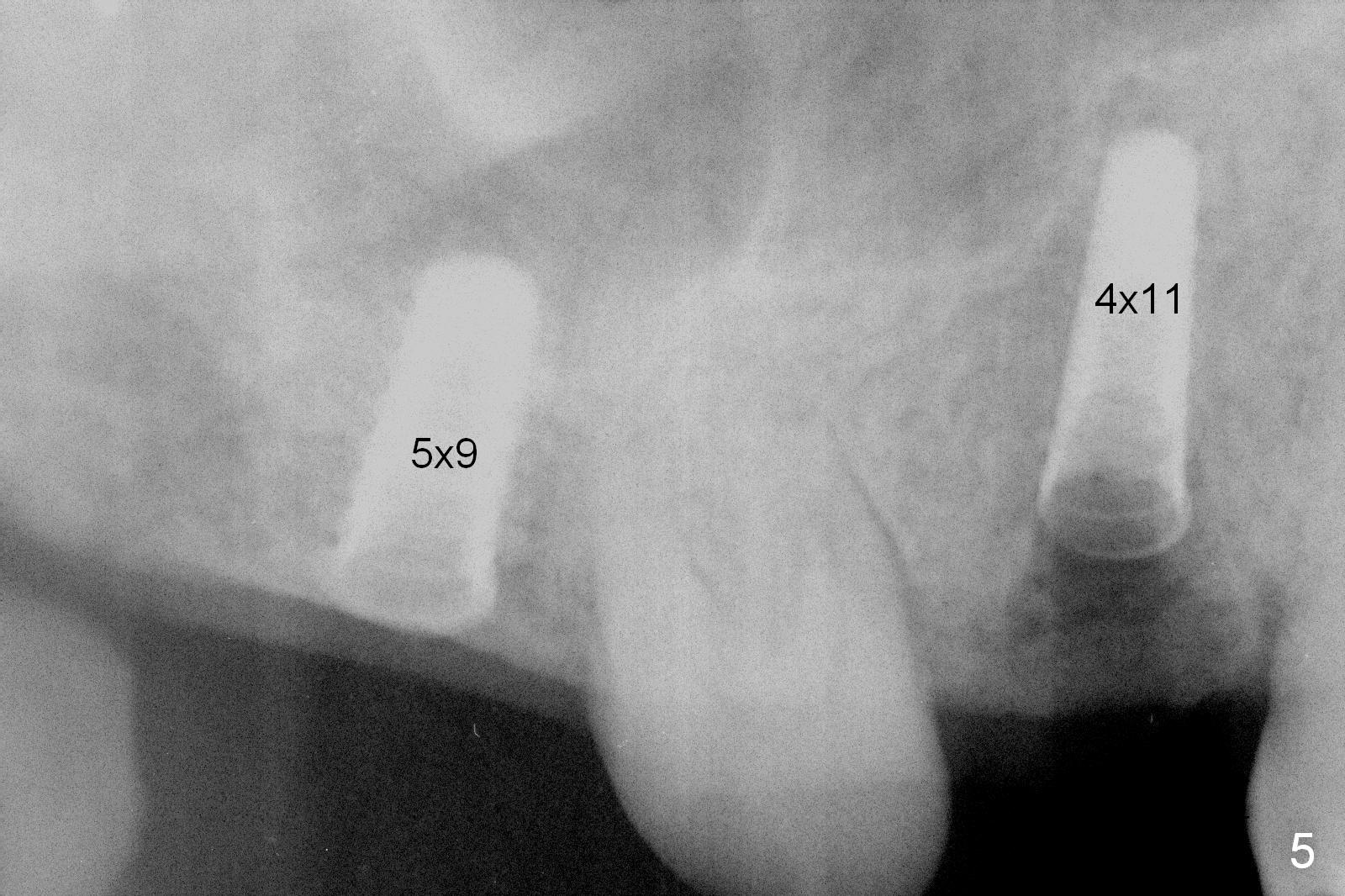
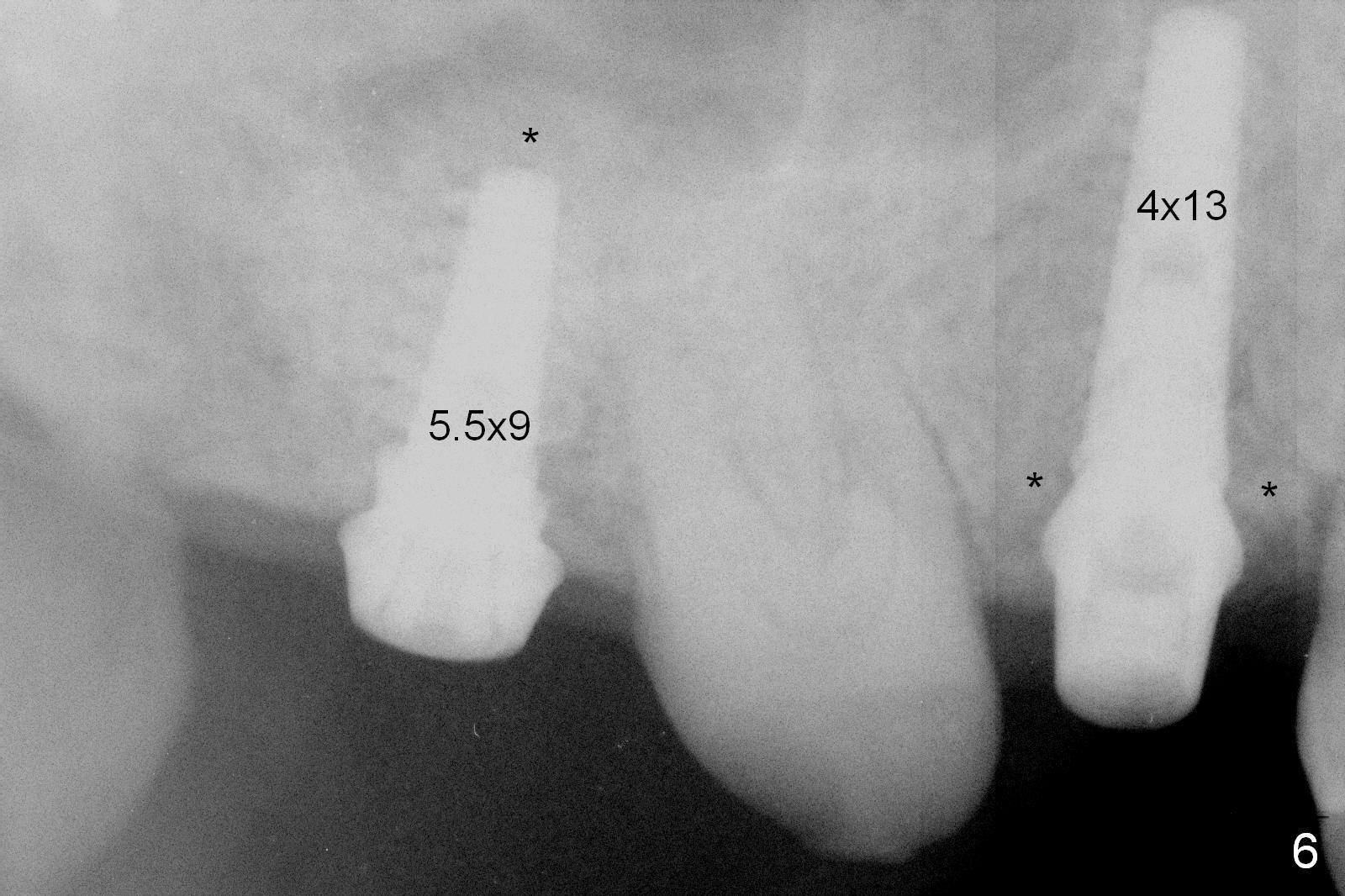
Preop exam shows posterior occlusal collapse (Fig.1) with #3 lost crown and #4 residual root. There is no ridge atrophy at #2 buccopalatally (Fig.2). The root stump of the tooth #4 is oblong, apparently consisting of 2 roots (Fig.3). There is a pointed septum at #4 socket (Fig.4, severe palatal wear of the anterior teeth (^)). After the septum is flattened with surgical handpiece and #8 round bur, 1.6 mm drill is used to start osteotomy in the septum, followed by Magic Drills (MD) and Magic Expanders (ME) alternatively. Osteotomy at #2 is initiated with Magic split, followed by MD and ME in the same manner. Dummy implants are tried in (Fig.5). Because of limited vertical height, Magicore (5.5x9(1) mm) is placed at #2, while a 4x13 mm FC implant 1-2 mm deeper than usual at #4 (Fig.6, ~ 55 Ncm). When a 5x4(2) mm pair abutment is placed at #4, there is no clearance between the Magicore at #2 and the abutment and the opposing dentition. A splinted provisional is fabricated at #3 and 4 to increase the posterior vertical height (Fig.7 P,8). In fact the occlusal contact is confined to the portion of the provisional at #3. The provisional has to extend to #4 to keep bone graft (Fig.6 *) and collagen plug in place. Liquid food is recommended at least 2-3 weeks, since there is no functional occlusal contact on the left. When the wound heals at #4 approximately 2-3 weeks, the splinted provisional can be sectioned with removal the portion at #4 to reduce micro-movement. By the evening the patient is doing well without nasal hemorrhage (sinus lift at #2 (Fig.6 *) or TMJ disturbance (due to increased vertical height).
When the patient returns 2 months postop, place a 5.5 mm healing cuff for Magicore at #2. At 4 months postop, place a 5.5x2 mm solid abutment for restoration (driver unavailable). Reduce the opposing supraerupted tooth (#31) if needed.
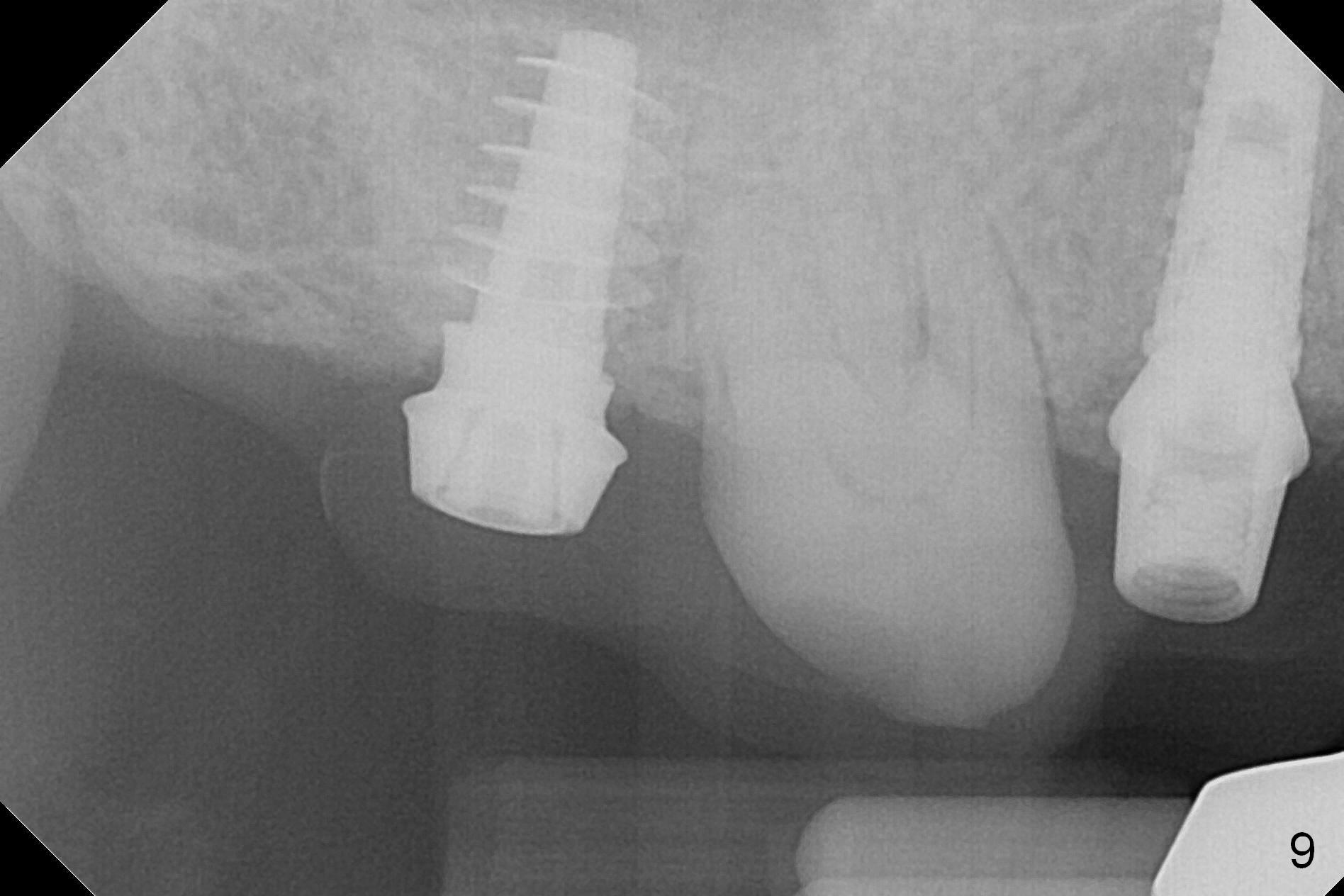
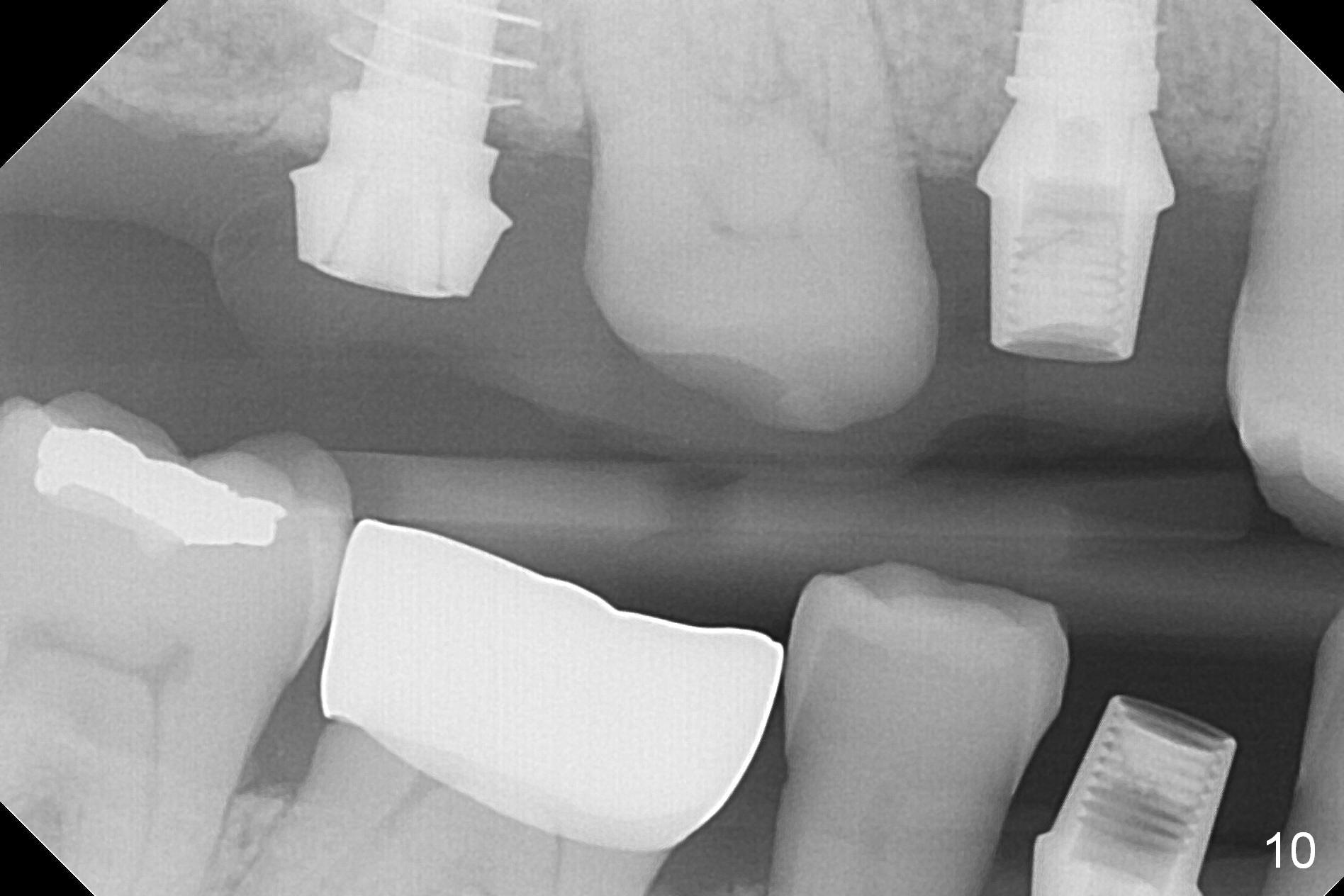
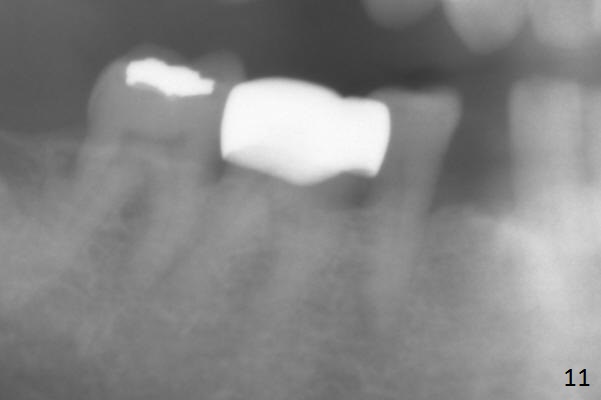
In fact the upper provisional has been extended to cover #2-4 three months postop. When the patient returns again, it is approximately 4 months postop for #2 and 4 (Fig.9,10) and 3 months for #28. Reline or make the provisional so that the teeth #5 and 29 will be intruded (Fig.11 preop pan for comparision). The tooth #30 appears to have been intruded for the past 4 months. The provisional at #3 is short so that the tooth #30 may be able to erupt (Fig.12).
Six months postop, the upper right splinted provisional between #2 and 4 is sectioned so that the tooth #3 is also free to erupt naturally (Fig.13). The patient tolerates occlusal increase well.
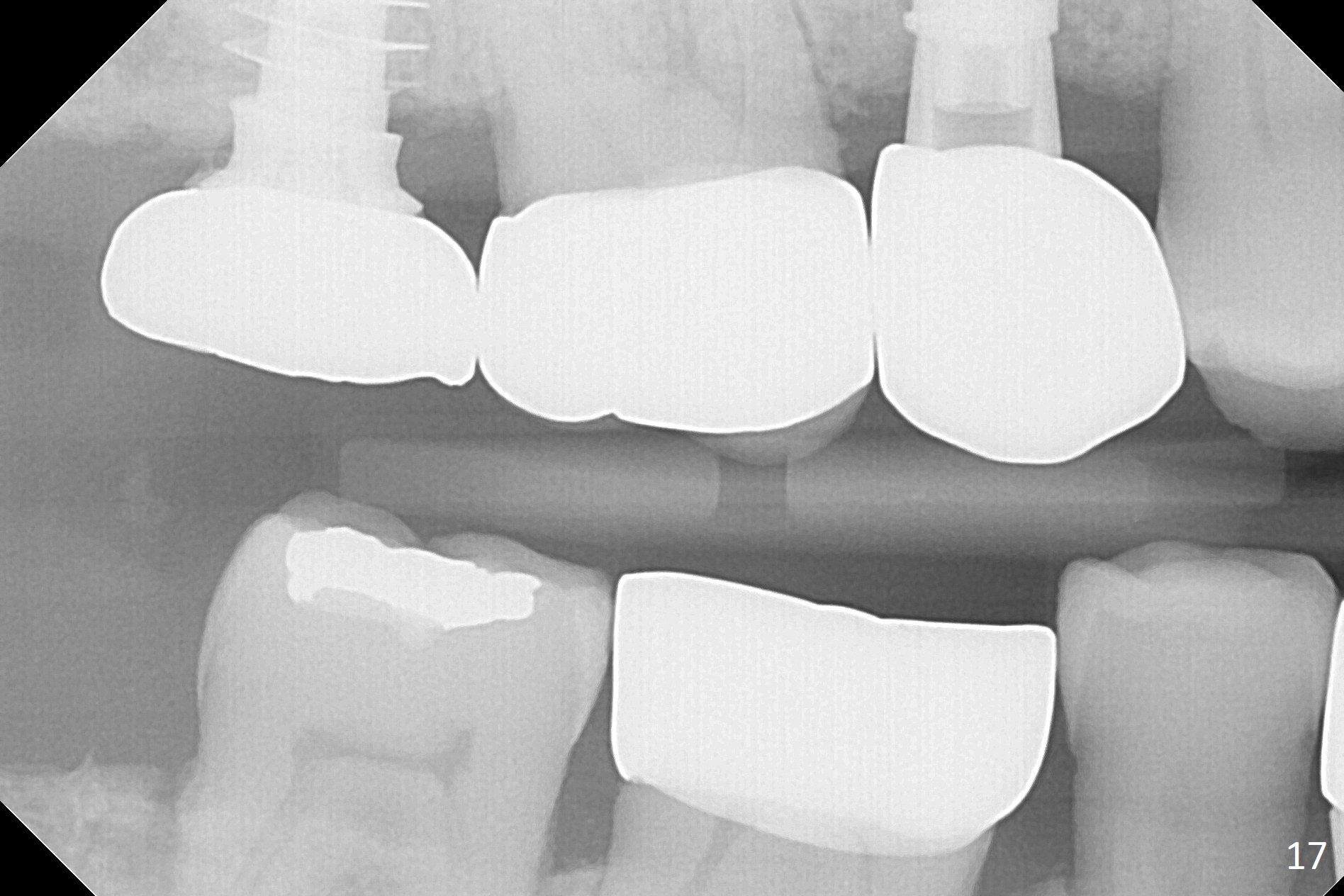
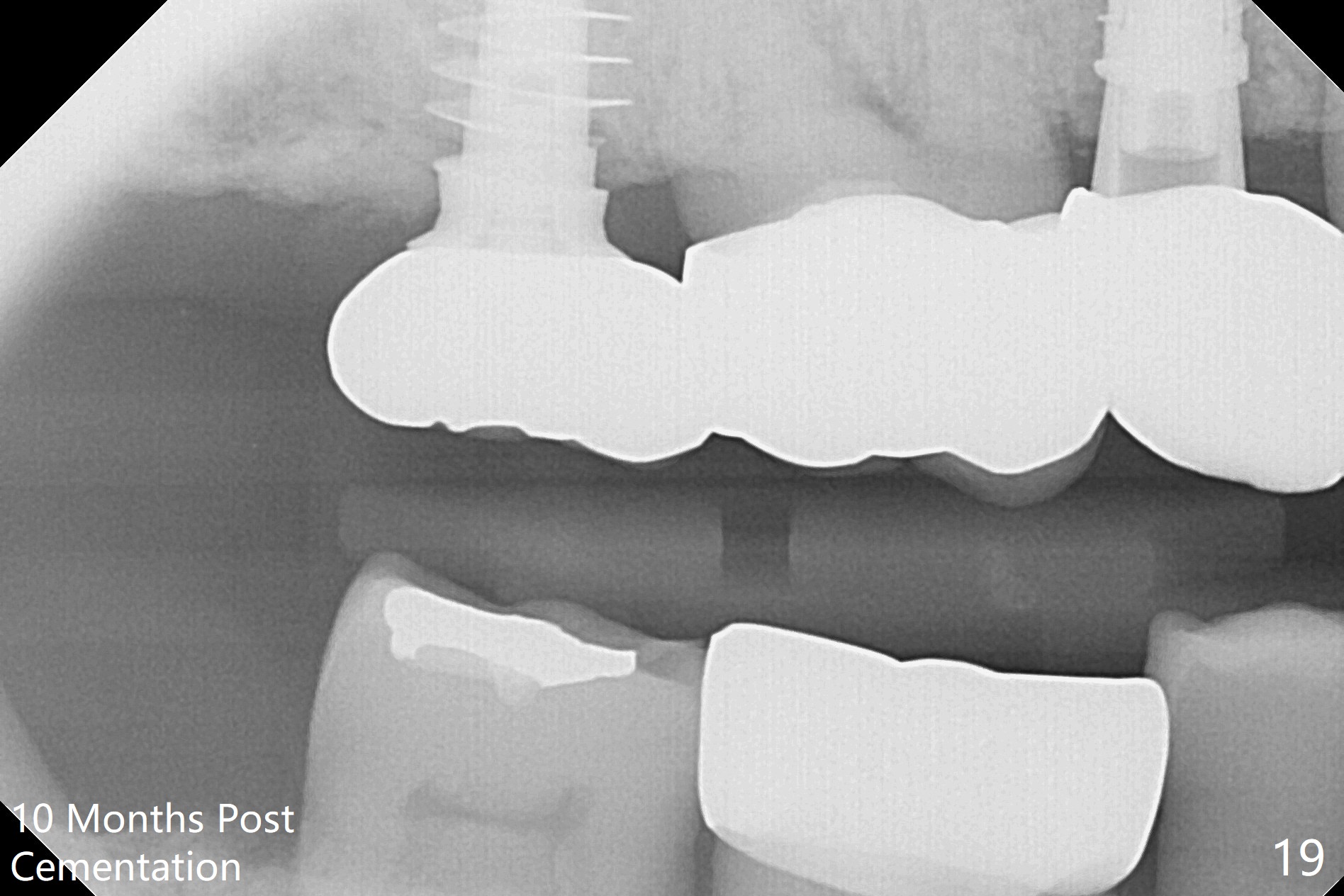
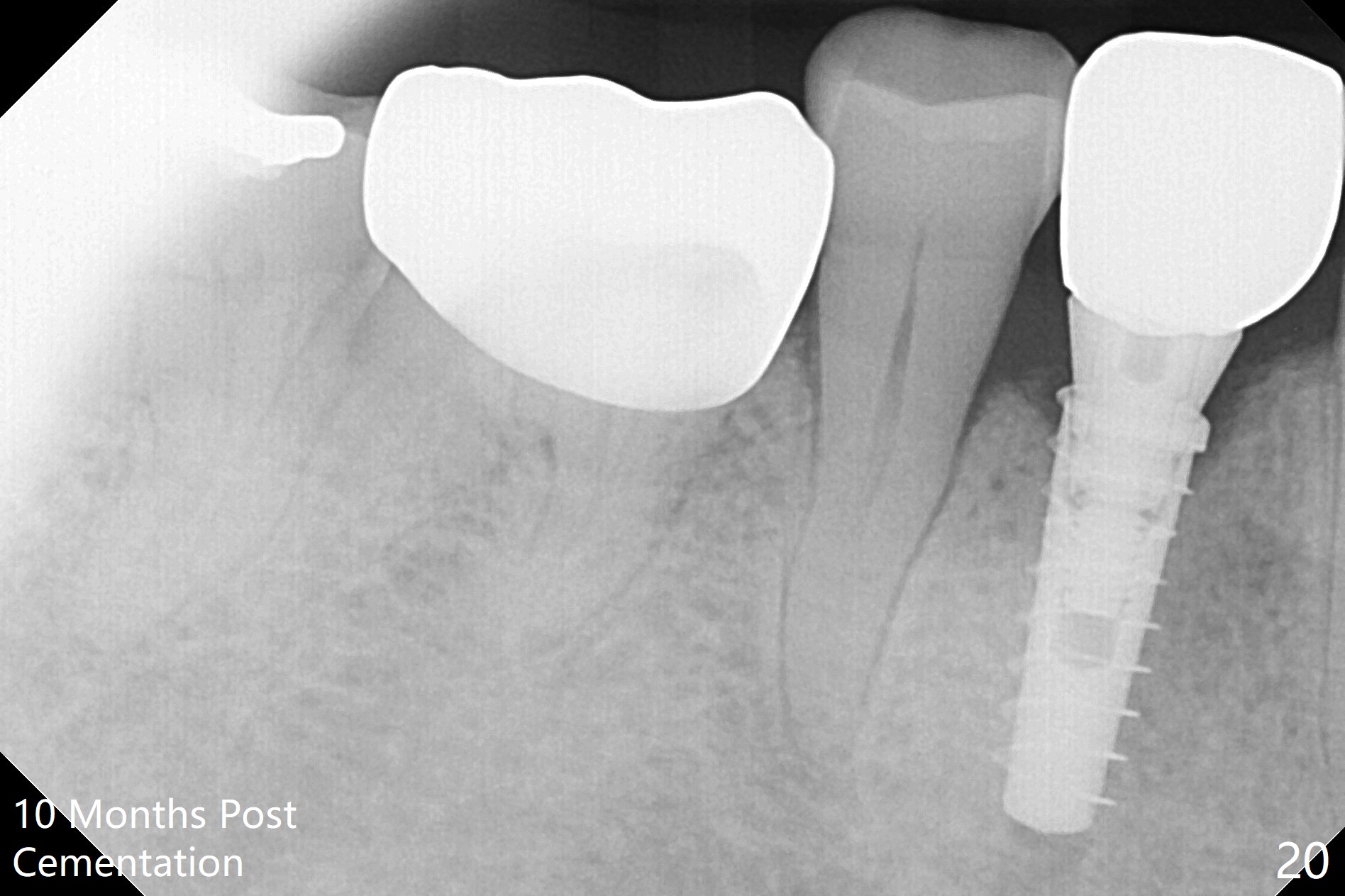
The right posterior final restorations (Fig.14) are fabricated as planned: increase in vertical height (Fig.15). The increase is minimal (Fig.14, 17(#2 limited crown height), 16 (#2 crown being thin *)). Fig.17,18 are taken immediately post cementation. There is no bone loss 10 months post cementation (Fig.19,20). The gingiva is healthy around the implant crowns (#2, 4 and 28) 1 year 4 months post cementation (Fig.21,22).
Return to Upper Molar, Premolar Immediate Implant, IBS, #28, 13-15 Design, 13-15 Placement, Implant & Ortho 2 1st Year, Magicore Cases
Xin Wei, DDS, PhD, MS 1st edition 11/14/2016, last revision 10/15/2018