








|
|
|
|
|
||
|
|
|
|
|
|
|
Trajectory Change Needs Critical Thinking
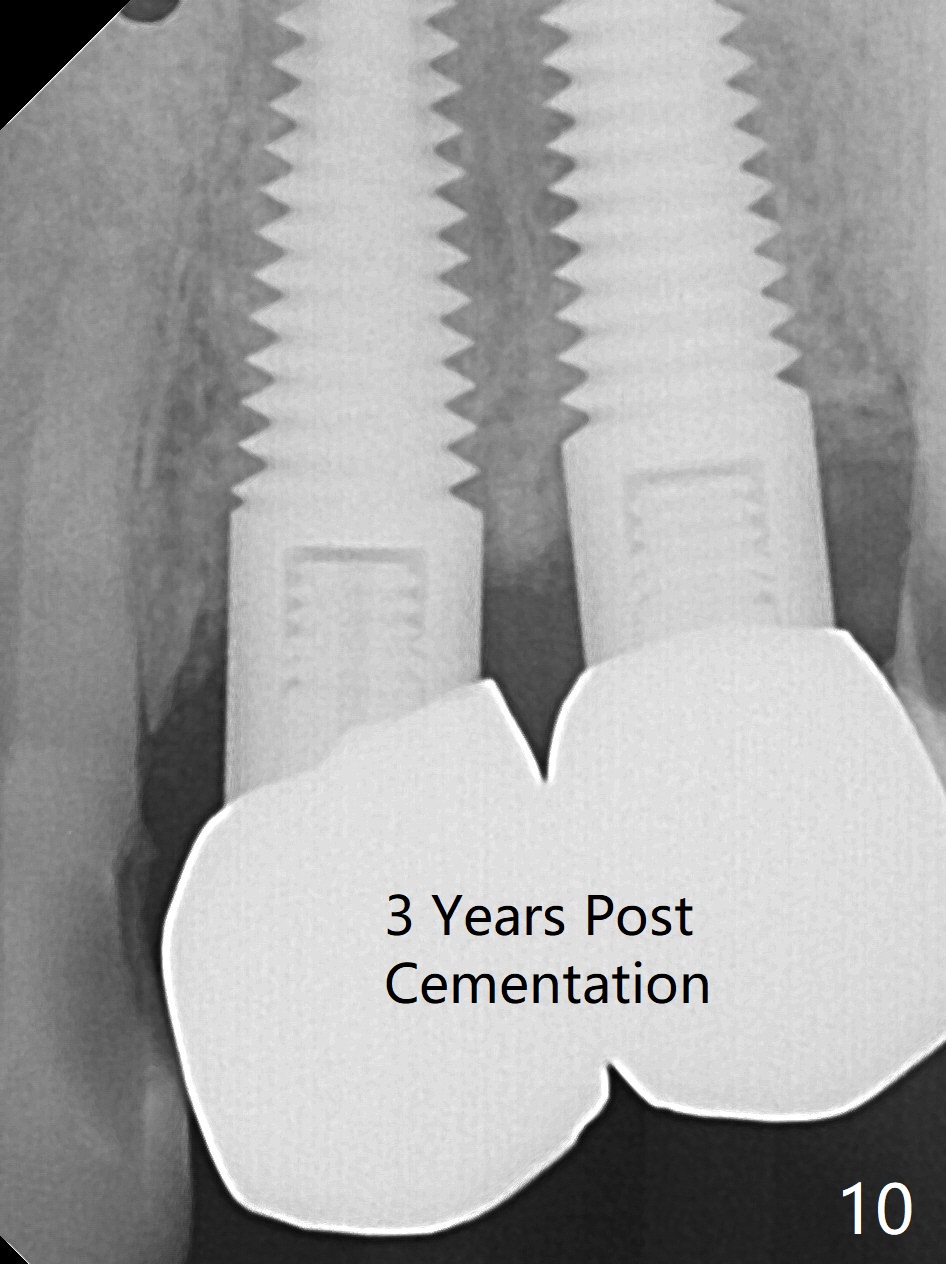
The socket at #12 is concave 2.5 months post socket preservation and #13 implant placement (Fig.1,2). The gingiva looks immature in the socket. As planned, osteotomy is created in the distal slope of the socket with a 1.5 mm drill (Fig.3). When the osteotomy increases with a 2 mm osteotome (Fig.4), it is close to the curved root of the canine (blue line). As a 3 mm osteotome is tapped in, the coronal end is positioned as close to the crown of the canine (Fig.5 red line), but there is excess of bone mesial to the osteotome (green). The excess of bone is removed before inserting a 4.5 mm tap (Fig.6); the coronal end of the tap is close to the neighboring tooth (arrows). When the implant at the site of #12 is partially placed, the separation from the neighboring root seems to be sufficient (Fig.7); the implant driver and the neighboring crown overlap (red dot). The separation remains the same as the implant is completely seated (Fig.8). Primary stability is satisfactory. An abutment is placed with fabrication of splinted provisional with #13. The patient returns for final restoration 2.5 months postop for #12 implant (Fig.9). The bone density around the coronal implant increases nearly 3 years post cementation (Fig.10).
Return to Upper Premolar Immediate Implant, Posterior Immediate Provisional 前磨牙即种 现在 Xin Wei, DDS, PhD, MS 1st edition 11/02/2015, last revision 05/02/2021