


|
|
|
|
|
|
|
|
|
|
|
Execution As Planned
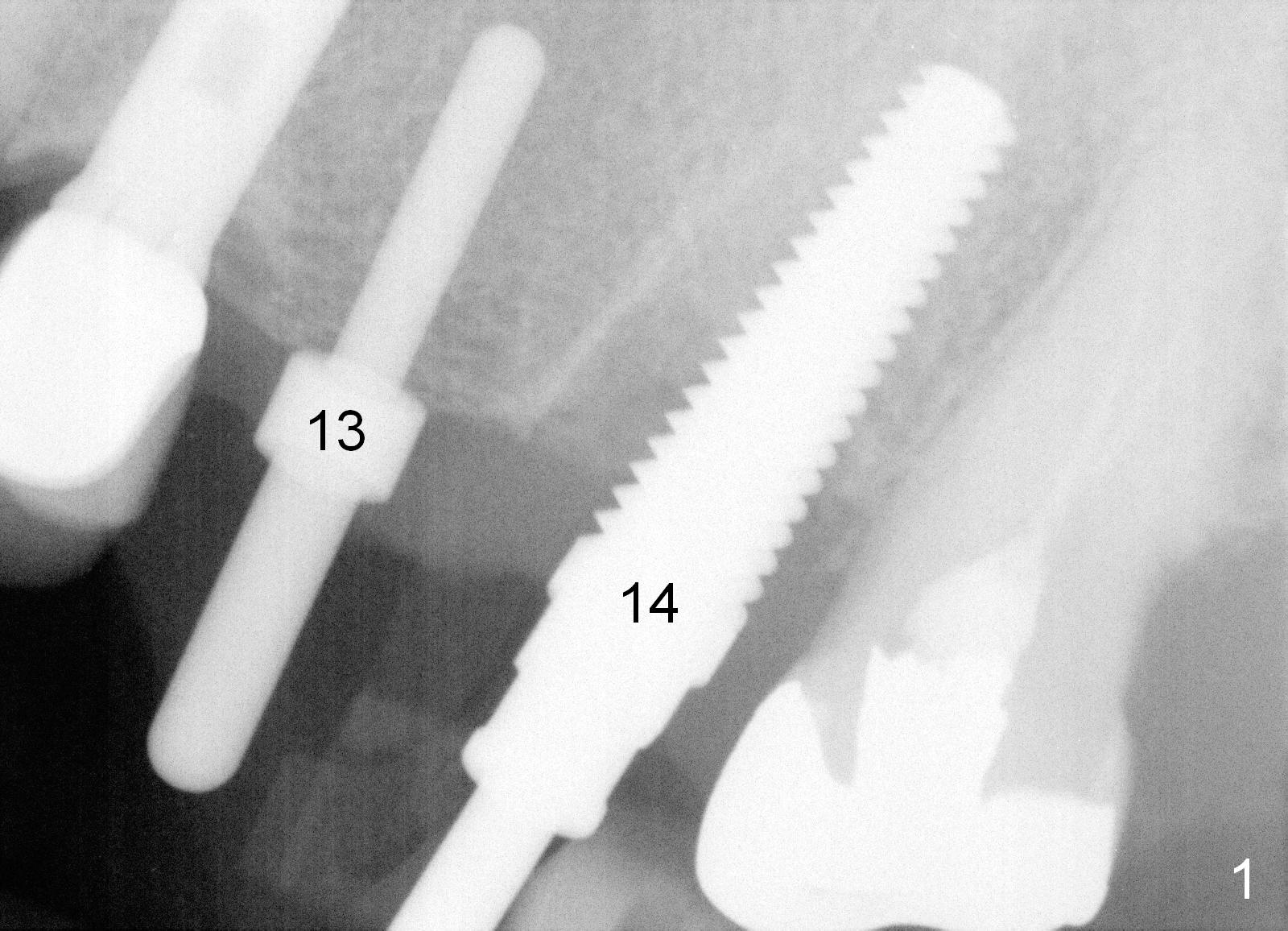
The tooth #14 is extracted by sectioning. The septum is robust and osteotomy is initiated slightly palatally. A 2 mm pilot drill is used, followed by 2.5-3.5 mm reamers (11 mm in the septal bone). Autogenous bone is harvested while reamering. When 4.5 and 5 mm taps are inserted, the coronal portion of the buccal slope of the palatal socket starts to be perforated. The last tap achieves stability (Fig.1: #14).
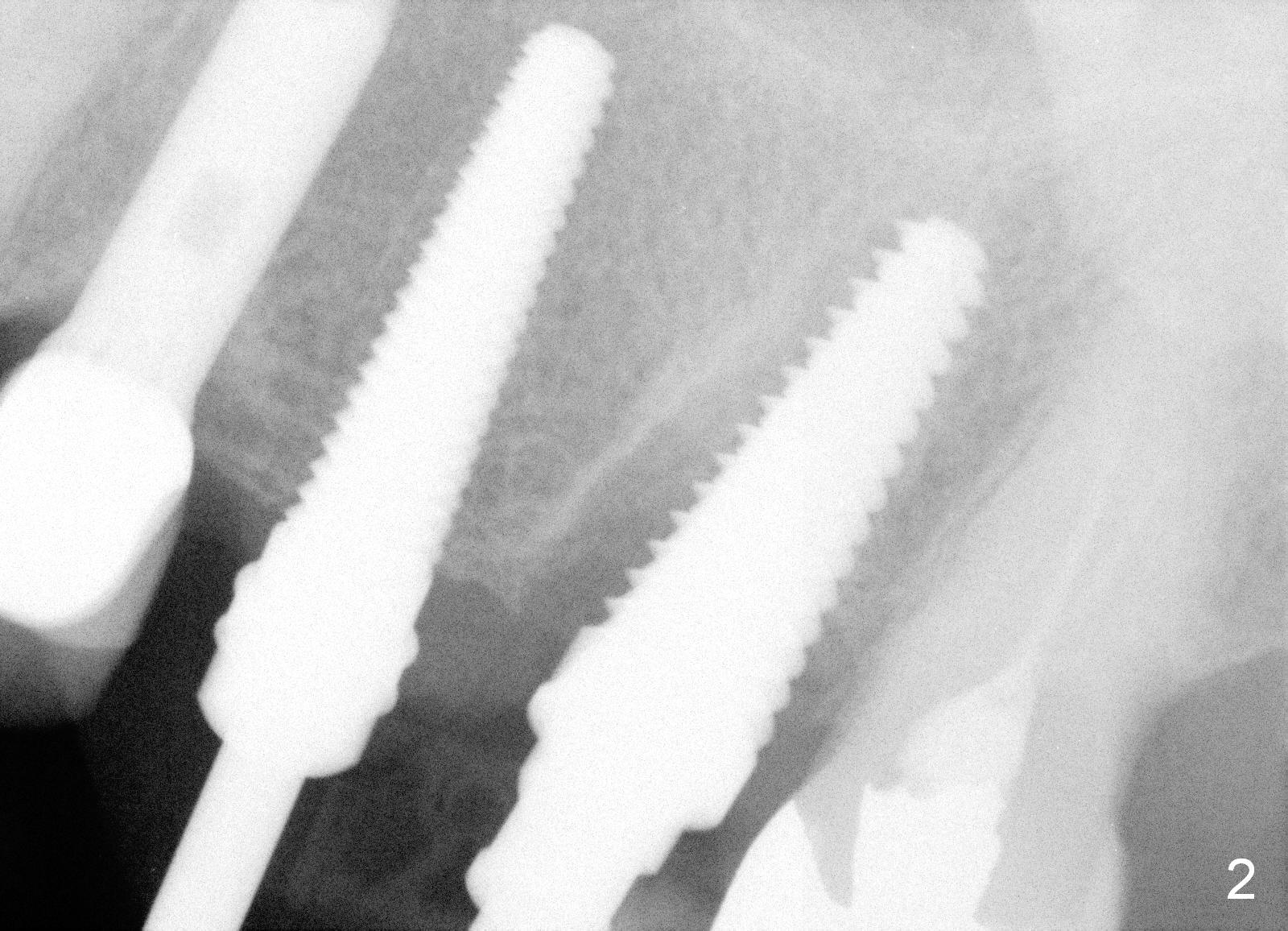
When a 2 mm pilot drill is used to initiate osteotomy at the healed site of #13 (Fig.1), the bone feels soft. No more drills or reamers are used. Instead the osteotomy is enlarged by bone expanders until 3.4 mm, followed by 4.5 mm tap (Fig.2). At this time, a 6 mm tap is placed at the site of #14 (Fig.2).
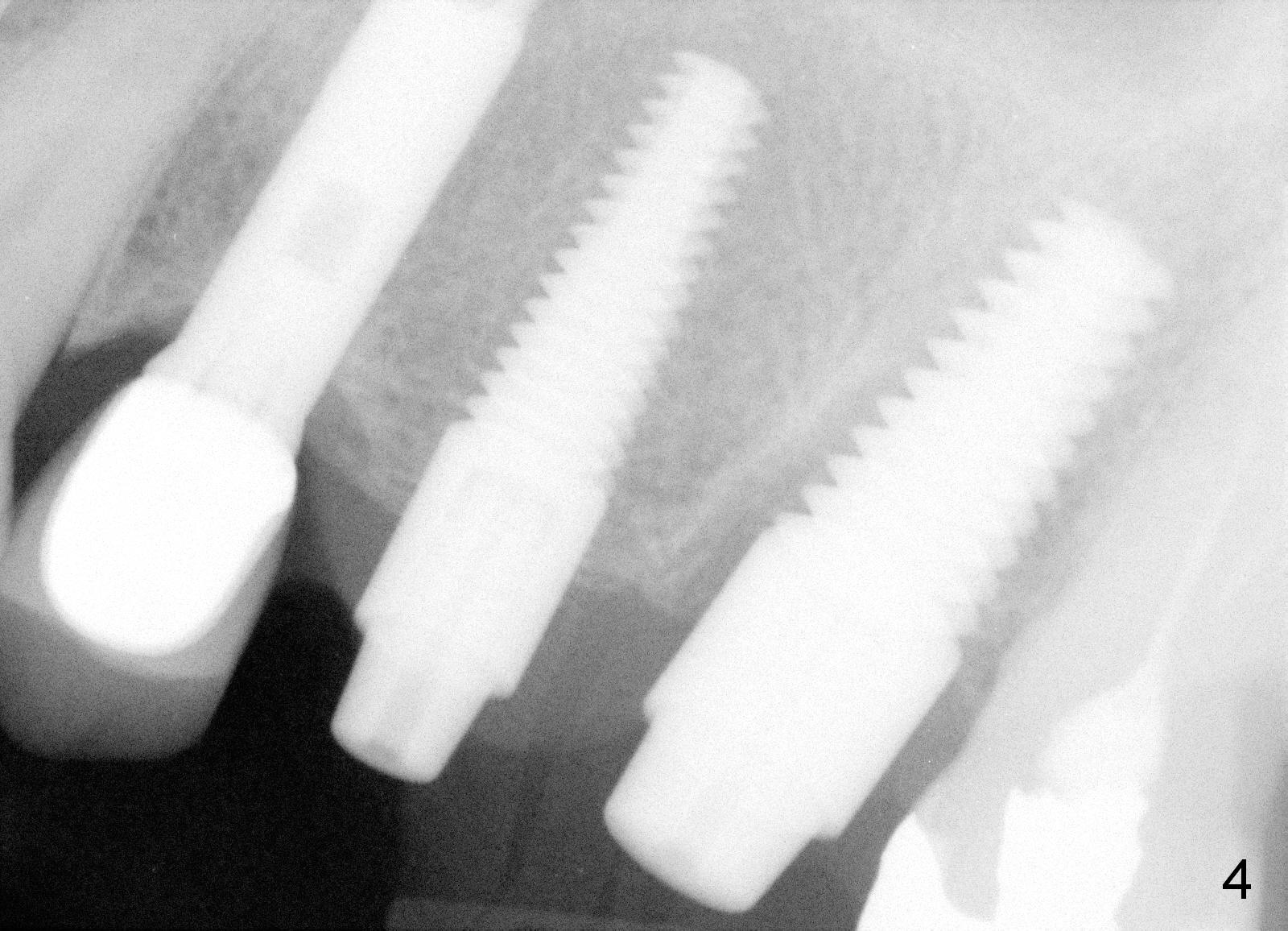
Finally 4.5x17 mm and 6x17 mm implants are placed at the sites of #13 and 14 with insertion torque ~ 45 and >60 Ncm, respectively (Fig.3,4). Bone graft is placed in the buccal and palatal gaps of #14 socket. Abutments are placed and an immediate provisional bridge is fabricated.
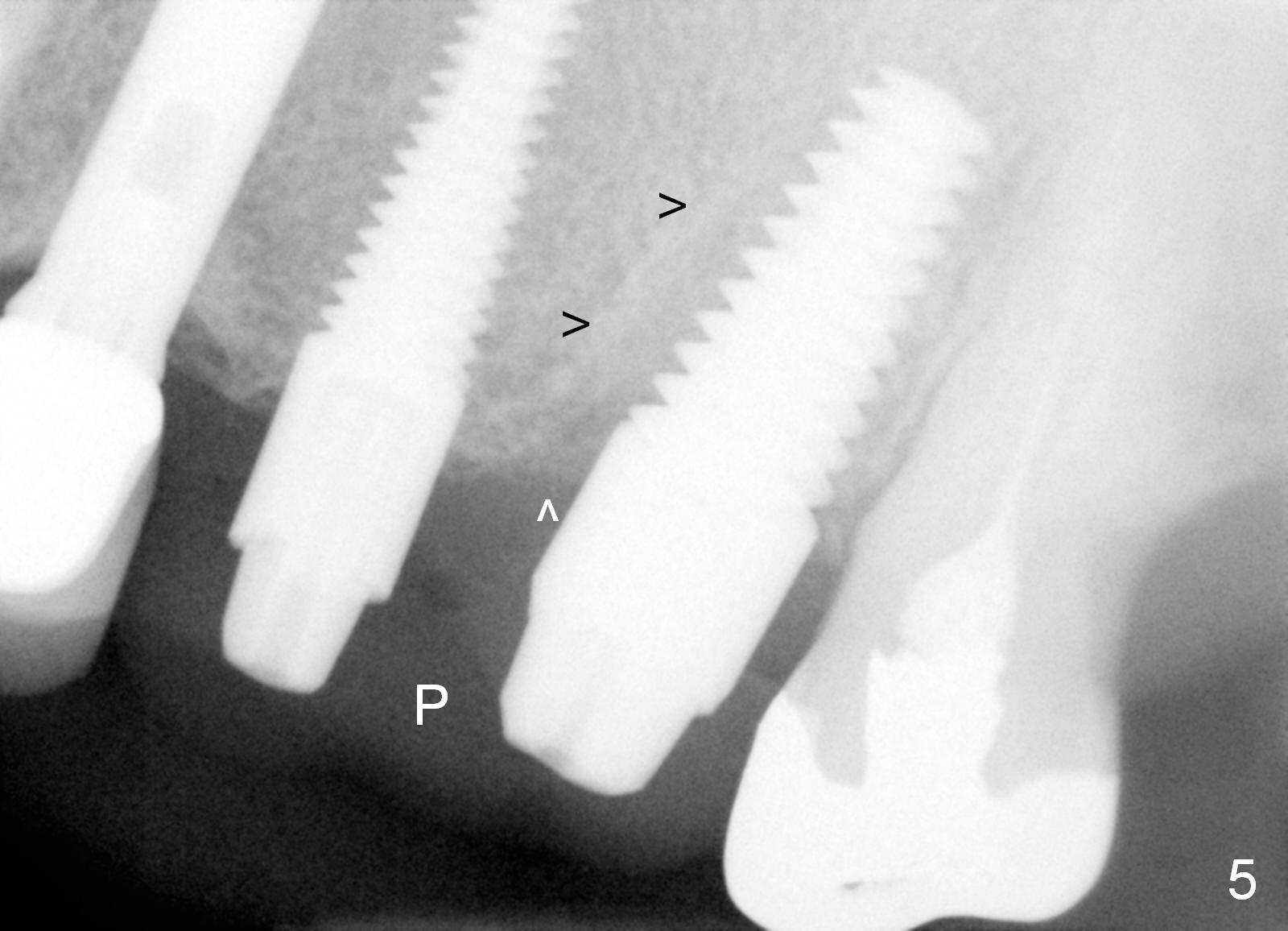
The splinted provisional remains in place 2 months 9 days postop (Fig.5 P). While the mesial lamina dura becomes fuzzy at the site of #14 (Fig.5 black arrowheads, as compared to Fig.4), the density of the mesial socket (white arrowhead) appears to have increased.
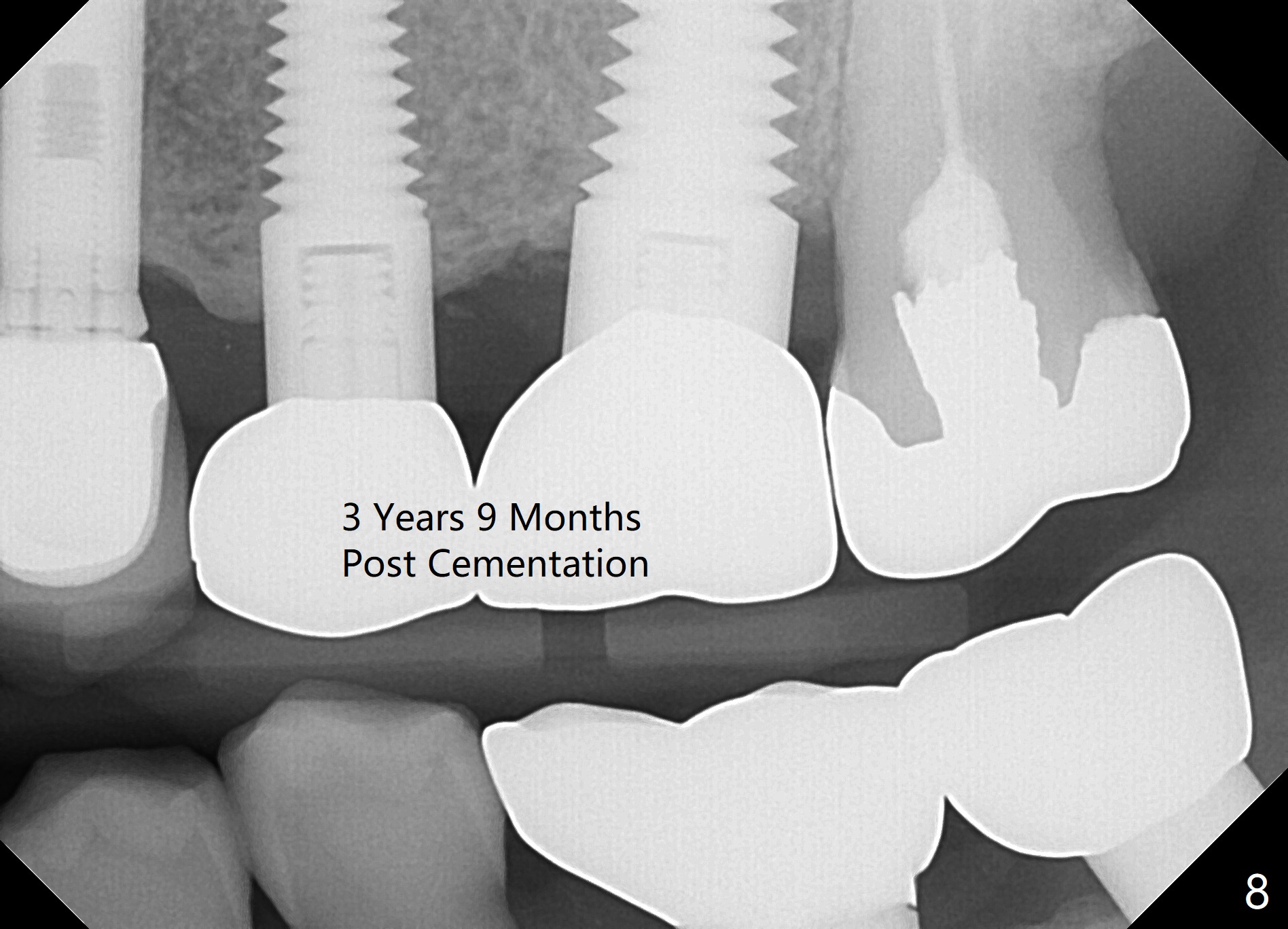
The papilla between #13 and 14 is maintained 4 months postop (Fig.6 *, as compared to preop), most likely due to the presence of the immediate provisional. The papilla (Fig.7*) will probably fill the embrasure between the high noble crowns at #13 and 14. There is no bone loss 3 years 9 months post cementation (Fig.8).
Return to Upper Molar Immediate Implant,
Posterior Immediate Provisional
#2
18
Xin Wei, DDS, PhD, MS 1st edition 05/05/2015, last revision 06/12/2019