|
|
|
|
|
As Simple As Possible
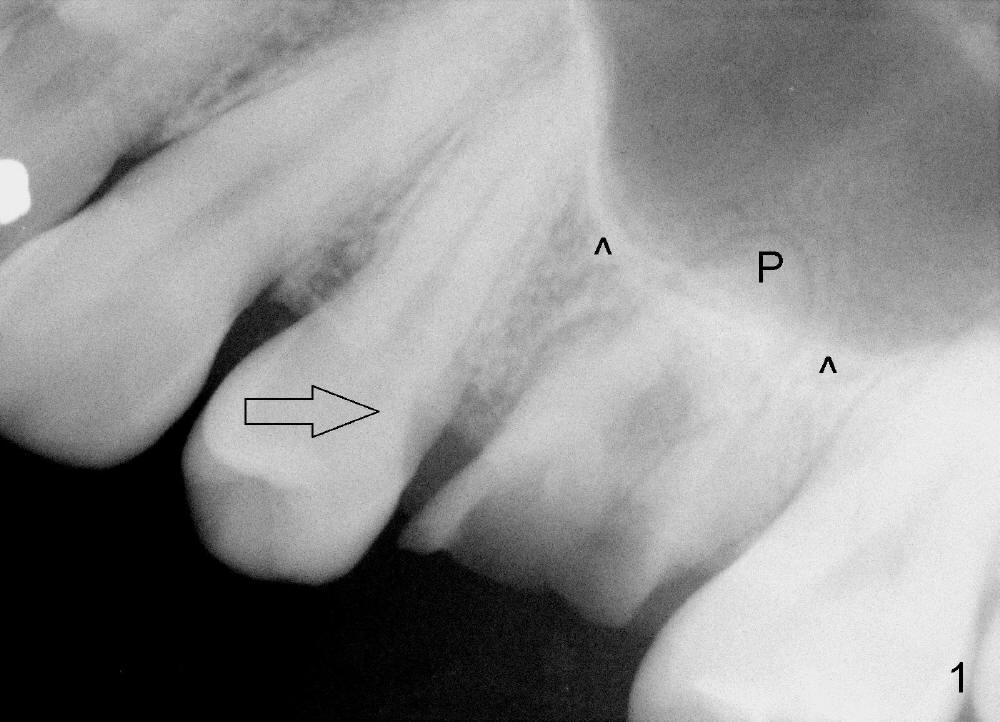
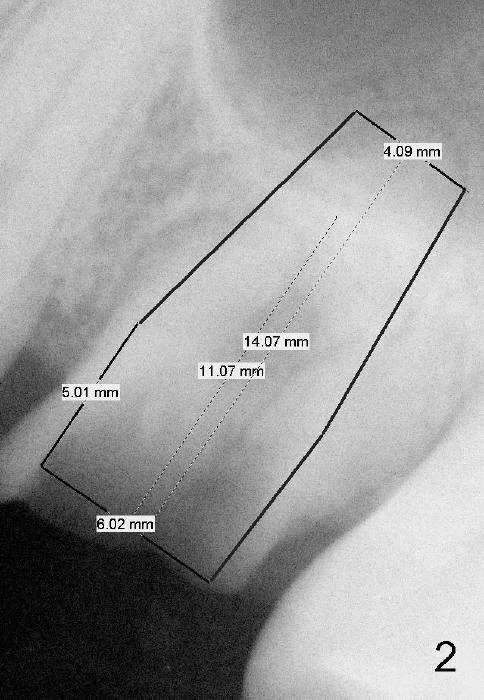
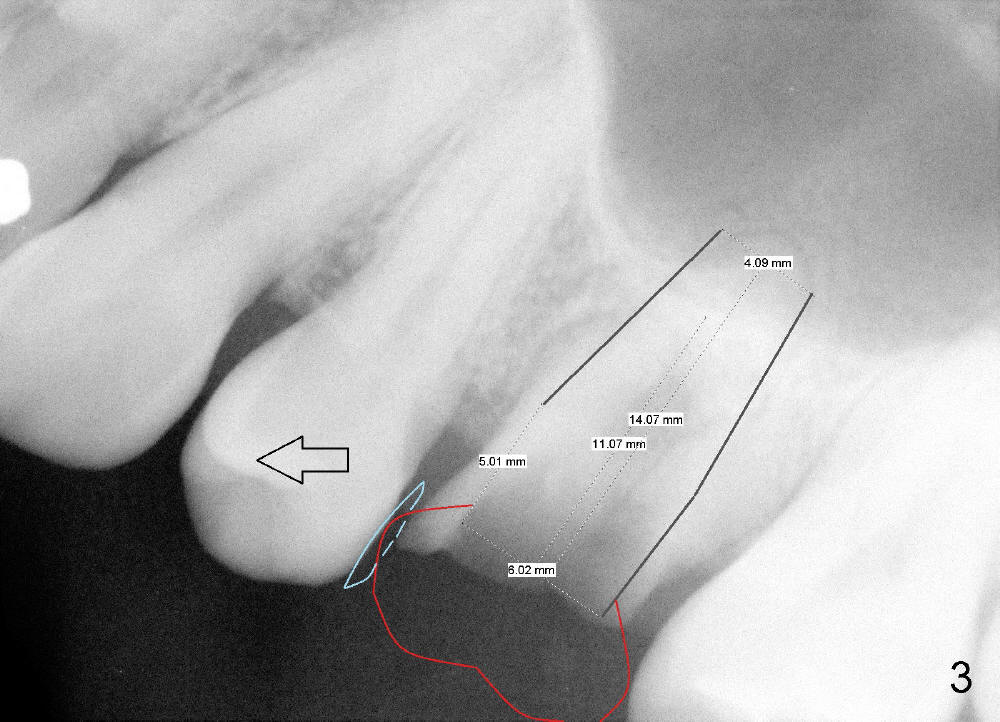
A 46-year-old lady is a dental phobic. She has had extraction ortho. The tooth #14 must have been nonfunctional for quite a while, as evidenced by distal shifting of the 2nd premolar (Fig.1 open arrow). The mesiodistal edentulous space is narrow. The diameter of the immediate implant should not be more than 6 mm (Fig.2). The bone height is somewhat limited, since the sinus floor (Fig.1 ^) is inferior to the palatal apex (P). After extraction, initial osteotomy depth is 11 mm from the gingival margin (~ 1 mm from the sinus floor). As the diameter of osteotomy increases, the depth can be eepened to 14 mm. Therefore the implant can be 6x14 mm (Fig.2); the height is between the sinus floor and the palatal apex. To prevent further tooth shifting during osteointegration, an immediate provisional will be fabricated (Fig.3 red). When osteointegration occurs, place a rubber separator between the provisional and the 2nd premolar (blue) so that the latter will gradually move (open arrow) back to its original place. A definitive restoration will be made.
Return to Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 01/02/2015, last revision 01/03/2015