




|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Why is the Sinus Membrane Perforated?
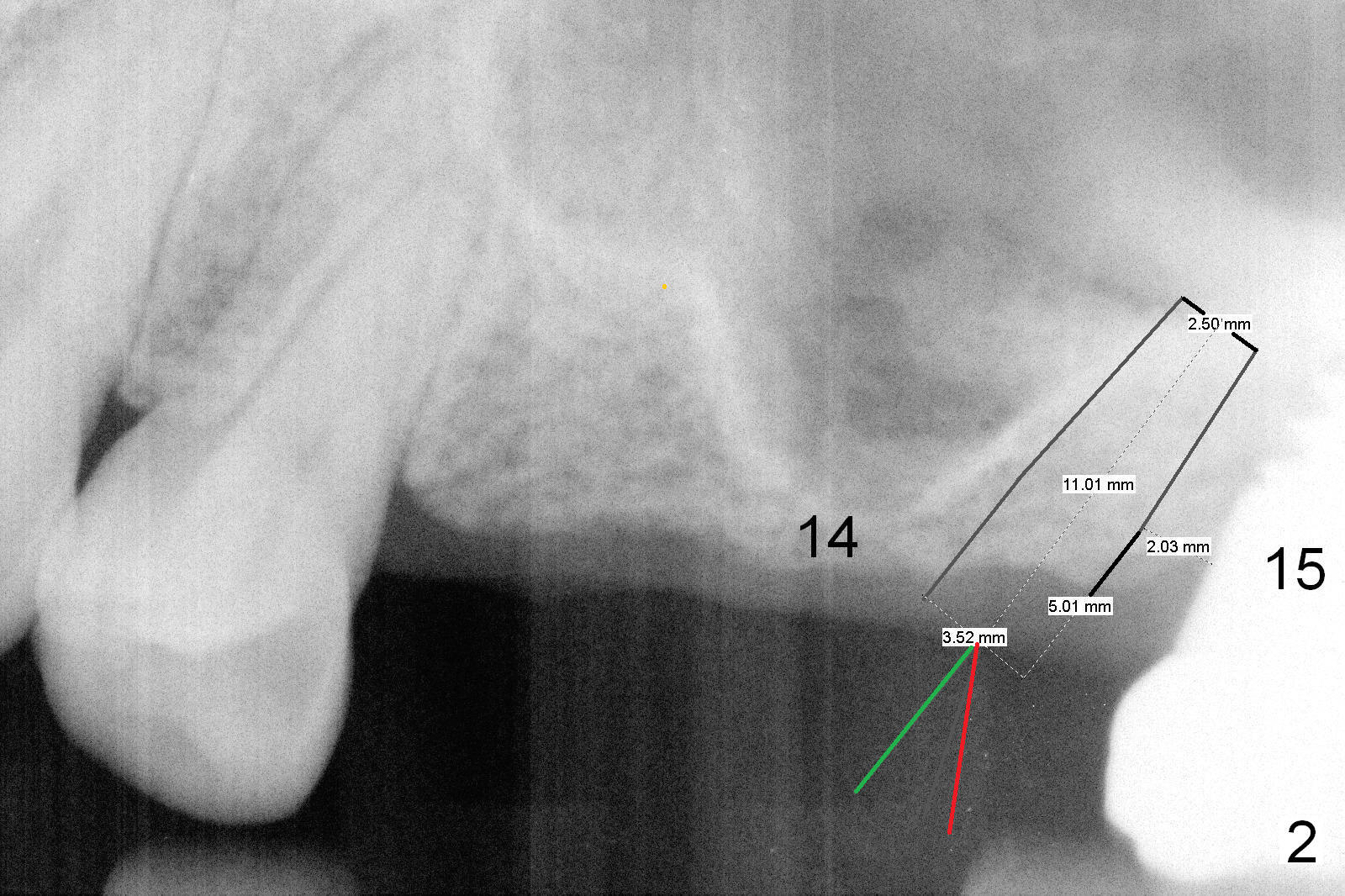
The ridge at the sites of #13 and 14 are large (Fig.1). Considering limited bone height at the site of #14, one alternative is to place a small implant obliquely between #14 and 15 (Fig.2: 3.5x11 mm), use an angled abutment (red line) and fabricate an atypical bridge between #13 and 14/15. This approach is not adopted, since there is 2 mm between the oblique implant and the one at the site of #15.
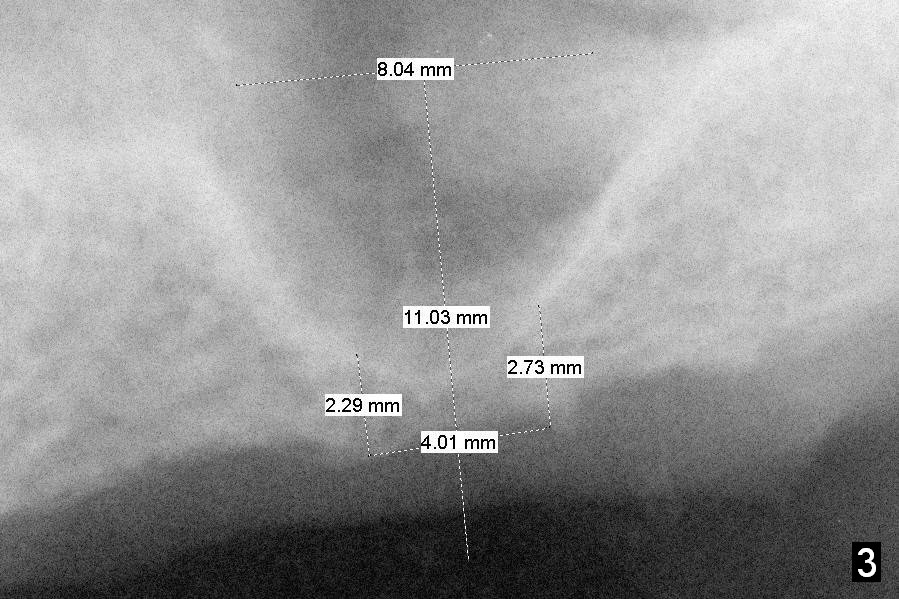
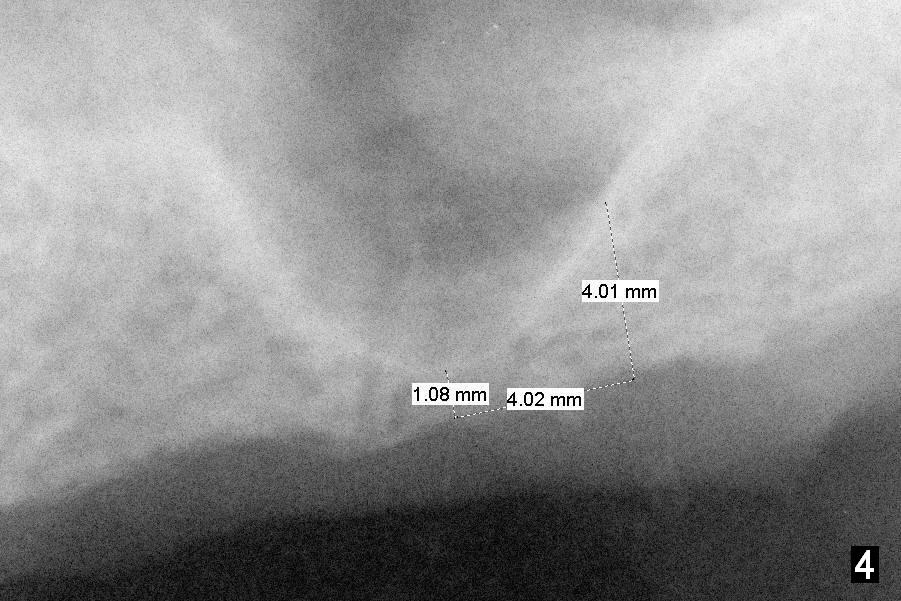
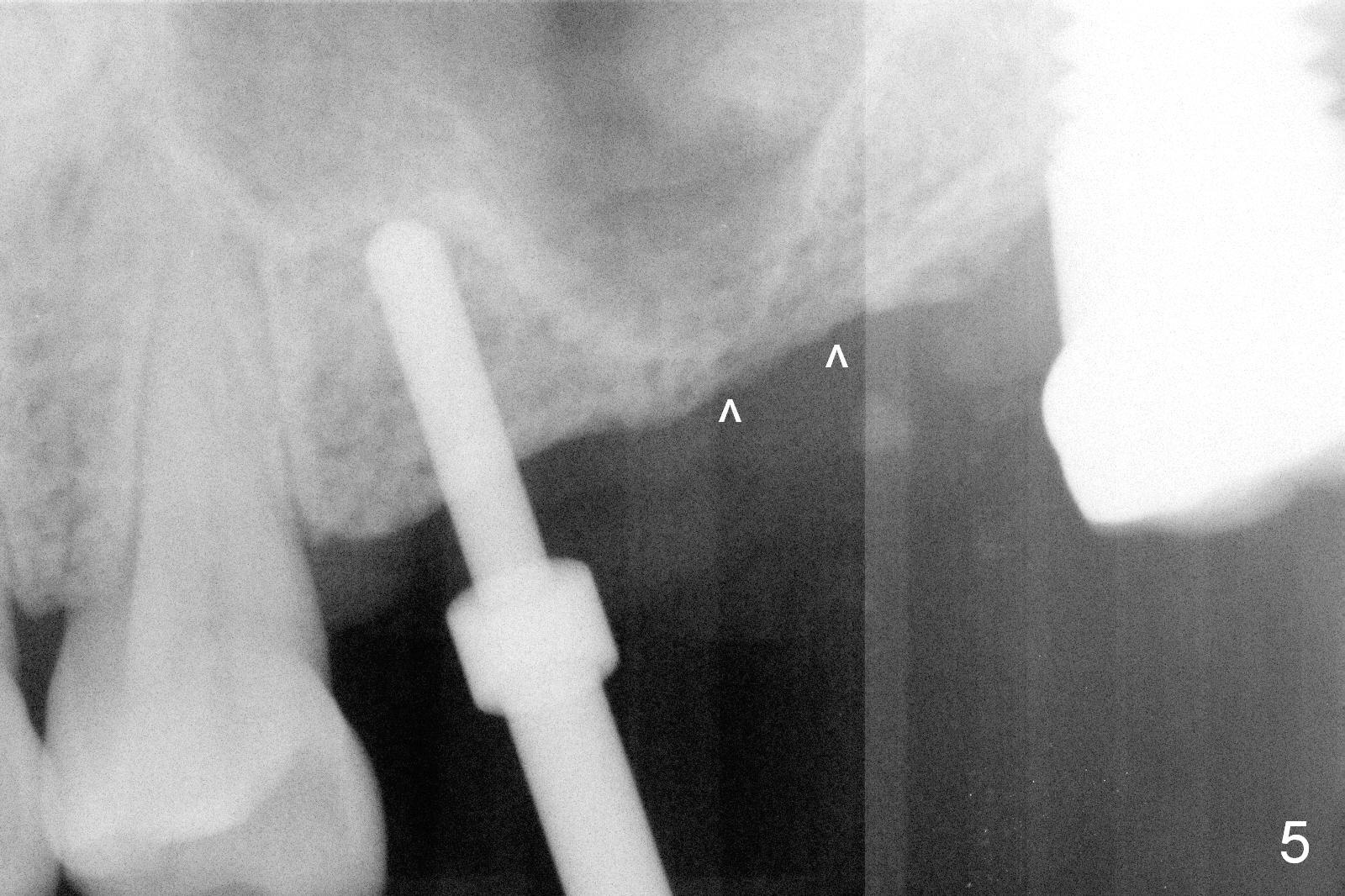
A 4 mm trephine bur is used to initiate osteotomy at the site of #14 for 2 mm deep, which should not perforate the sinus membrane (Fig.3). In fact, there is air leakage after trephine bur. When the bone block is pushed upward with an osteotome, the mesial sinus floor is approximately 1 mm thick, whereas distal ~ 4 mm (Fig.4, 5 (arrowheads)). The sinus membrane is perforated apparently non-reparable with collagen dressing (Impladent) packing.
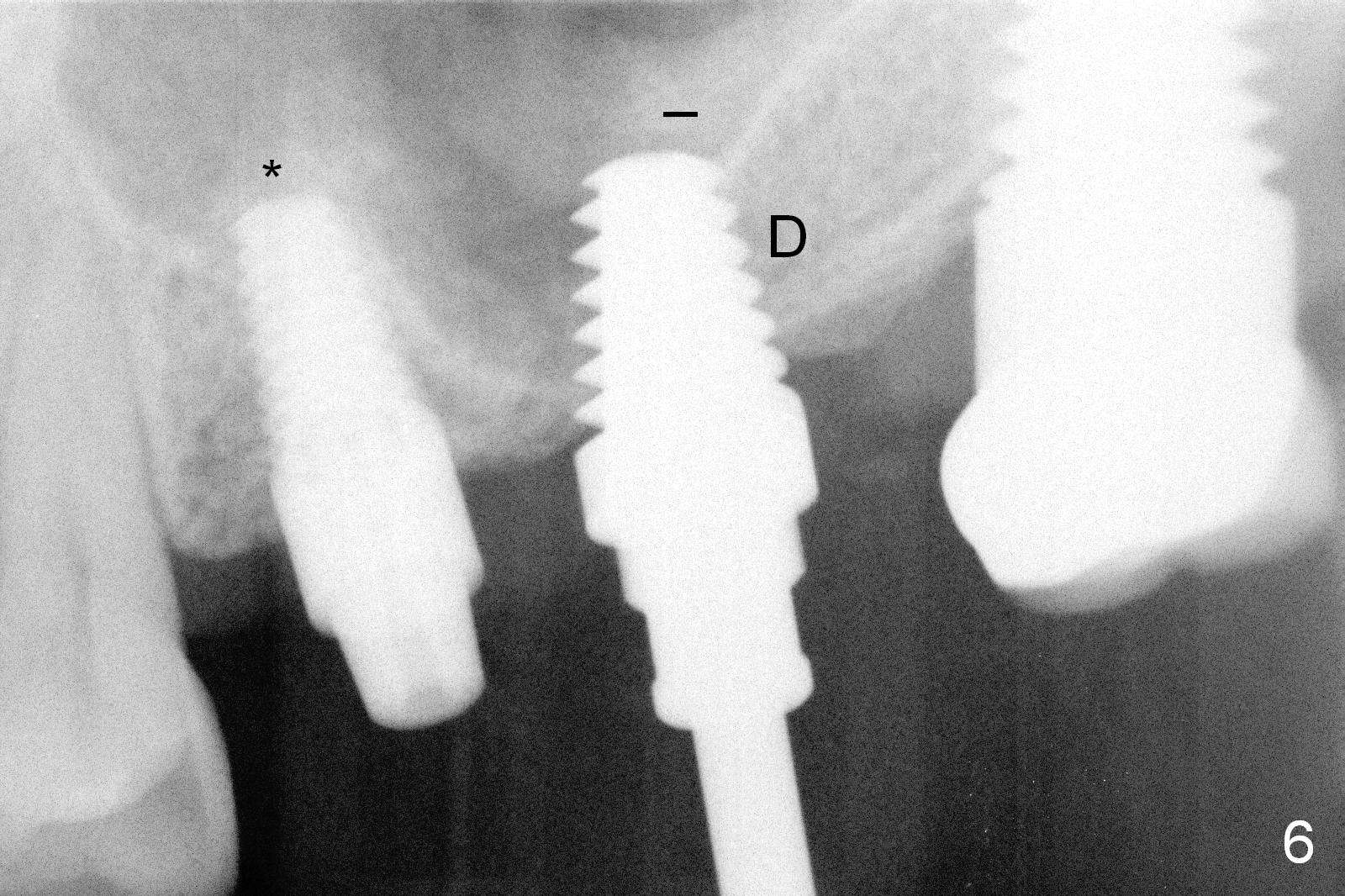
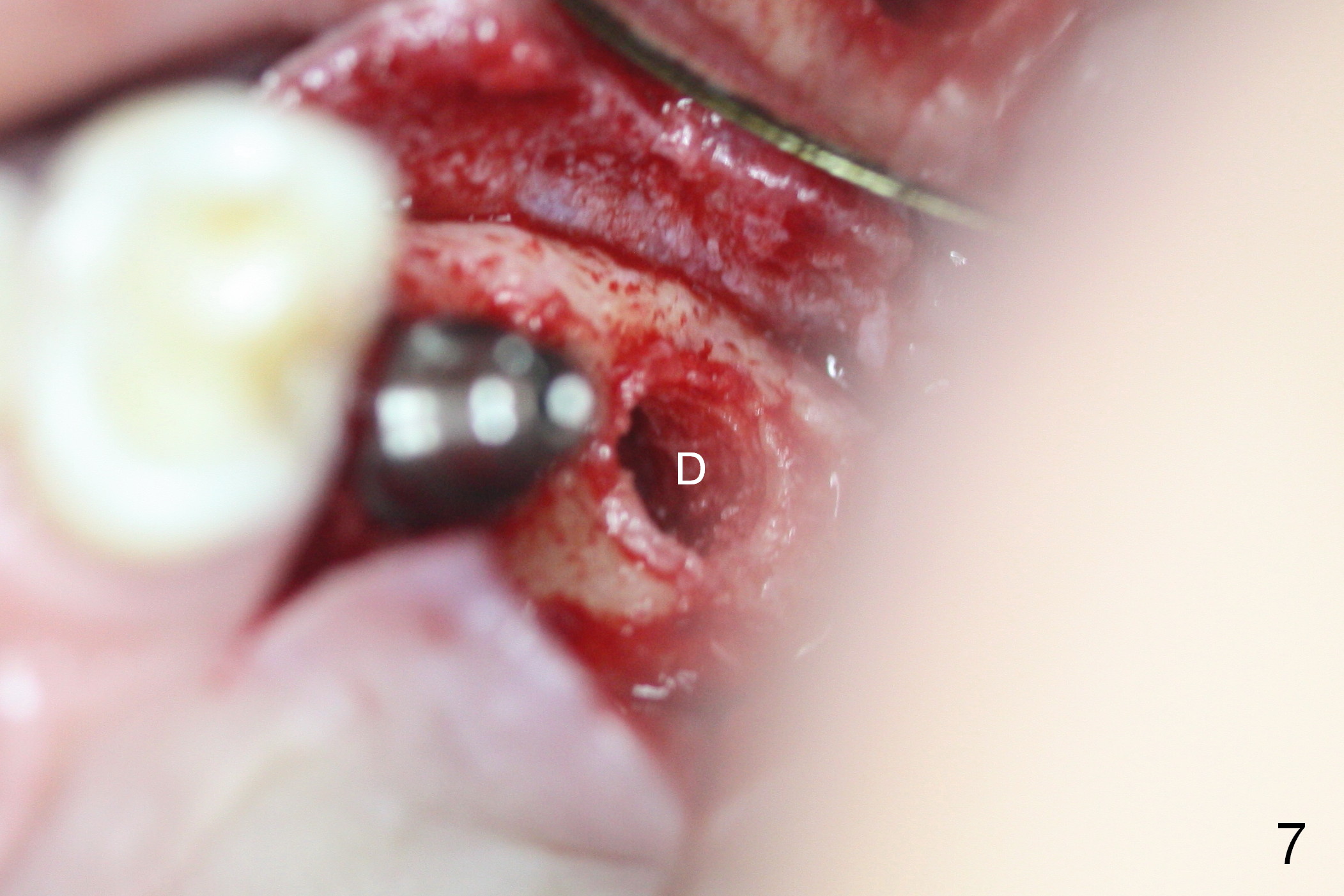
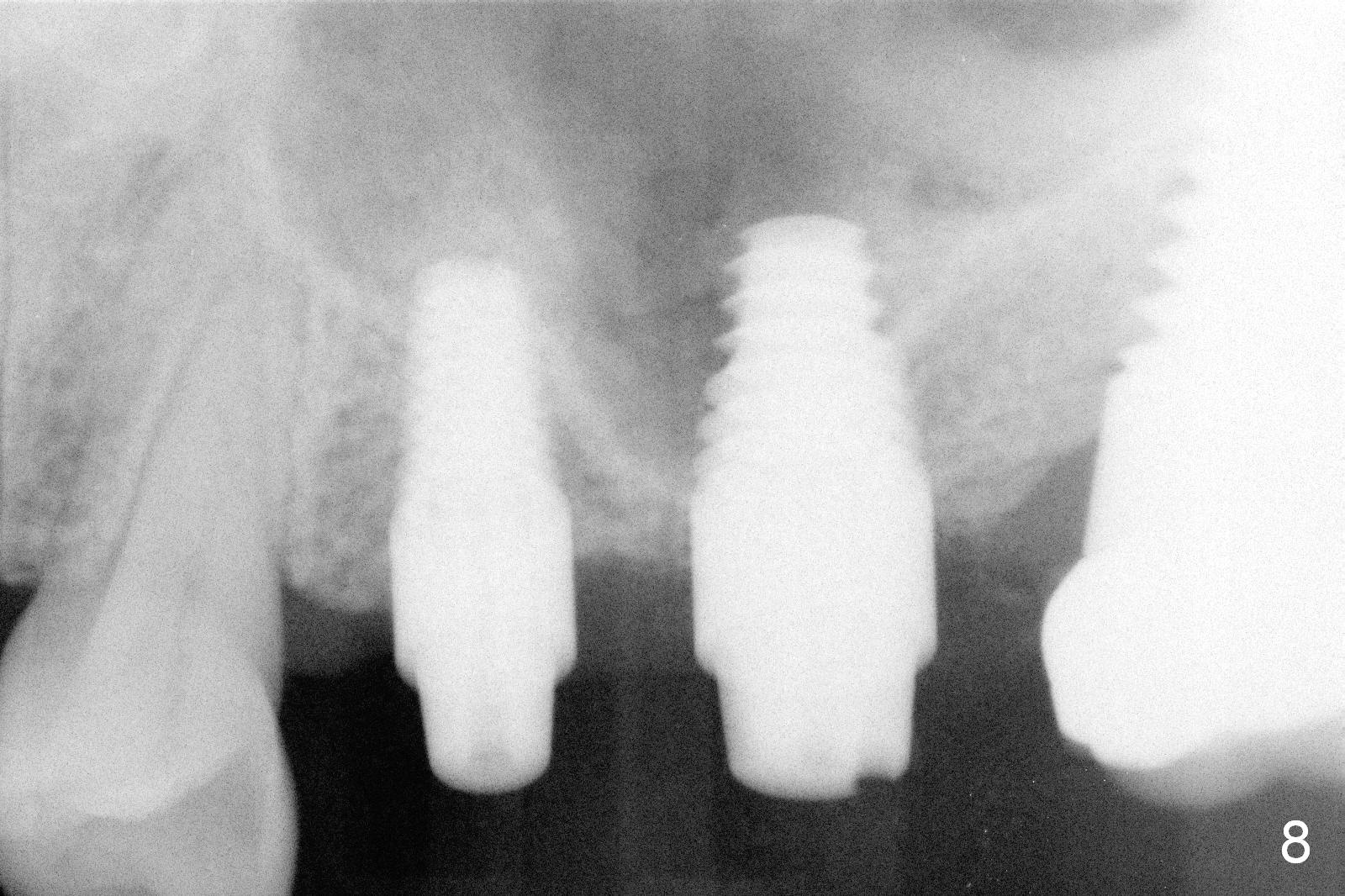
Osteotomy starts at #13 (Fig.5). A 4.5x11 mm implant is placed with insertion torque >60 Ncm (Fig.6), suggesting high bone density. Why not place an implant at #14? A 6x11 mm tap is inserted with high torque with thick bone distally (Fig.6 D). When the tap is removed (Fig.7), there is a lip of bone displaced apical to (but continuously connected to) the distal bone (Fig.6 a black transverse line). Finally a 6x11 mm implant is placed with insertion torque >60 Ncm (Fig.8). The mesial threads appears not to be covered by one. Prior to implant placement, a small amount of bone graft is placed at the osteotomy and sprinkled over the implant threads. It is wish that more of collagen dressing were used to form the superior (apical) seal before placing more of bone graft in the sinus.
There is mild nasal hemorrhage or discharge for a few days postop. Other than that, the patient is doing well. Perio dressing is dislodged ~ 2 weeks postop. The wound appears to heal 4 weeks postop; the abutments are removed to reduce bite interference (Fig.9). While he was visiting China, the implant at #14 fell out. We may have to redo the case using Sinus Master kit.
The latter should help reduce sinus perforation and perform sinus lift (prepare Metronidazole and bone graft). Also use a UF implant so that threads can directly contact the native bone (vs. smooth surface of Tatum implant contacting the mesial wall). Last splint the two provisional crowns if there is enough occlusal clearance (vs. perio dressing last try). Use an abutment with the shortest cuff (6.5x4(1) mm)). Also prepare 4.5x11 mm tap.
In fact the patient does not want to try again (Fig.10, 7.5 months postop). Two weeks later, a crown is cemented at #13 (Fig.11,12).
Return to Upper Molar Immediate Implant,
Professionals,
IBS training
Xin Wei, DDS, PhD, MS 1st edition 05/20/2015, last revision 09/28/2016