
.jpg)



|
|
|
|
||
|
|
|
|
||
|
|
|
|
|
|
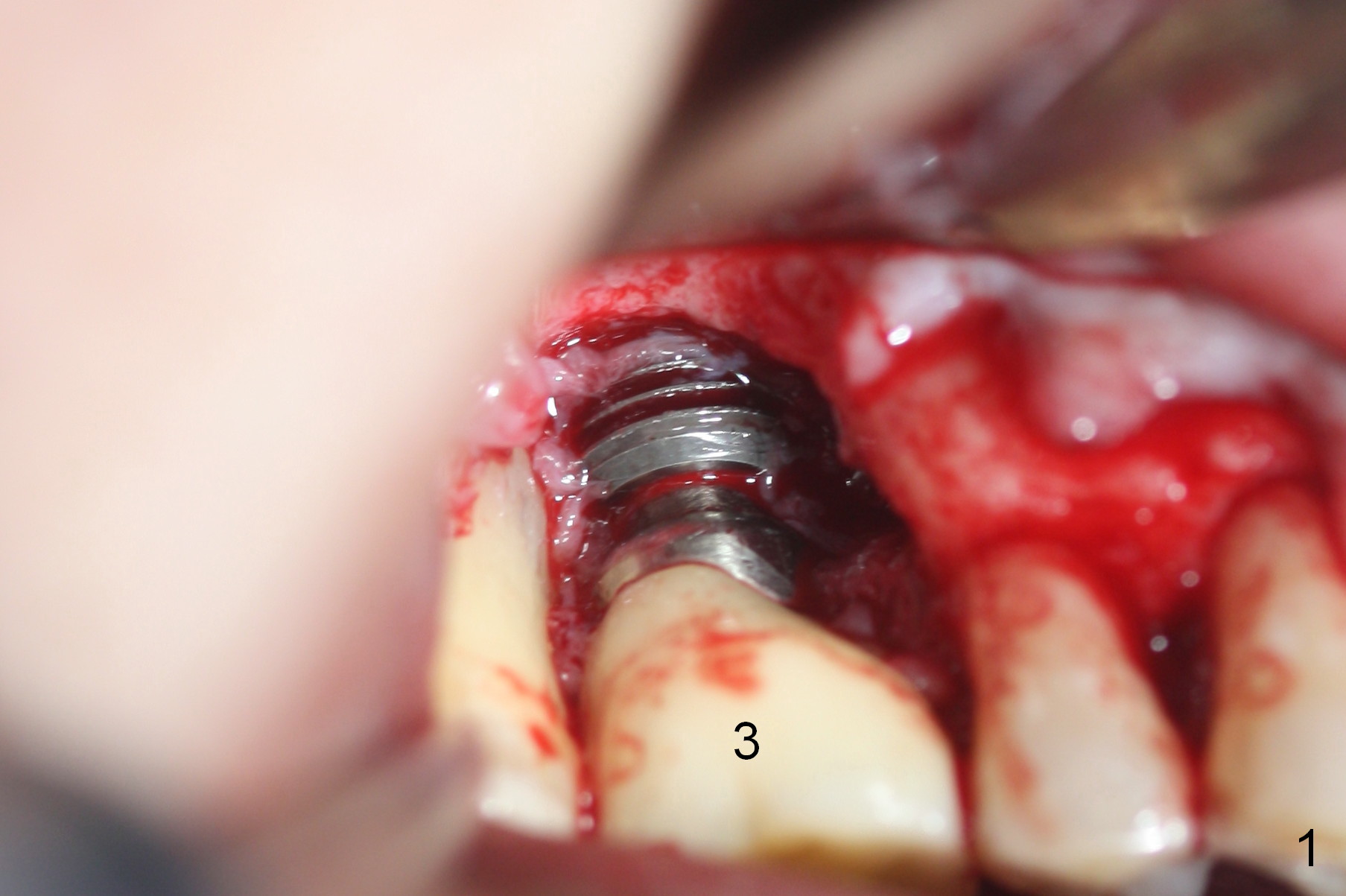
1-2 mm Allograft to Cover Exposed Implant Thread
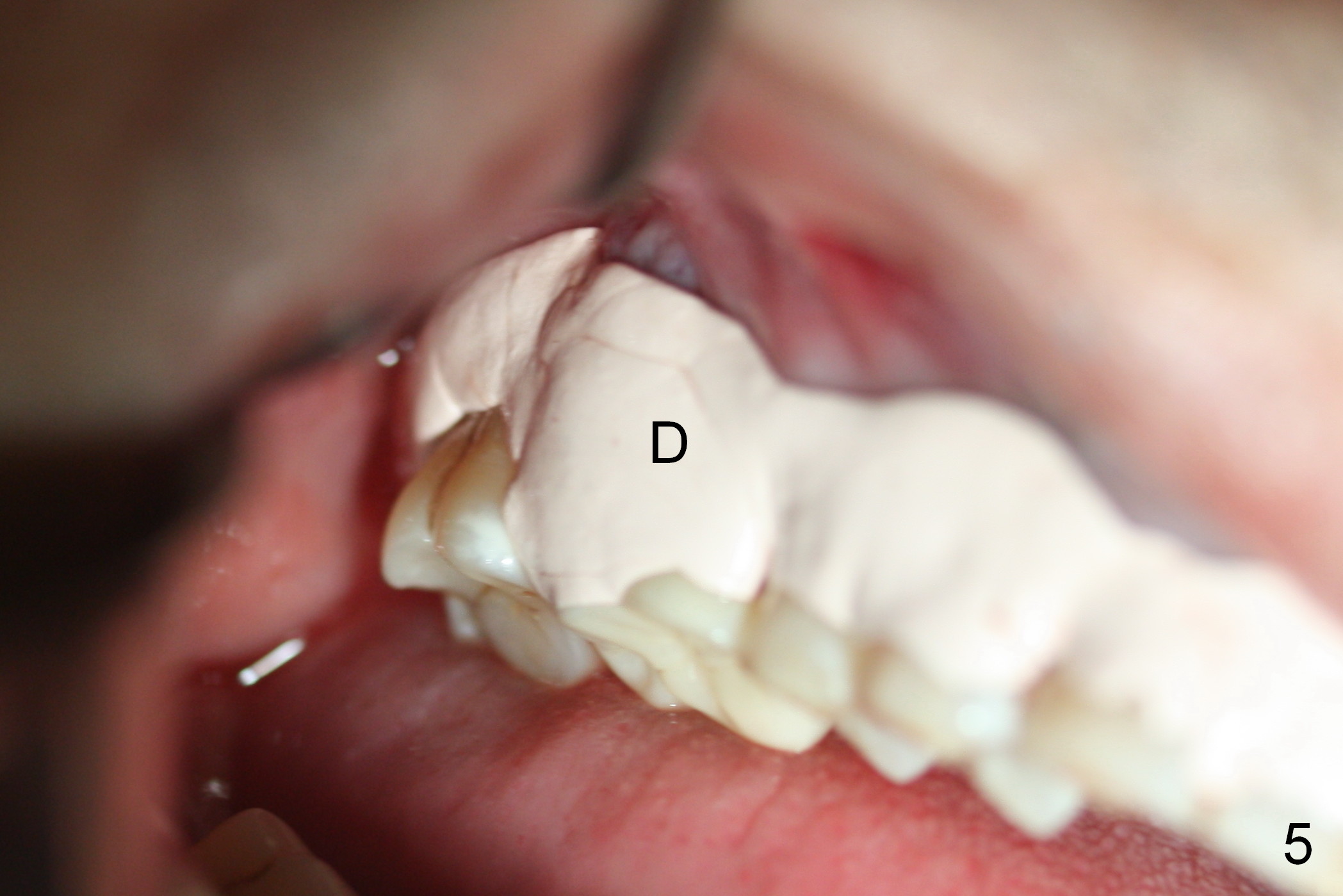
Envelop flap reveals buccal implant thread exposure (Fig.1 after granulation tissue removal). It appears that a block graft does not fit the defect. Instead 1-2 mm mineralized cortical and cancellous allograft mixed with Osteogen is placed (Fig.2,4 *). The graft is covered by resorbable (Fig.3 white *) and nonresorbable (black *) membranes. Peridontal dressing is applied (Fig.4 D). One week postop, the periodontal dressing has dislodged; the non-resorbable membrane appears to adhere to the crown; the gingiva appears to recede (Fig.6 arrow). The patient is scheduled to return for removing the non-resorbable membrane in 4 weeks.
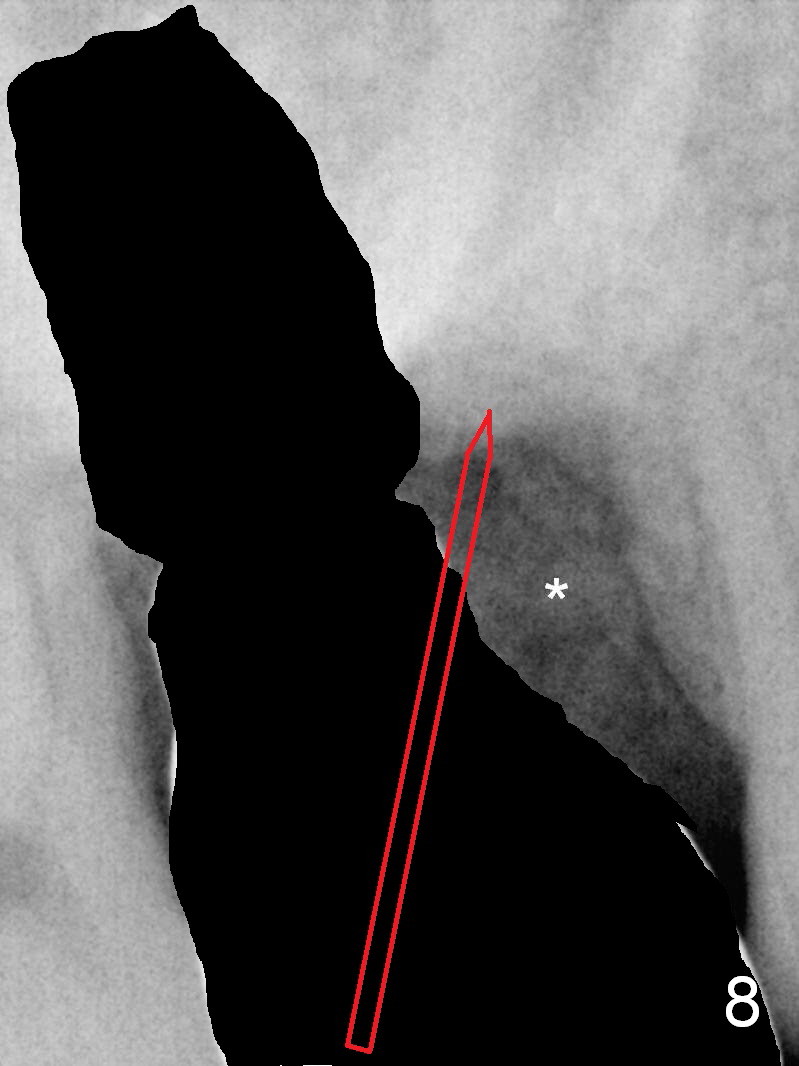
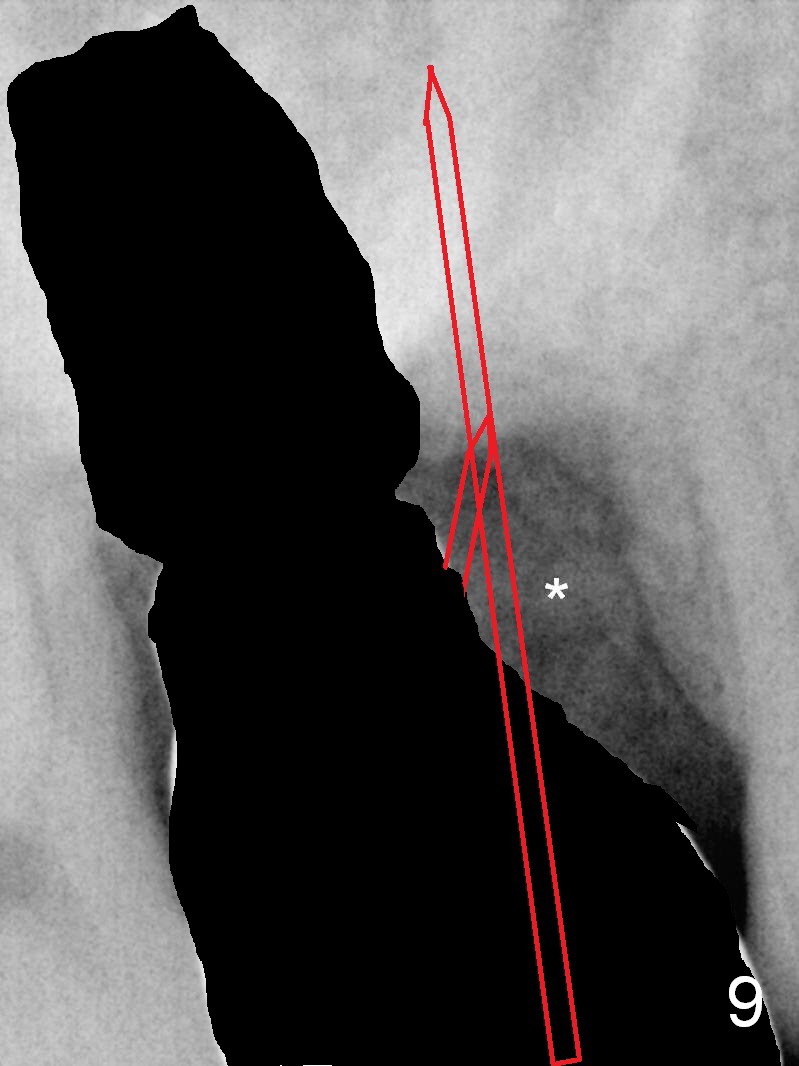
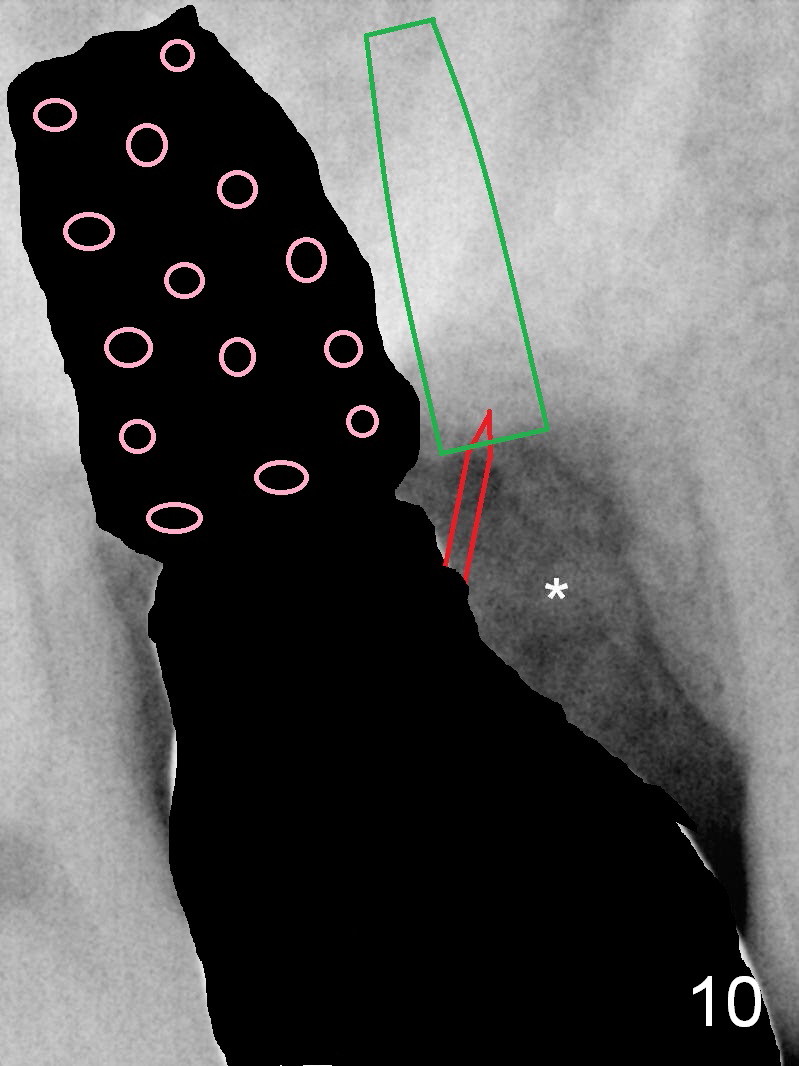
In fact the membrane is dislodged by itself with re-exposure of threads (Fig.7 (1 month post grafting)). Since the implant is malpositioned and oversized, it should be removed. Prepare Dialite bur(s) and crown removals. After Metronidazole treatment and irrigation, a new osteotomy site is gained mesially (Fig.8 red arrow). Once bony entrance is obtained, change trajectory (Fig.9). Use 5 mm stopper and 2 mm pilot drill from Sinus Master Kit, followed by the smaller round drill to obtain proper depth. When the smallest UF implant achieves primary stability (Fig.10 green), try the largest cemented abutment. Then remove the latter, insert a piece of cotton pellet into the implant well, and pack bone graft until the platform of the implant (Fig.10 pink). Remove the cotton pellet, tighten the abutment, place more bone graft around the abutment until its margin and fabricate an immediate provisional to seal the defect opening. Also prepare Emdogain so that bone may form over the exposed root of the tooth #2 to reduce sensitivity.
If the implant does not seem to be too distally placed clinically with relatively intact buccal wall and the implant is able to be torqued more apically, remove it, clean outside the mouth with Titanium brush and return to the same osteotomy site with higher position (sinus lift). The rest of the procedure is shown above.
In brief, avoid incision to reduce trauma and promote healing.
Return to Upper Molar Immediate Implant,
Berkeley
Xin Wei, DDS, PhD, MS 1st edition 01/25/2016, last revision 03/03/2016