

|
|
|
|
||
| Fig.1 | Fig.2 | Fig.3 | ||
|
|
|
|
||
| Fig.4 | Fig.5 | Fig.6 | ||
|
|
|
|
|
|
| Fig.7 | Fig.7' | Fig.8 | Fig.9 | Fig.10 |
Stability Derives from Engagement to Sinus Floor
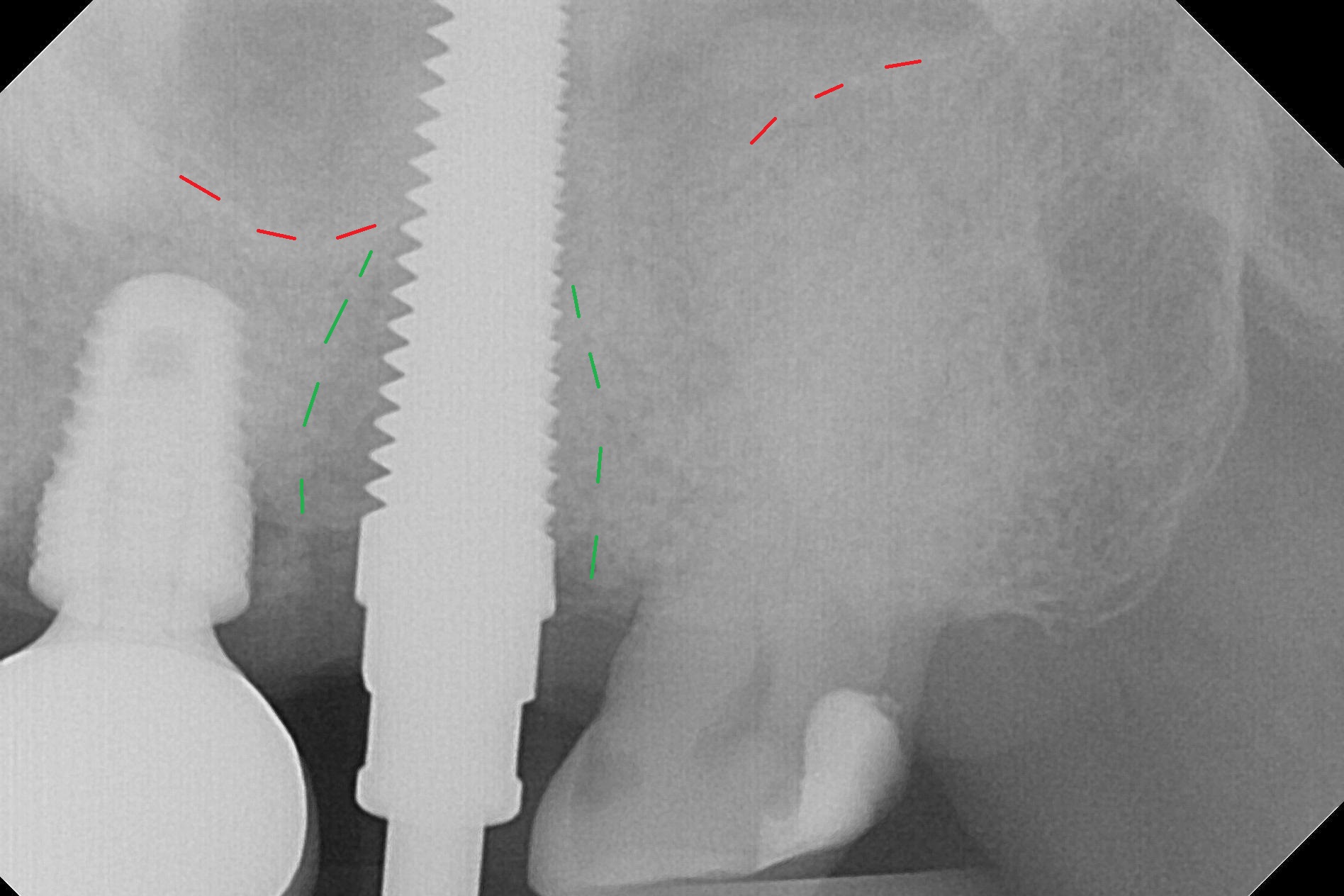
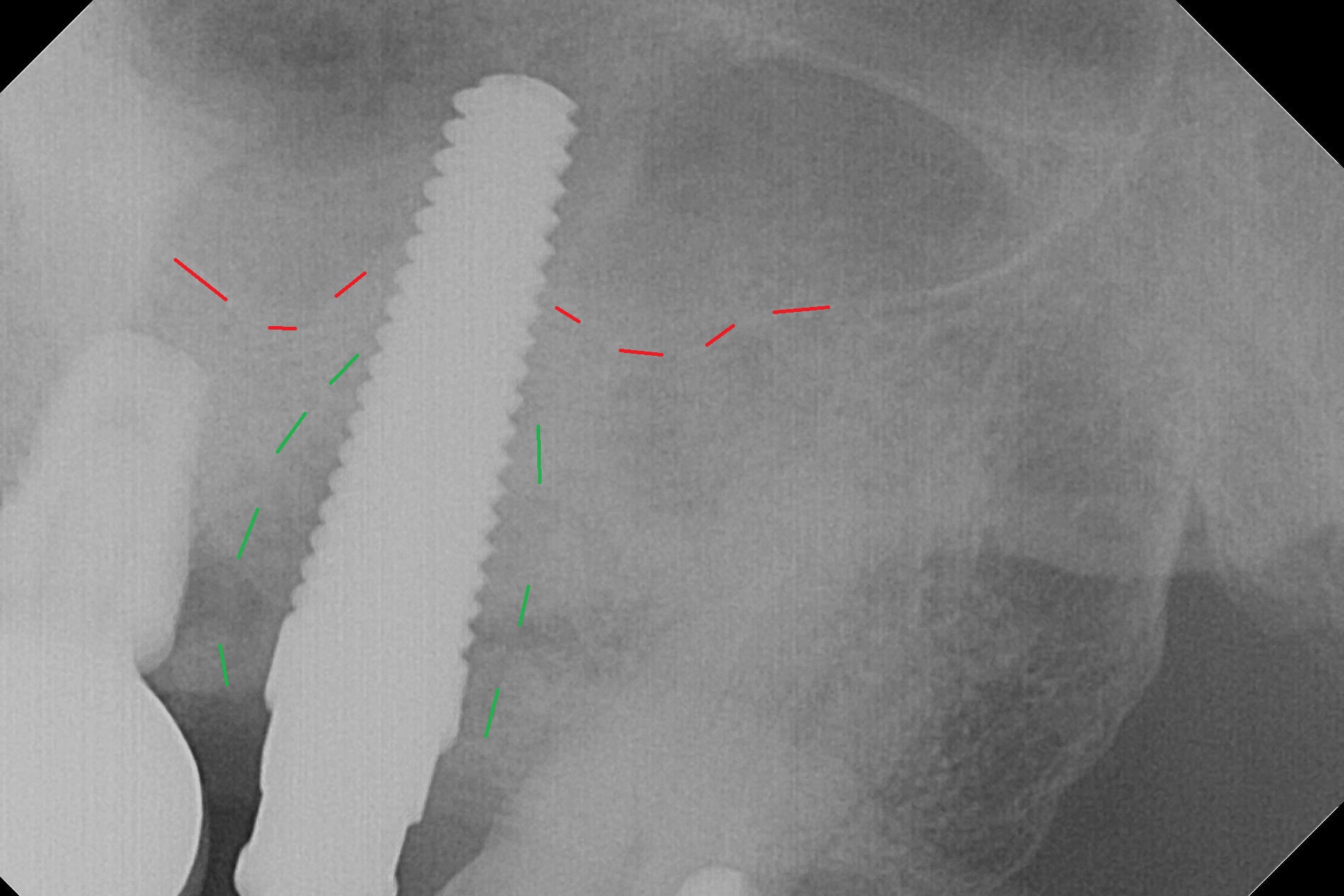
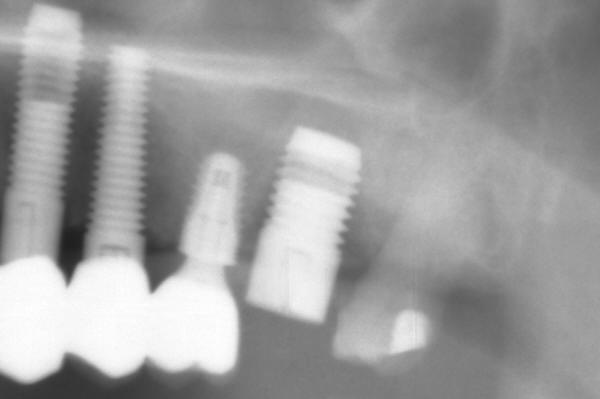
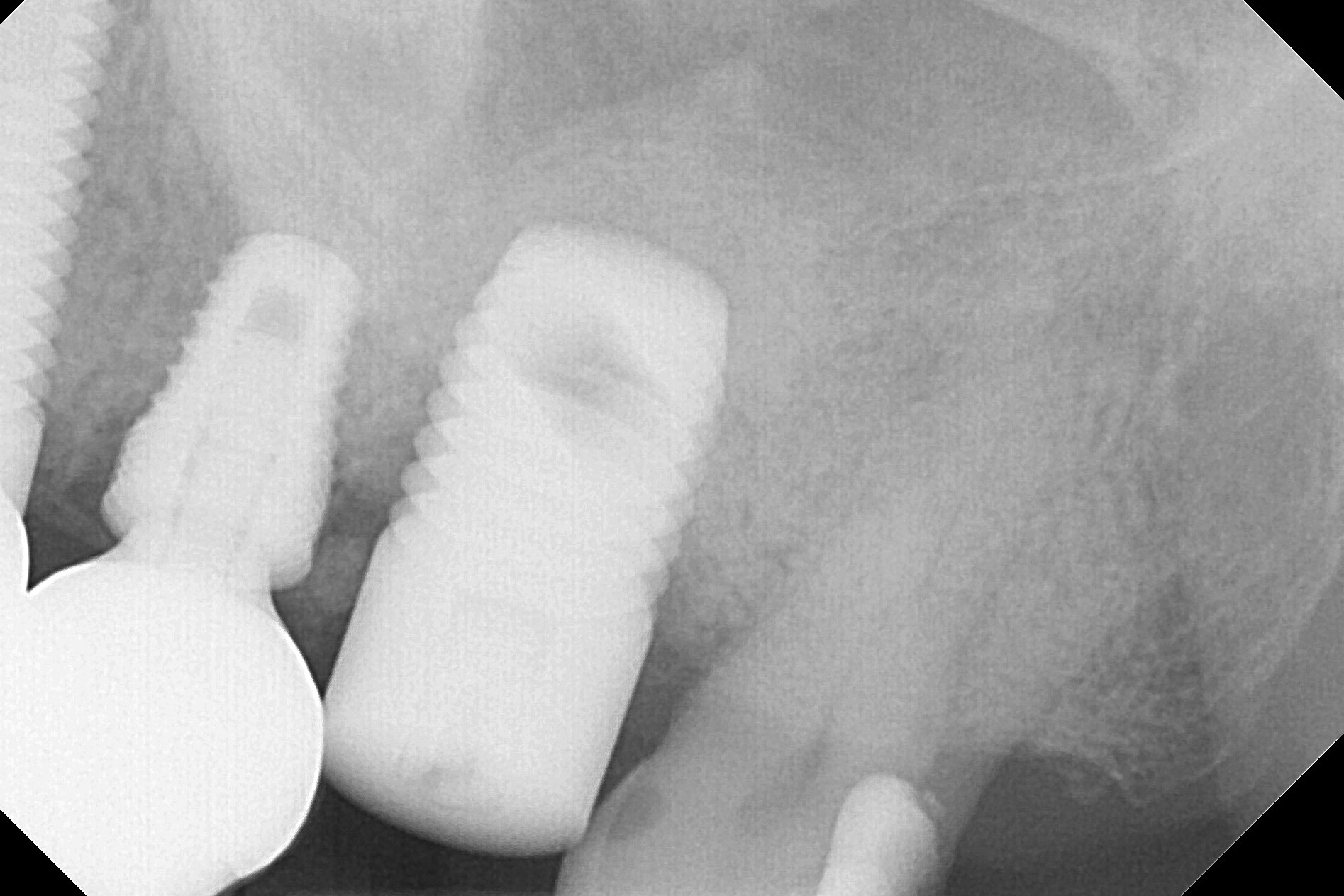
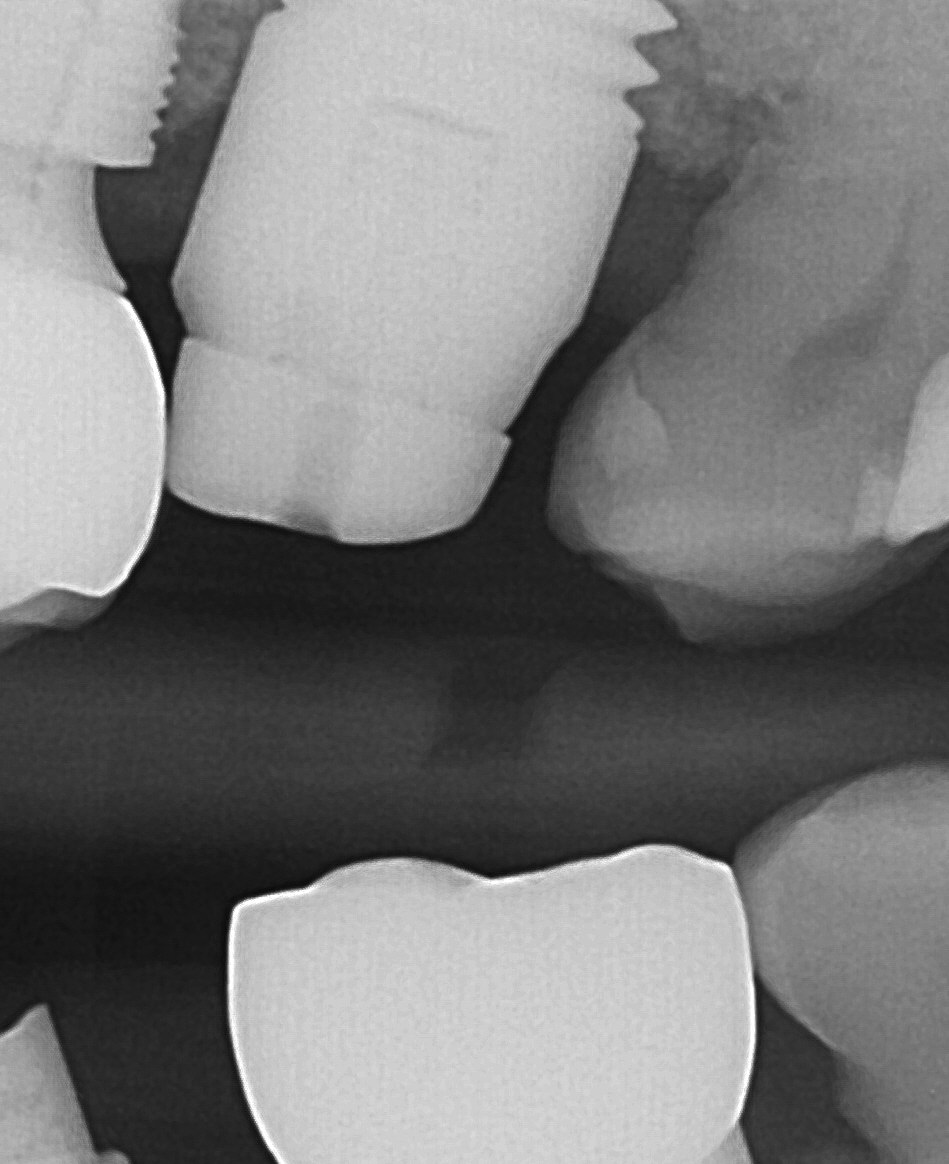
Seven days post implant removal without debridement, RT2-4 are tapped for 14-17 mm, followed by 5x20 mm tap for 17 mm (Fig.1,2). In fact the sinus membrane perforates. With an increase in tap diameter, the stability does not increase, since soft bone is being removed from the osteotomy wall. By the time a 8x17 mm tapered tap is inserted for 14 mm, the restorative space (mesiodistal) is violated (Fig.3,4). A 7x14 mm cylindrical tissue-level implant is placed with ~ 20 Ncm (Fig.5,6) only after use of 7x14 mm tapered drill appears to have penetrated the sinus floor.
When the osteotomy is large with soft bone, implant stability depends on the engagement into the apical bone (around the sinus floor), in which the bone density is high.
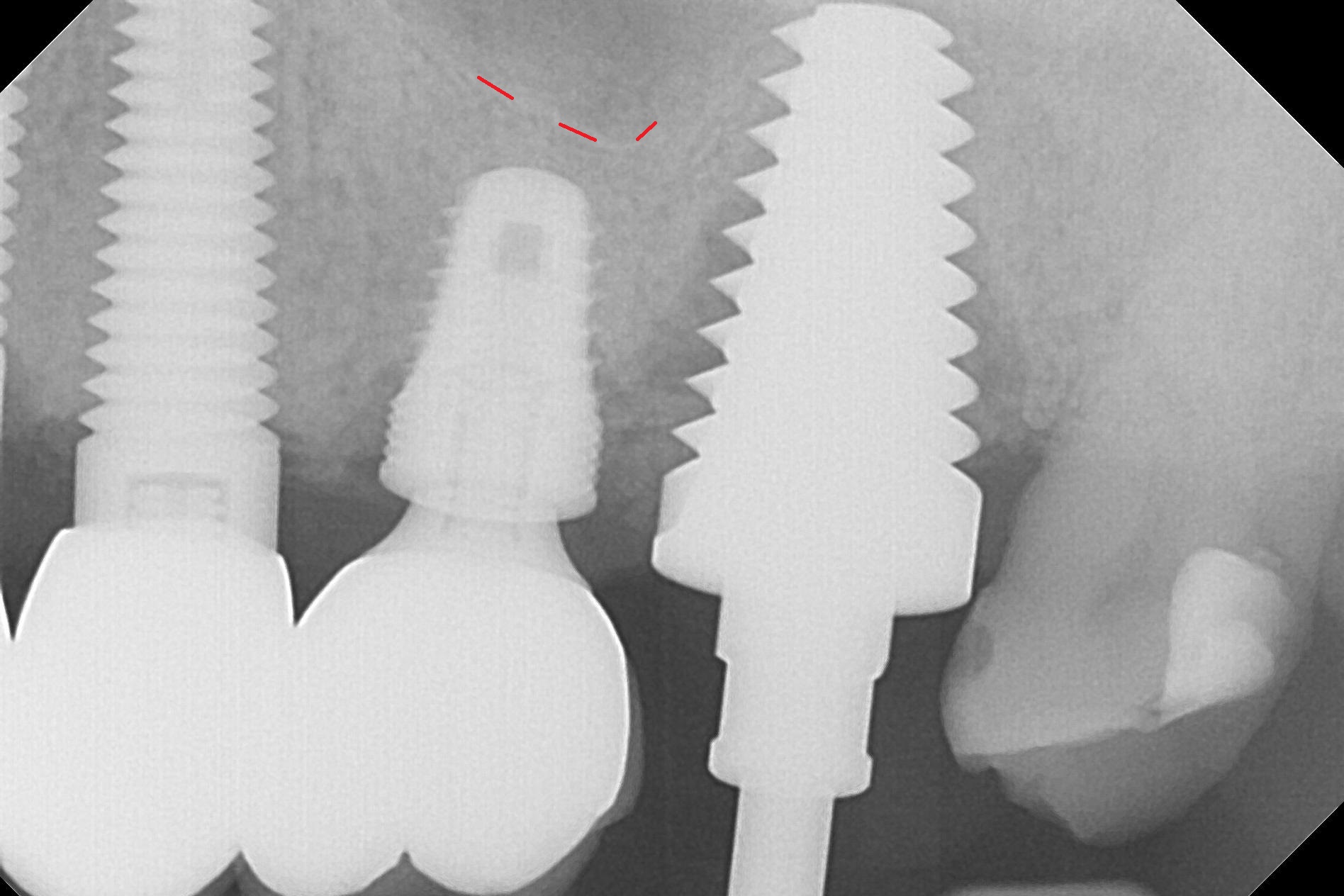
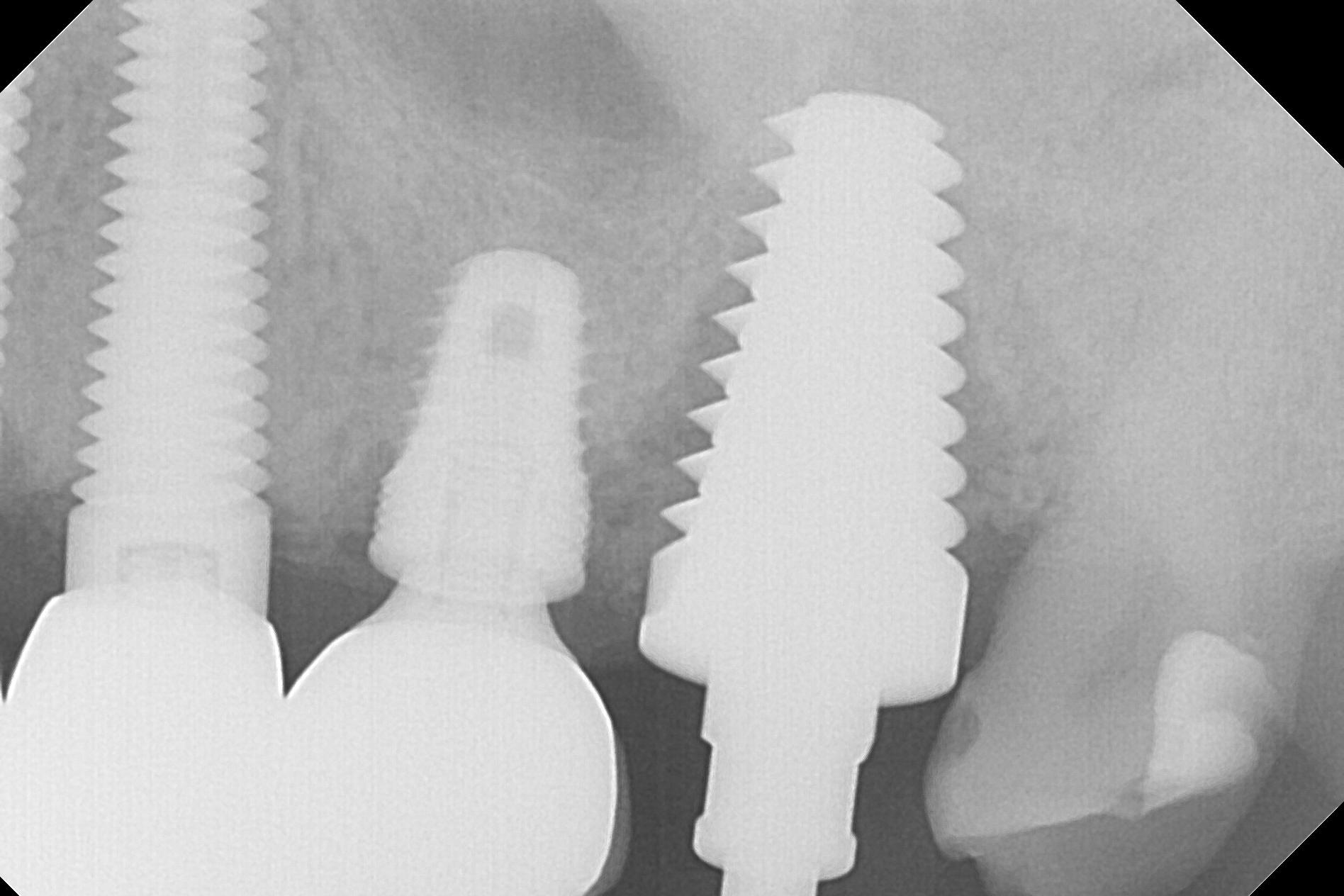
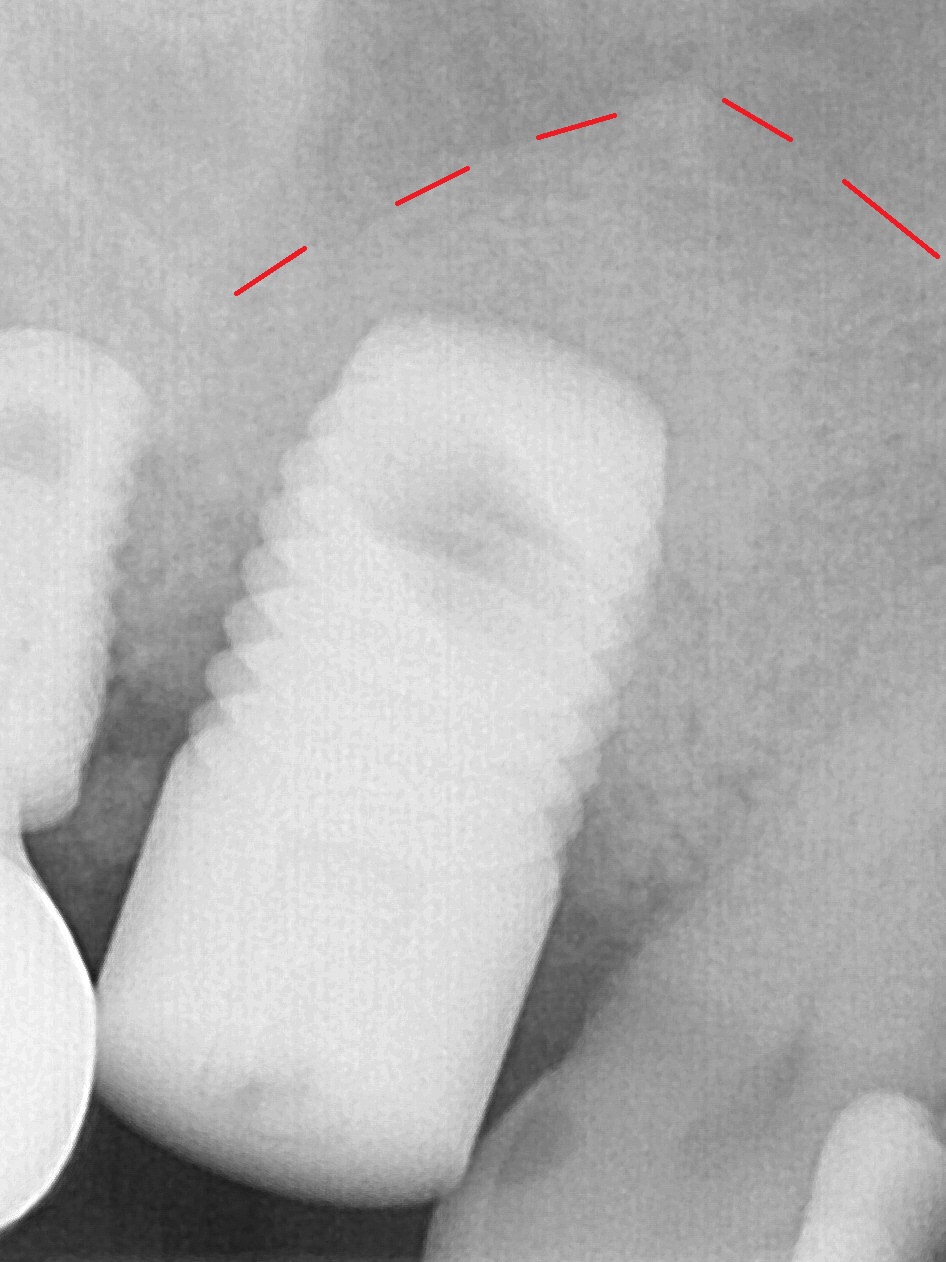
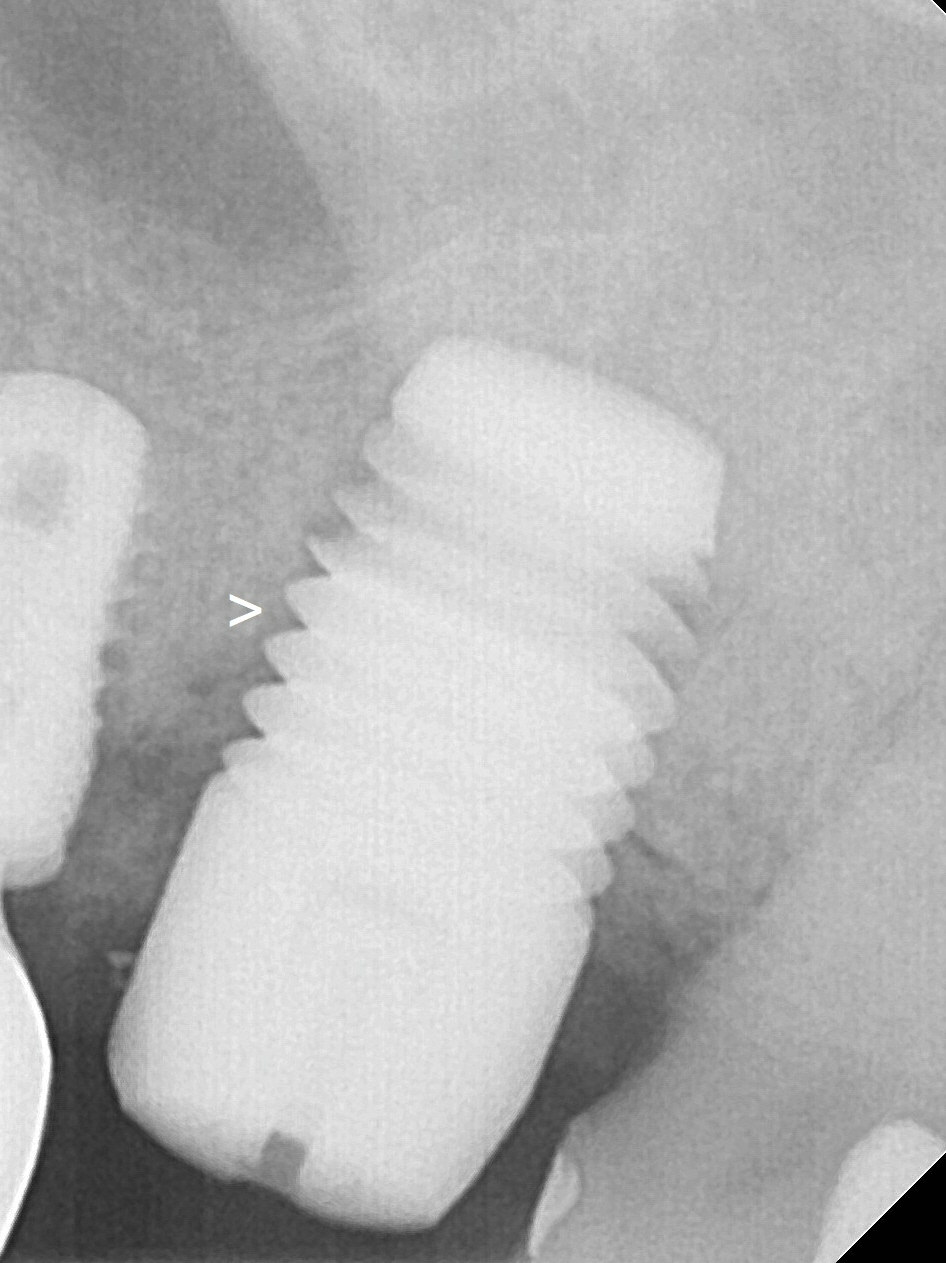
There is bone formation apical to the implant nearly 5 months postop (Fig.7, 7'). After placement of a 5x3 mm abutment and prep, a provisional is fabricated with placement of a separator between #15 and 16 to distalize the latter. Two months later, the provisional dislodges and the implant is found to be mobile. The abutment is removed; the implant is retorqued under local anesthesia until 30 Ncm. The implant becomes stable with gap (Fig.8 >). When a 6x3 mm abutment is retightened 2 months later (8.5 months postop), the patient feels pain. Impression is taken (Fig.9,10). Permanent cementation should be postponed. In fact the implant is found to be loose ~ 1 year post cementation.
Return to
Upper
Molar Immediate Implant, IBS,
Lower
2nd
Molar Large Implant
Xin Wei, DDS, PhD, MS 1st edition 02/27/2017, last revision 04/13/2019