

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
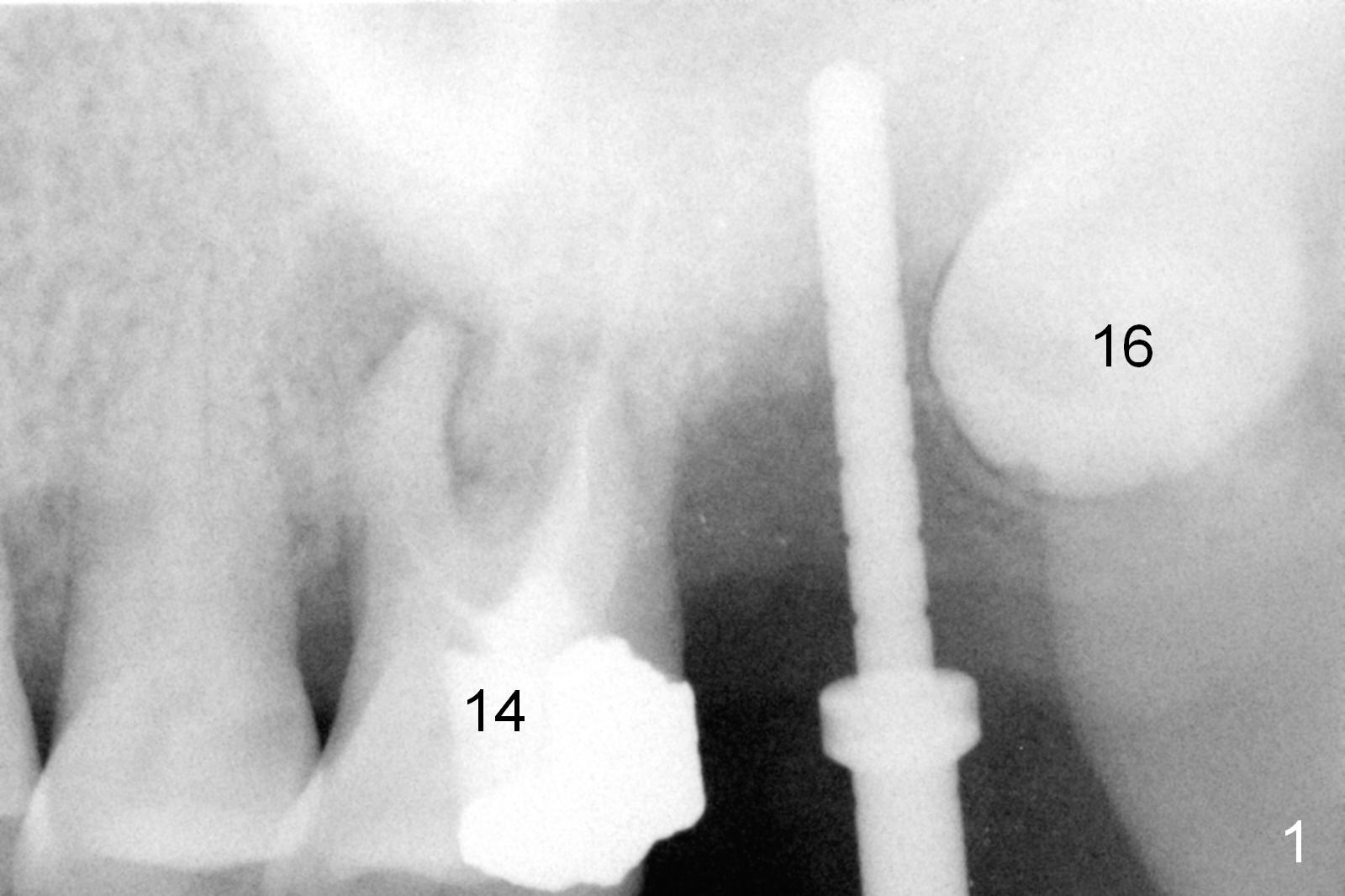
PA Angulation in Upper 2nd Implant Placement
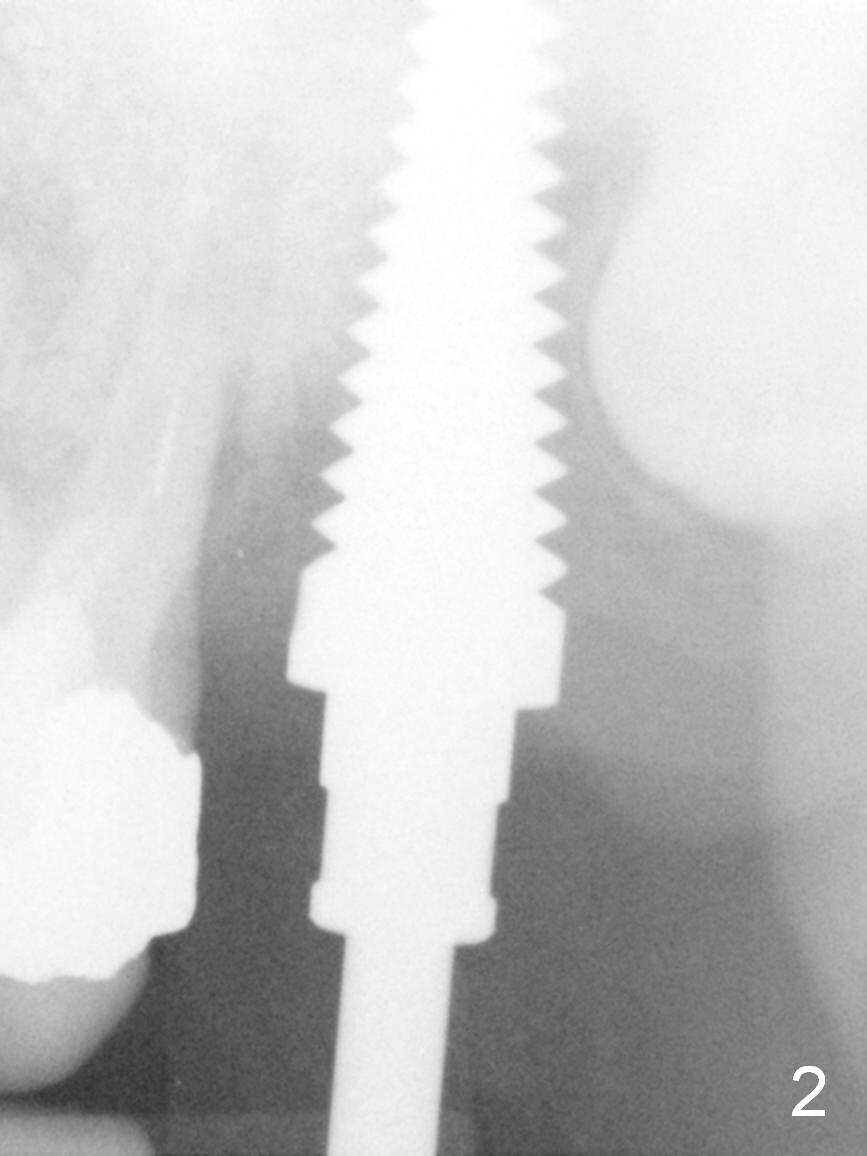
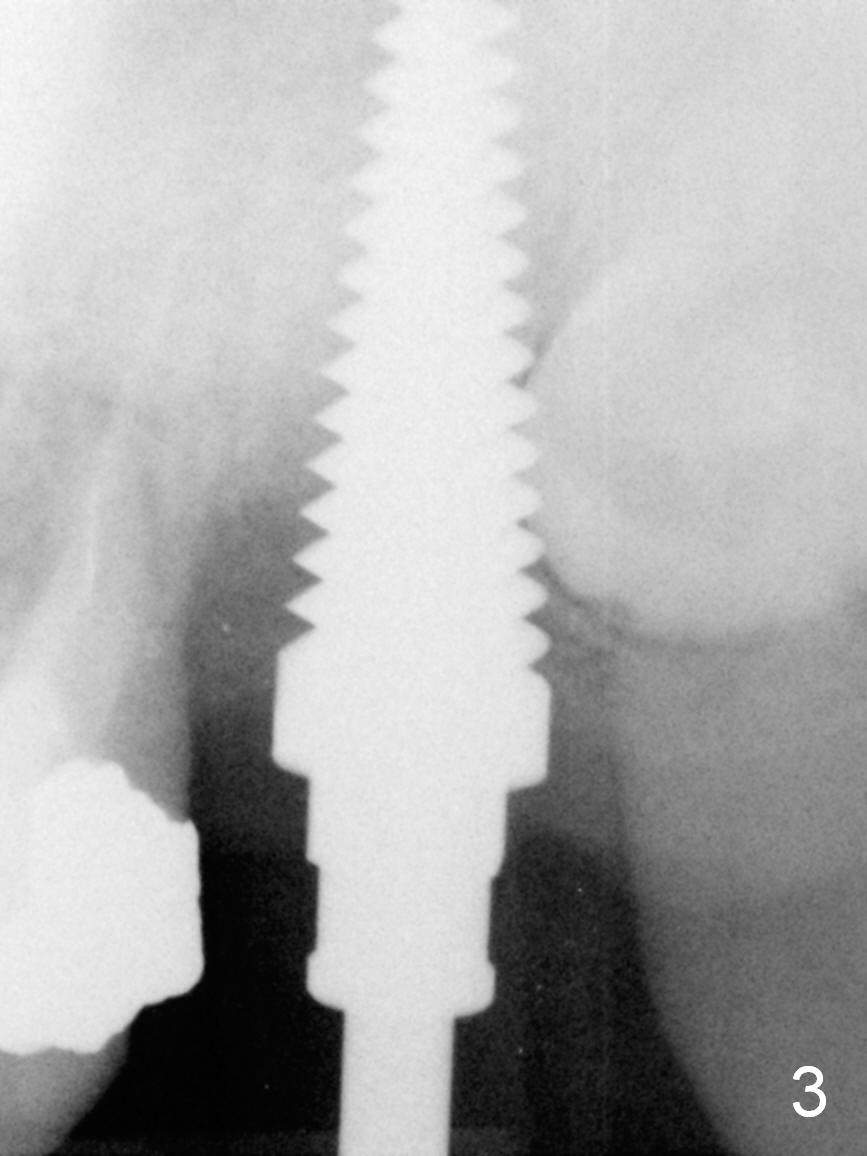
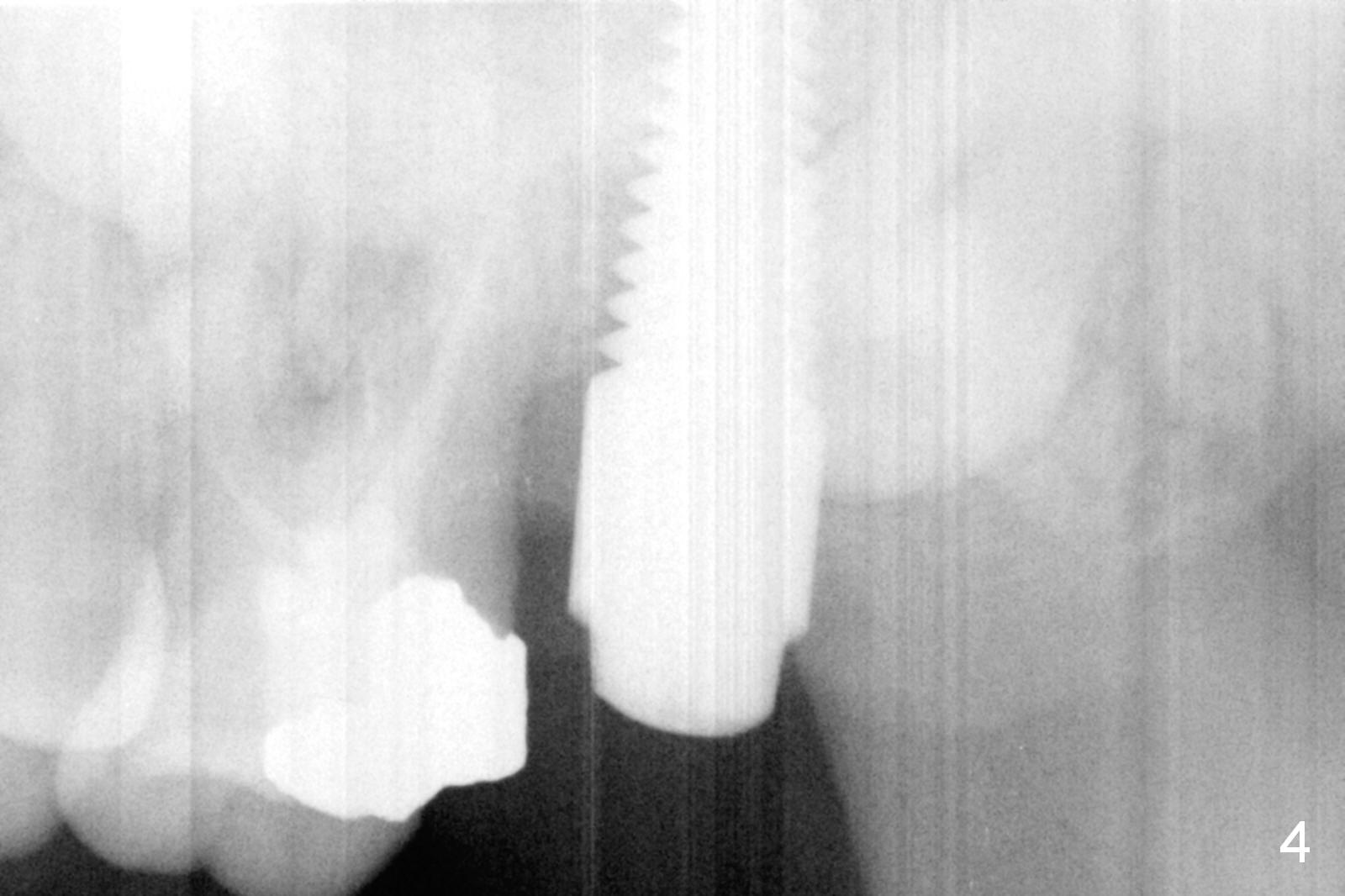
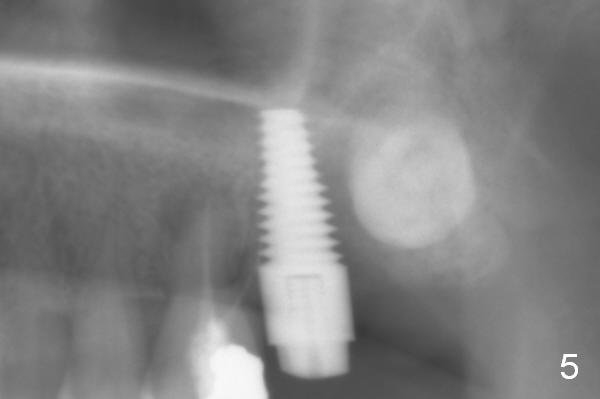
As planned osteotomy is established in the mesial slope of the 2nd molar socket, a fair distance from the 3rd molar, but PA does not show so (Fig.1). The PA does not show the apical end of long osteotomy (Fig.2,3 tap). When a 6x17 mm implant is placed, a PA does not show the implant apex (Fig.4), but panoramic X-ray does (Fig.5). In fact the implant is placed between the 1st and 3rd molars. When PA presents angulation issue, take panoramic X-ray.
In spite of the fact that the implant is apparently superior to the sinus floor, there is no air leakage prior to implant placement. The 3rd molar is not extracted to avoid trauma. It appears to be in the bucco- or linguo-version. The 1st molar is asymptomatic.
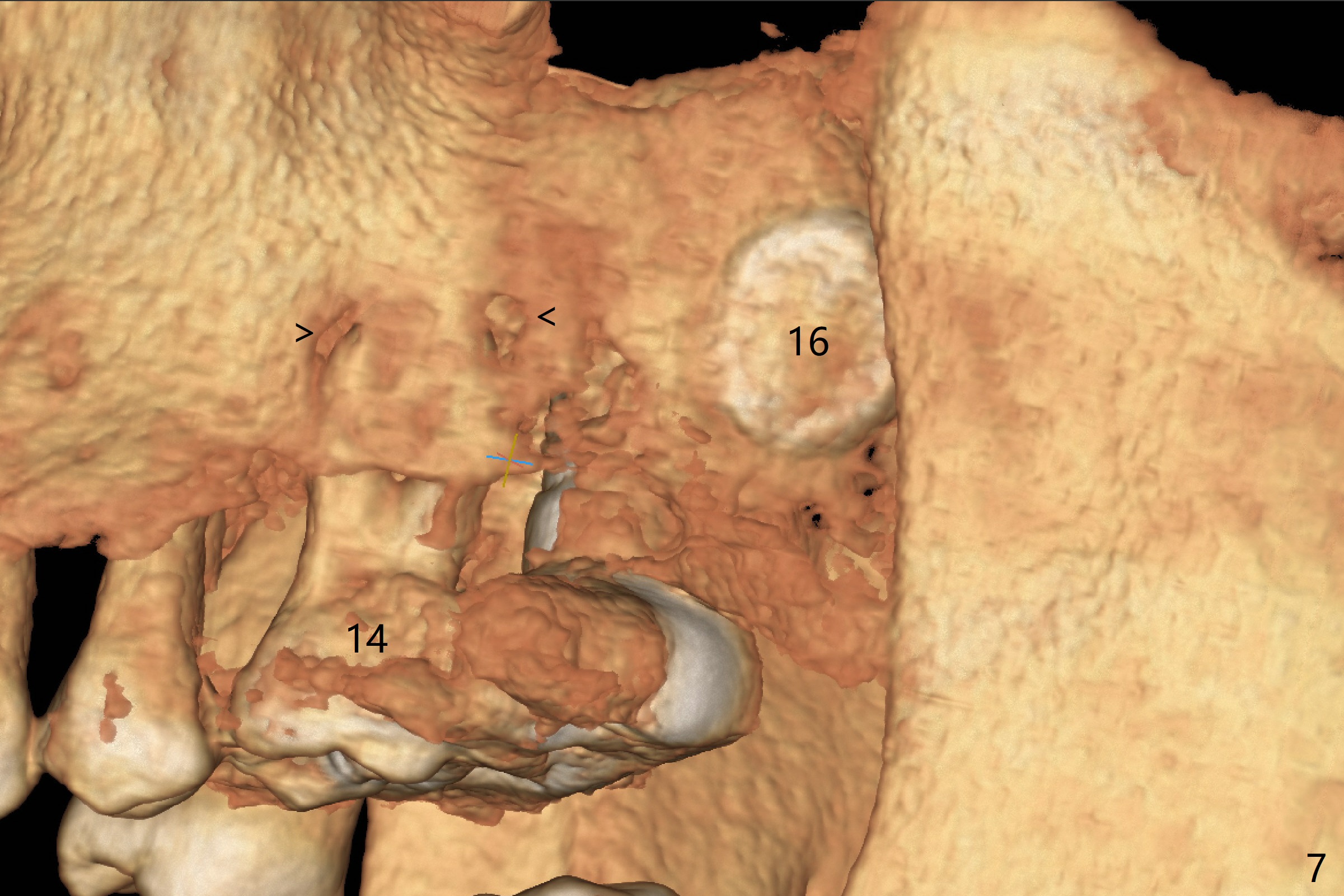
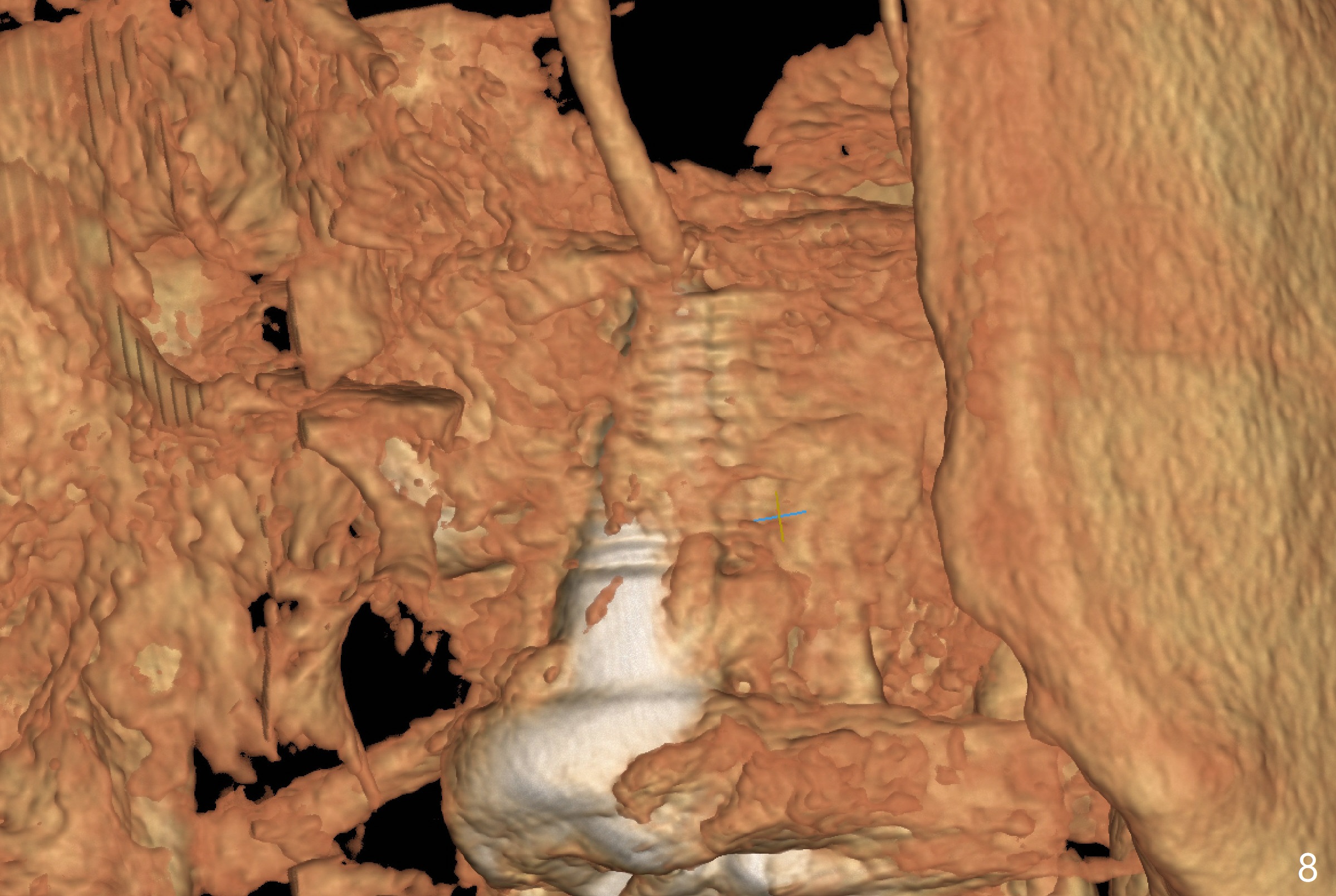
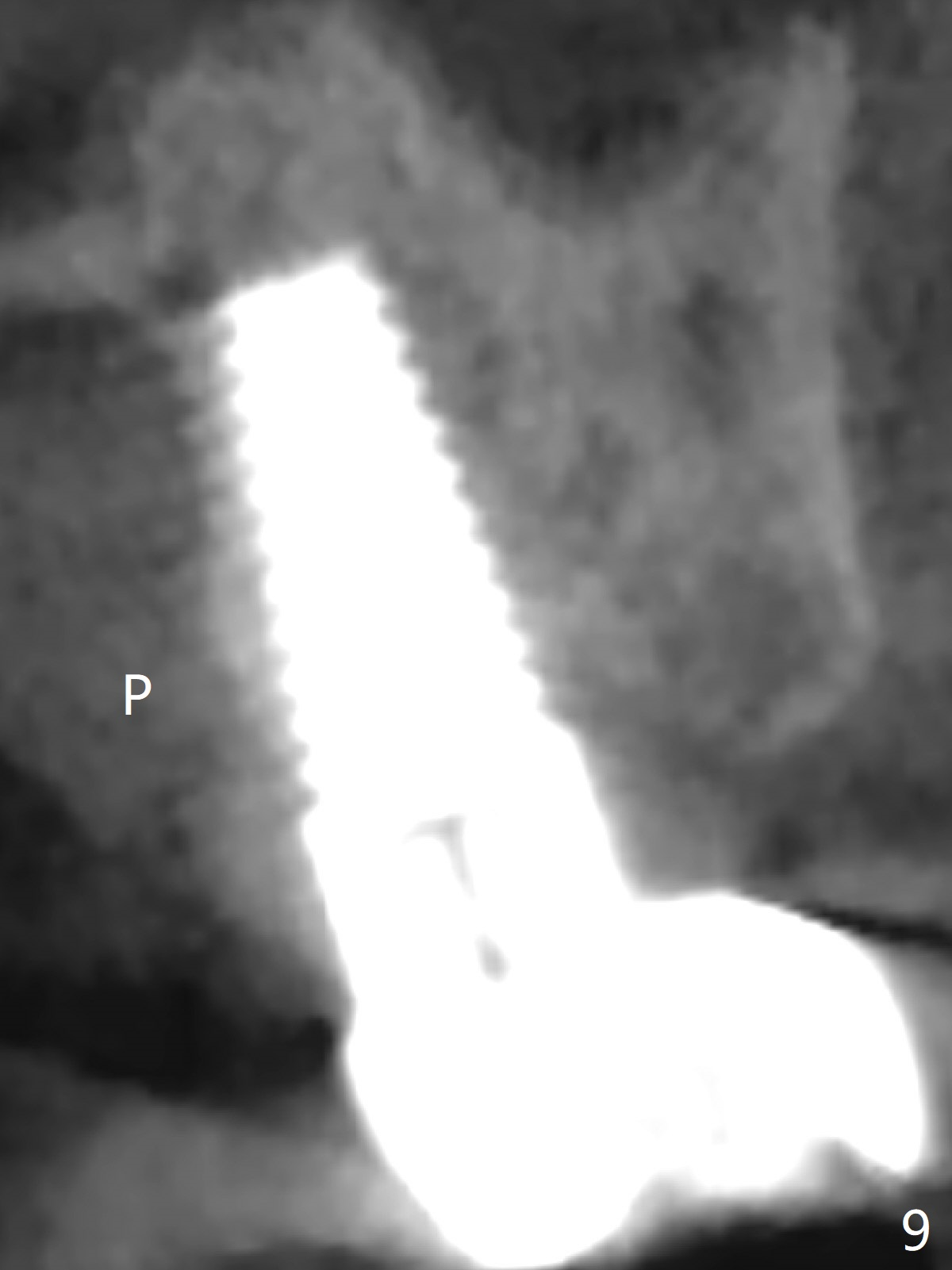
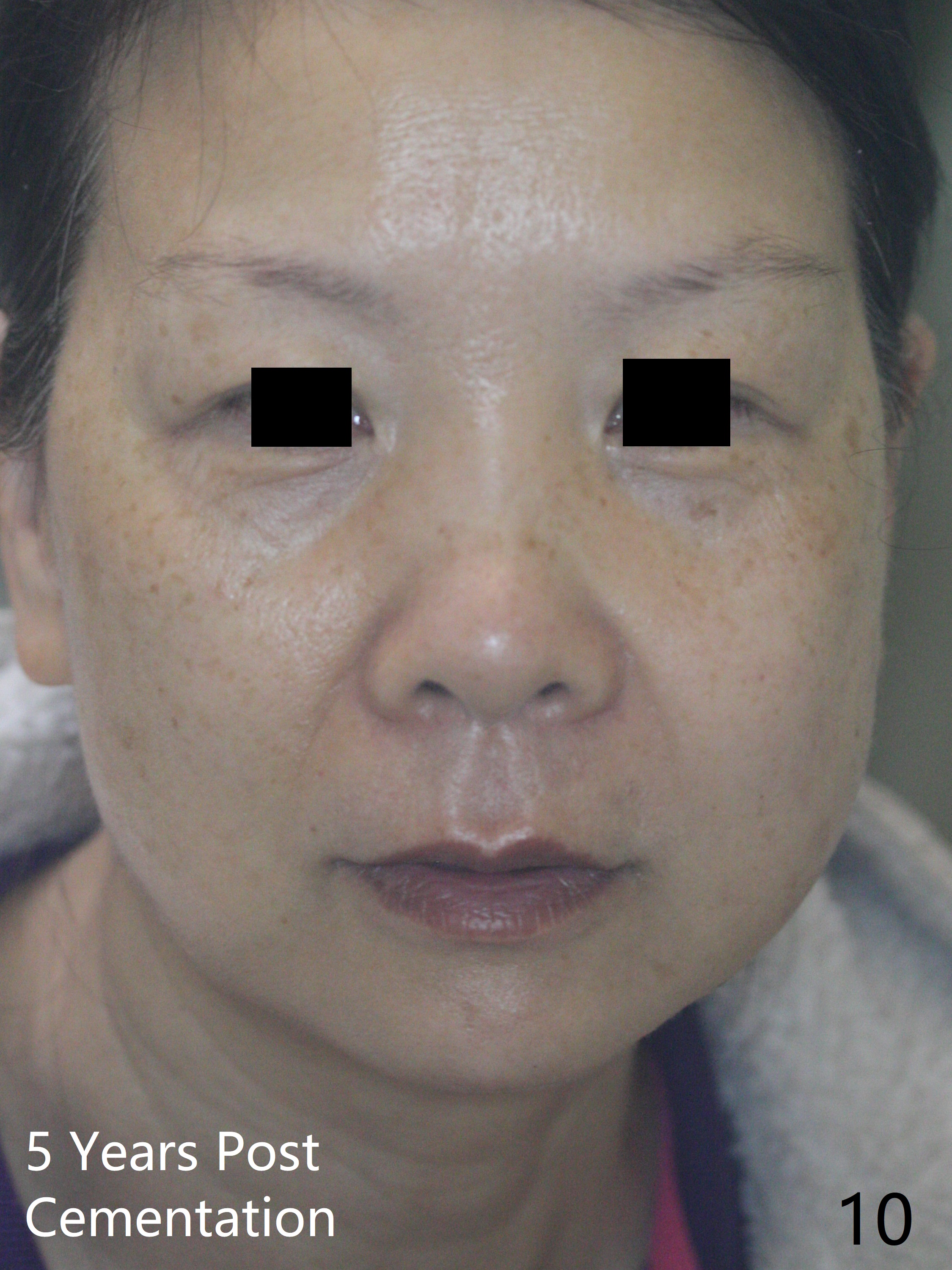
The patient returns 3 months postop because of dislodgement of the immediate provisional. It appears that the implant has osteointegrated, although there is bone loss in the coronal half of the 1st thread (Fig.6 *). Impression is taken for the definitive restoration. The fearful patient asks whether we can place 2 implants in the upper right quadrant! The implant is functioning 2 years post cementation in spite of the presence of the two pathologies (buccal apical bony defects at #14 (Fig.7 arrowheads) and impacted 3rd molar (#16)). However, the implant was placed palatally (Fig.8 (3 D palatal view), 9 (coronal section)). Finally the patient develops left facial cellulitis 5 years post cementation (Fig.10), probably related to apical periodontitis of the MB root of #14 (Fig.11 *).
Return to Upper Molar Immediate Implant #2,3 最常见并发症 Screw Xin Wei, DDS, PhD, MS 1st edition 11/12/2015, last revision 02/23/2021