


|
|
|
|
|
|
|
|
|
|
|
|
|
||
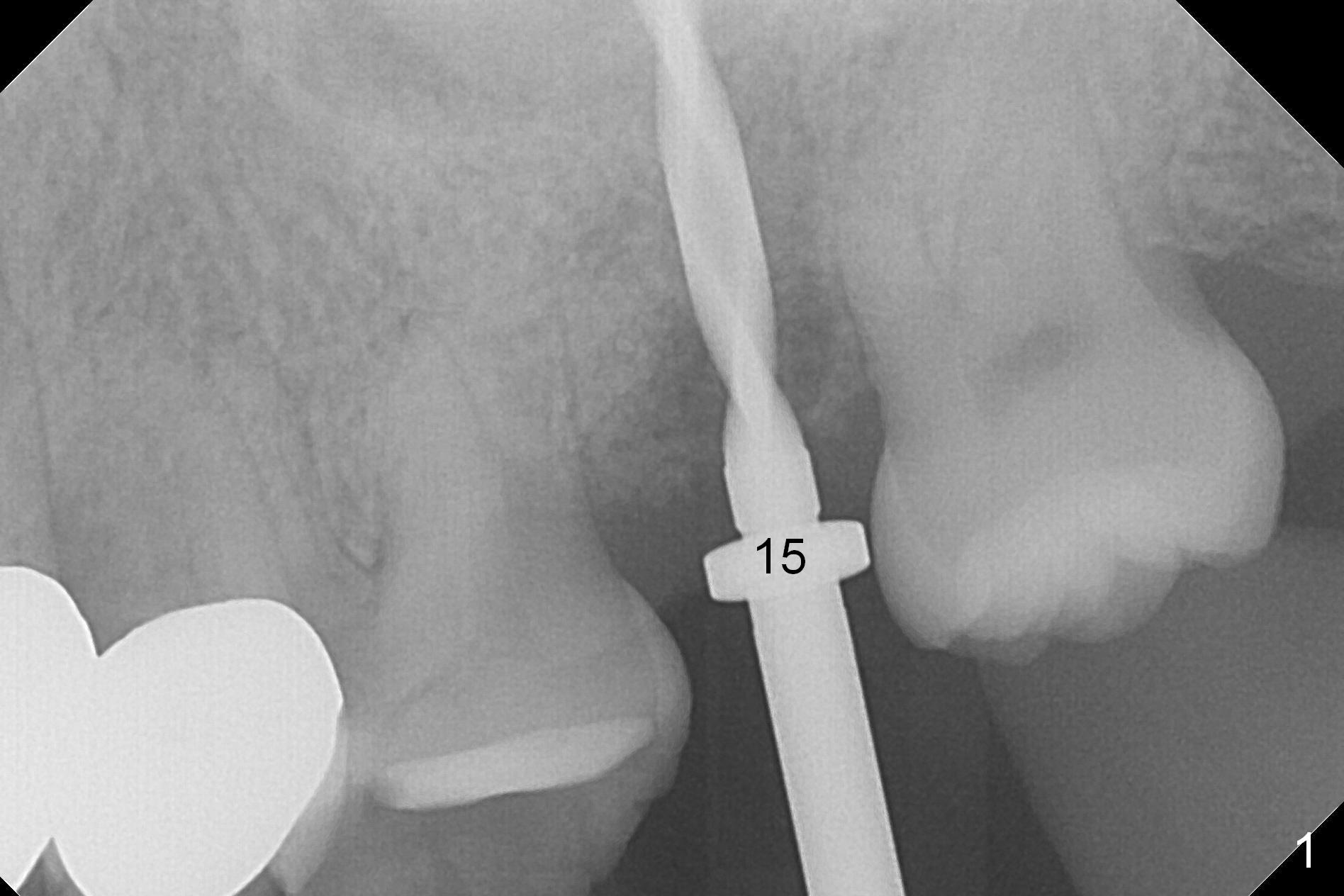
Implant Placed Deep
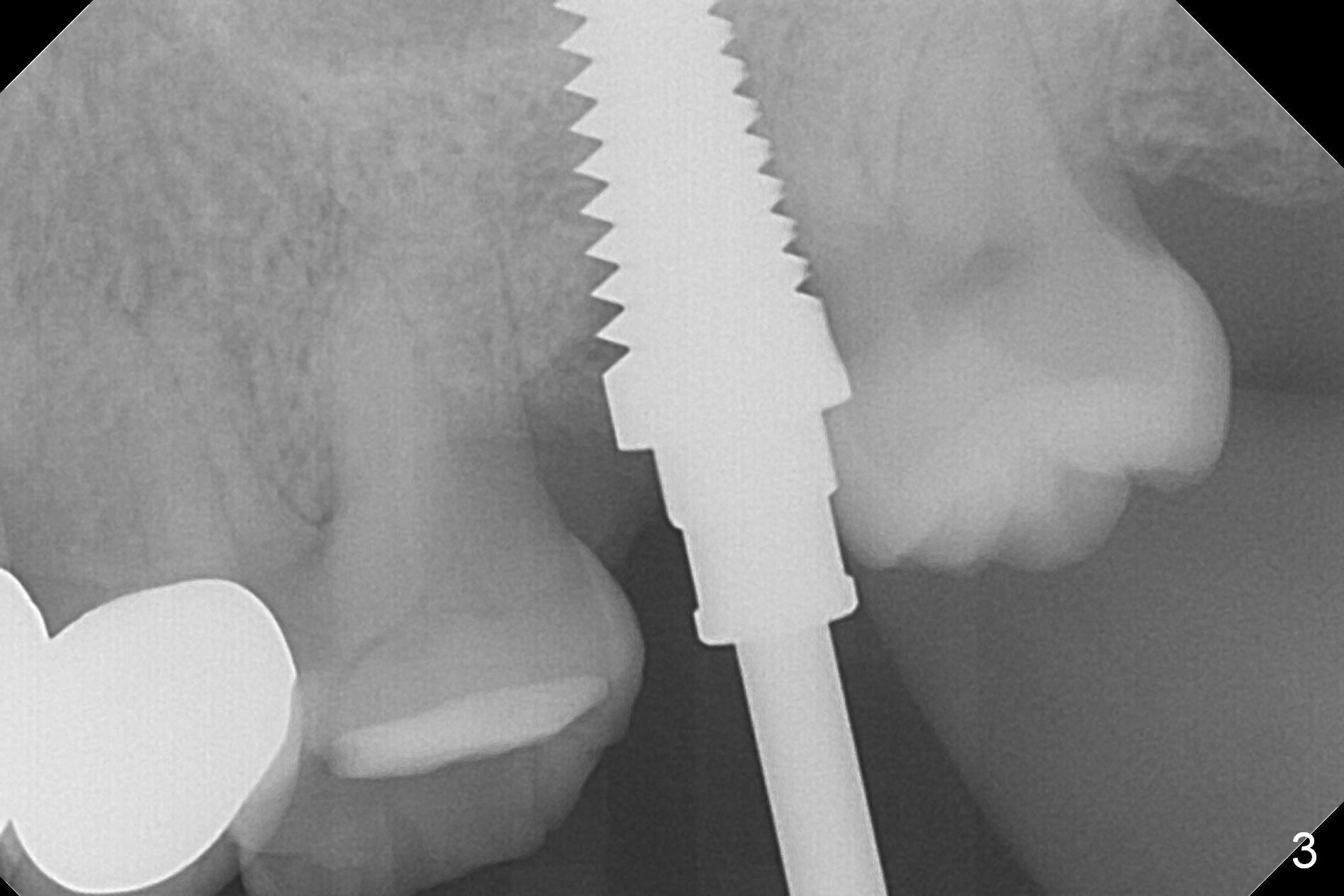
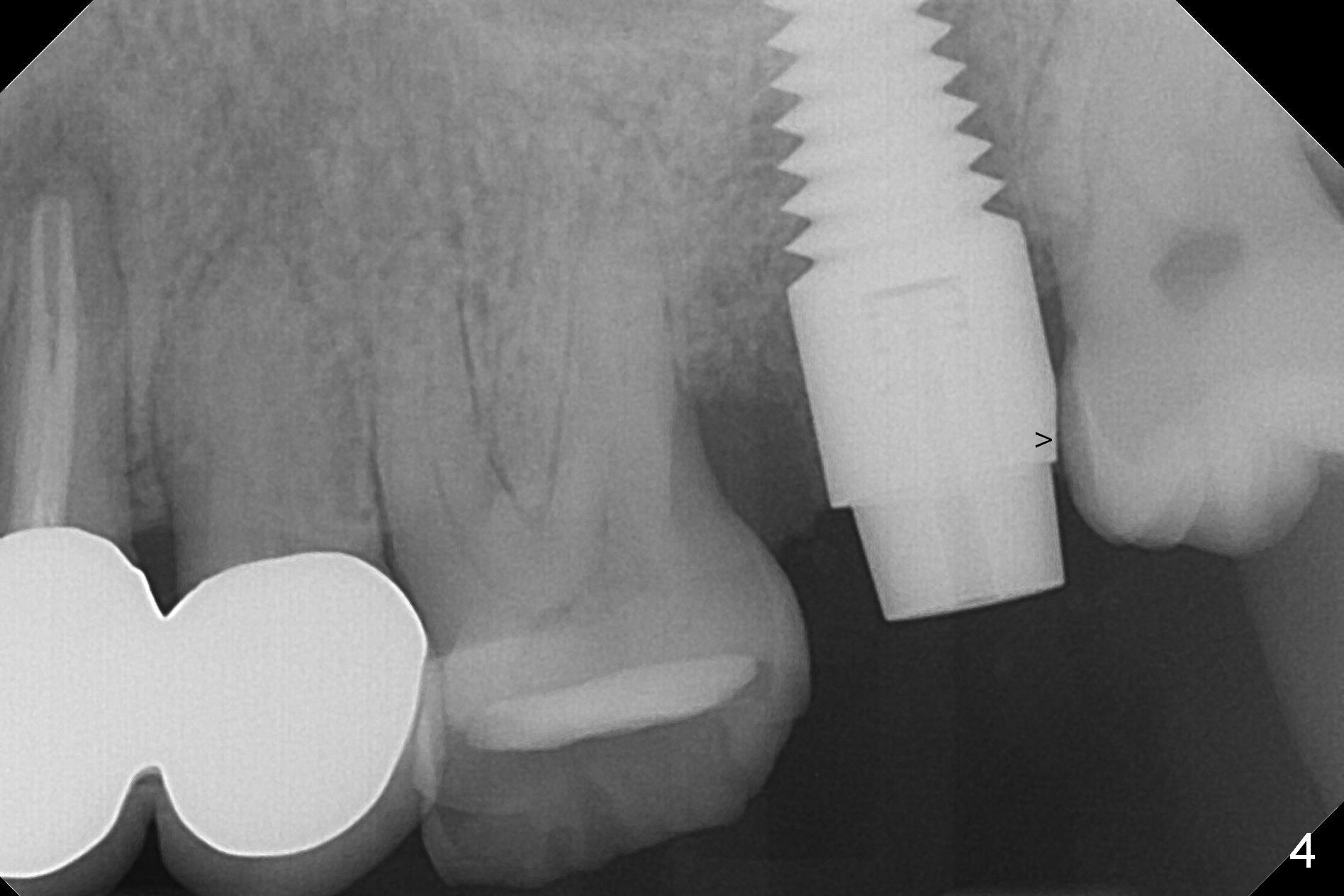
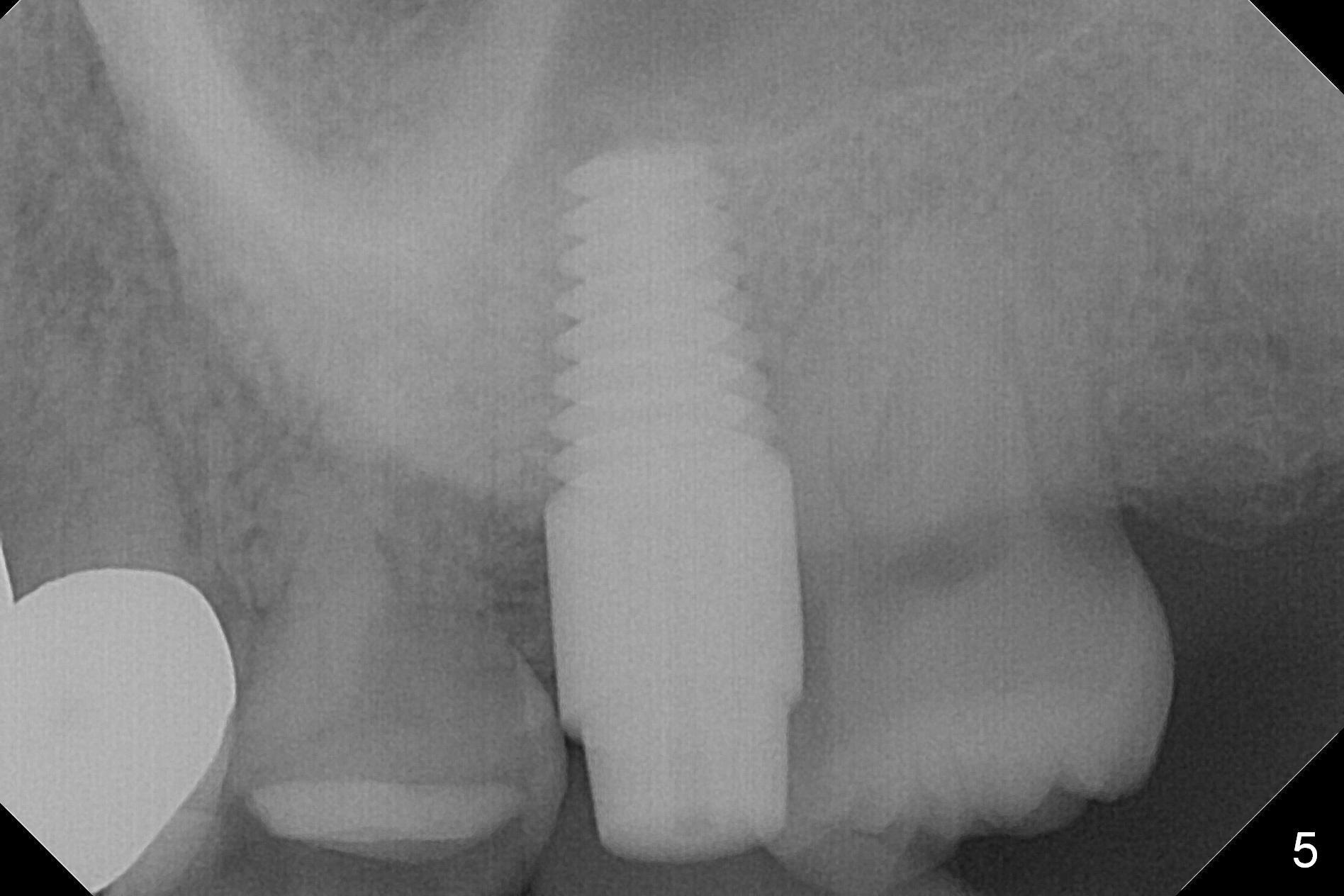
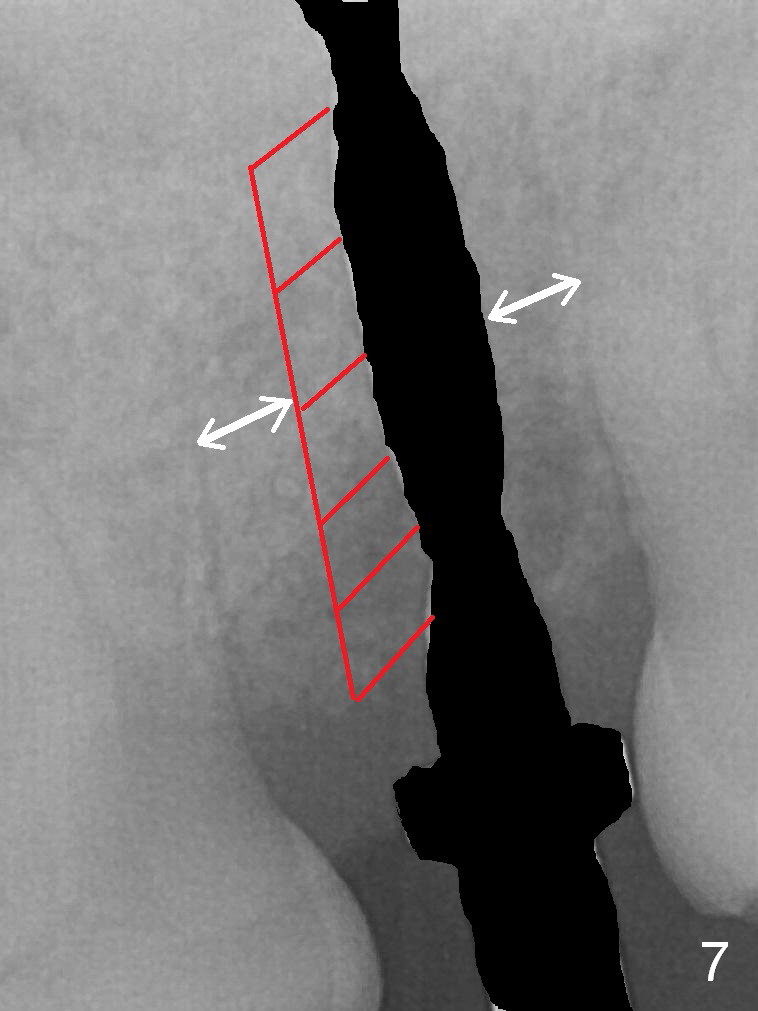
As expected, the implant at #15 is removed with ease. There is no granulation tissue. After applying Metronidazole gauze, osteotomy is initiated in the palatomesial wall of the site (Fig.1 with sinus membrane perforation). Without careful observation, the osteotomy increases until 5 mm UF tap drill is inserted without much stability; in fact the osteotomy remains distal (Fig.2). To increase stability, a 6x17 mm Tatum tap is placed for 14 mm (Fig.3). A 6x14 mm implant is placed with insertion torque less than 40 Ncm, followed by 5x3 mm abutment (Fig.4). The distal margin of the implant has to be trimmed to get clearance from the tooth #16. Before implant placement, a piece of collagen plug is placed in the apical portion of the osteotomy to repair the sinus membrane perforation (Fig.5). After implant placement, there is ~ .5 mm buccal gap, which is filled with allograft and Osteogen. To correct the trajectory, Lindamann bur should be used immediately post removal of the 2 mm drill (Fig.6, as compared to Fig.1). Substantial mesial bone should be removed (Fig.7 red slashes) so that the thickness of the mesial and distal bone is equivalent (white arrows).
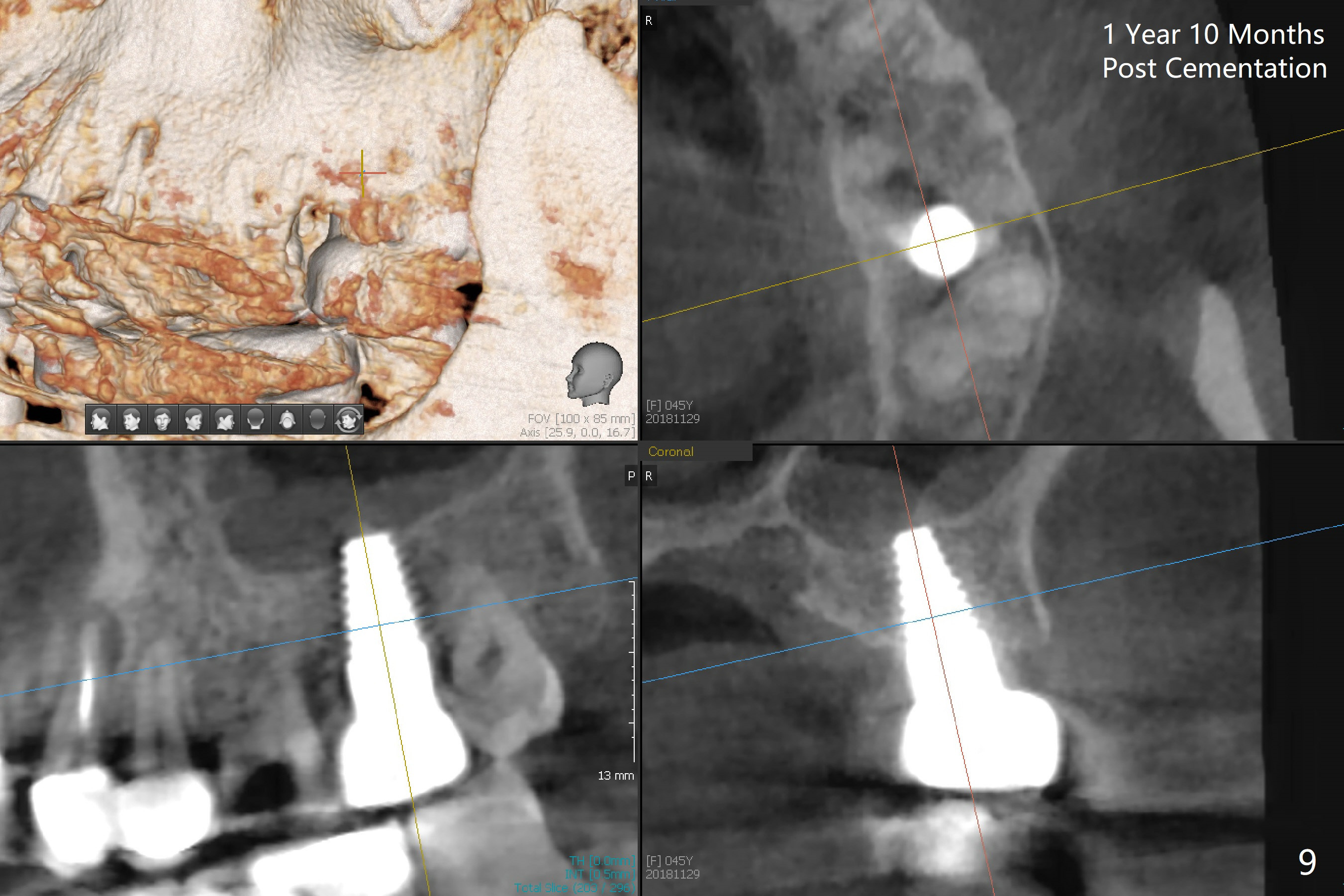
The patient returns for final restoration 7 months postop (Fig.8). The clearance between #15 and 16 is minimal. To increase the clearance, acrylic is added to the distal surface of a provisional at #15 so that the tooth #16 will be distalized. It appears that the implant is positioned within normal limit after limited ortho (Fig.9).
Return to Upper Molar Immediate Implant, IBS, #3,10 Xin Wei, DDS, PhD, MS 1st edition 02/13/2017, last revision 12/02/2018