

|
|
|
|
|
|
Compensation for Osteotomy Deviation
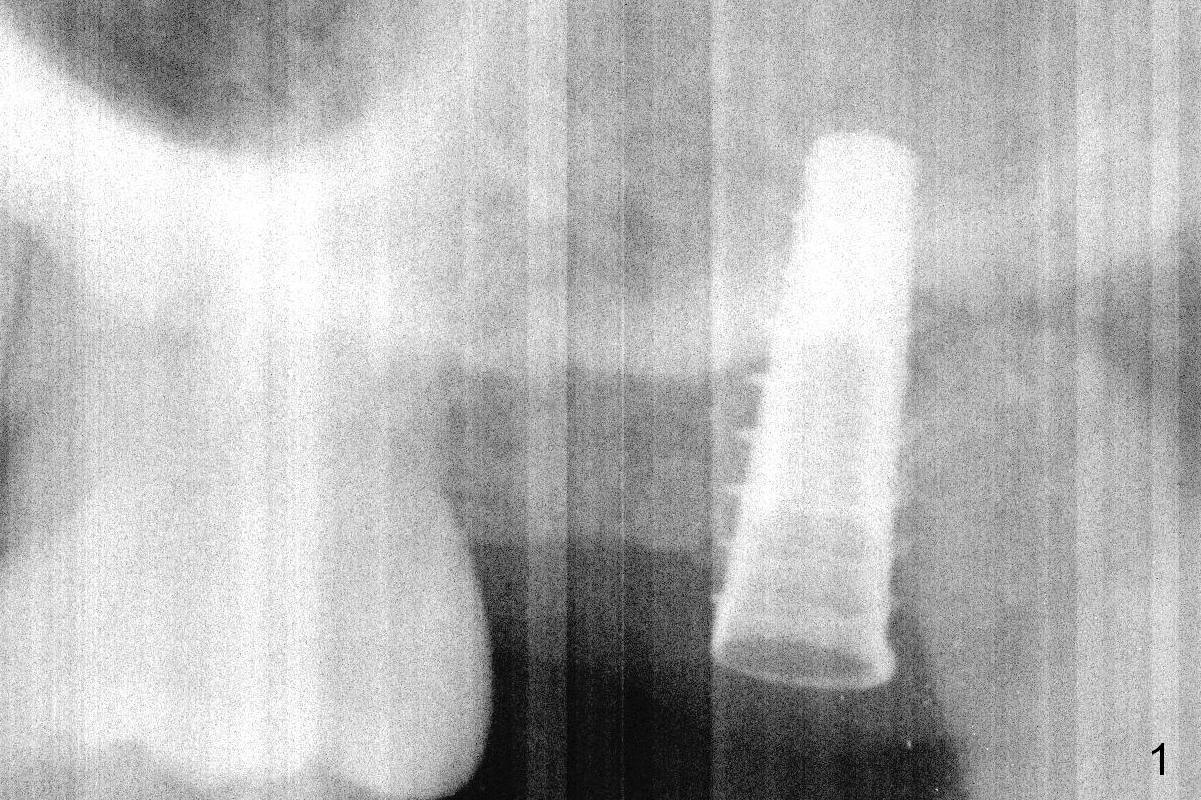
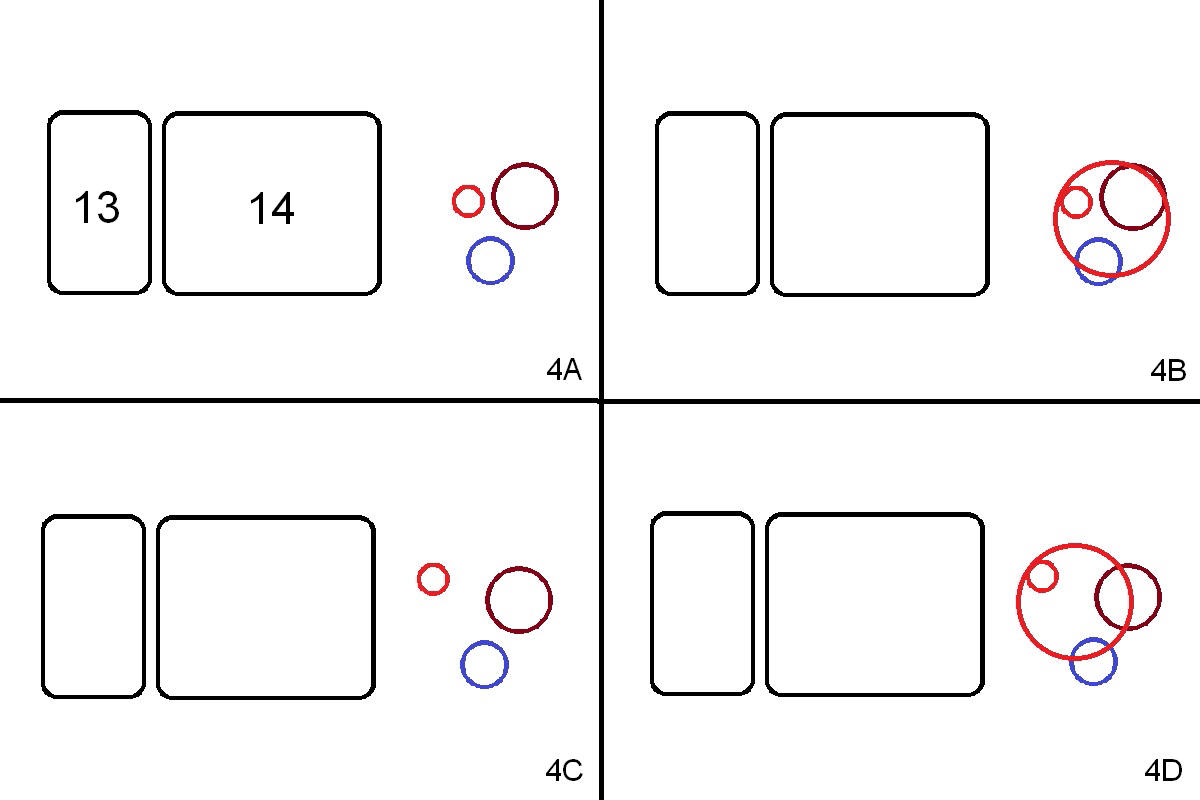
Initial osteotomy at the site of #15 for 4x11 mm dummy implant is created by #15 blade, Magic Split and Magic Expanders (ME) 3.0 and 3.8 mm (flapless, Fig.1,2, 4A (blue circle)). The implant is palatally displaced. Release incision confirms the deviation. A new osteotomy is established with 1.6 mm pilot drill in the middle of the site (Fig.4A (occlusal view) red circle). Distal to the new osteotomy is the incompletely healed socket (brown circle). As the osteotomy is enlarged by ME until 4.3 mm and placement of 4.5 and 5.0 mm dummy implant and of 5.5x9 mm definitive one (Fig.3, 4B large red circle), the osteotomy gradually deviates distopalatally. Introspectively, the new osteotomy should have been placed more buccomesially (Fig.4C red circle) so that the final osteotomy may end up normally (Fig.4D large red circle).
Prior to implant placement, two pieces of PRF plug are inserted. The insertion torque is <15 Ncm. A cover screw is placed. The distopalatal defect is covered by allograft and 1 piece of PRF membrane. There is no intraop sinus membrane perforation or nasal hemorrhage postop.
Because of unfavorable implant/crown ratio (Fig.3), the implant will be uncovered 6-7 months postop. An angled abutment is expected to correct the distopalatal displacement of the implant. In the meantime orthodontic treatment should start to align the malpositioned anterior teeth before extraction and implantation.
Return to
Upper
Molar Immediate Implant, IBS
Xin Wei, DDS, PhD, MS 1st edition 11/28/2016, last revision 11/28/2016