
|
|
|
|
|
|
|
|
|
|
|
|
Osteotomes for Early Implant Placement are Efficient
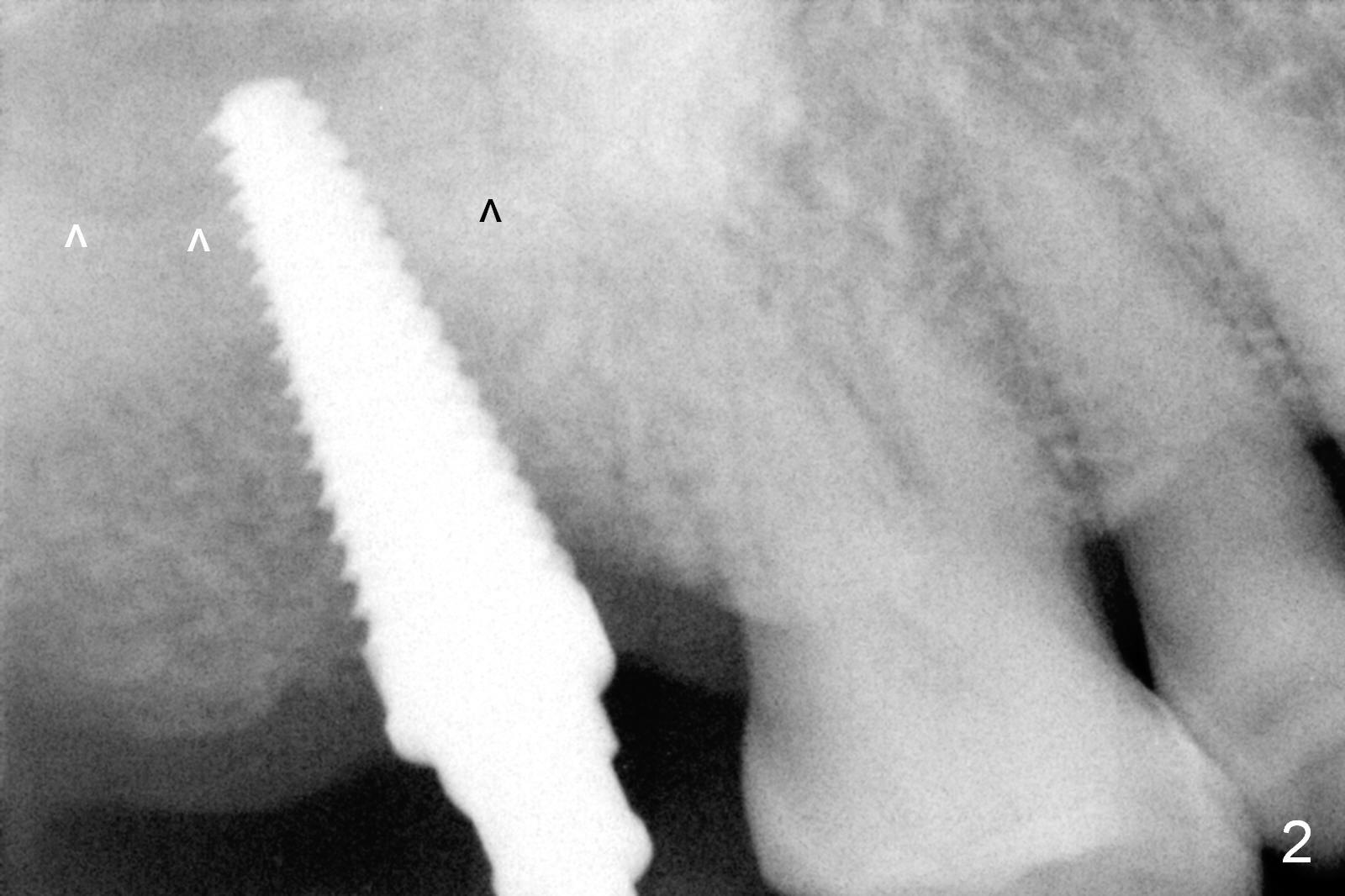
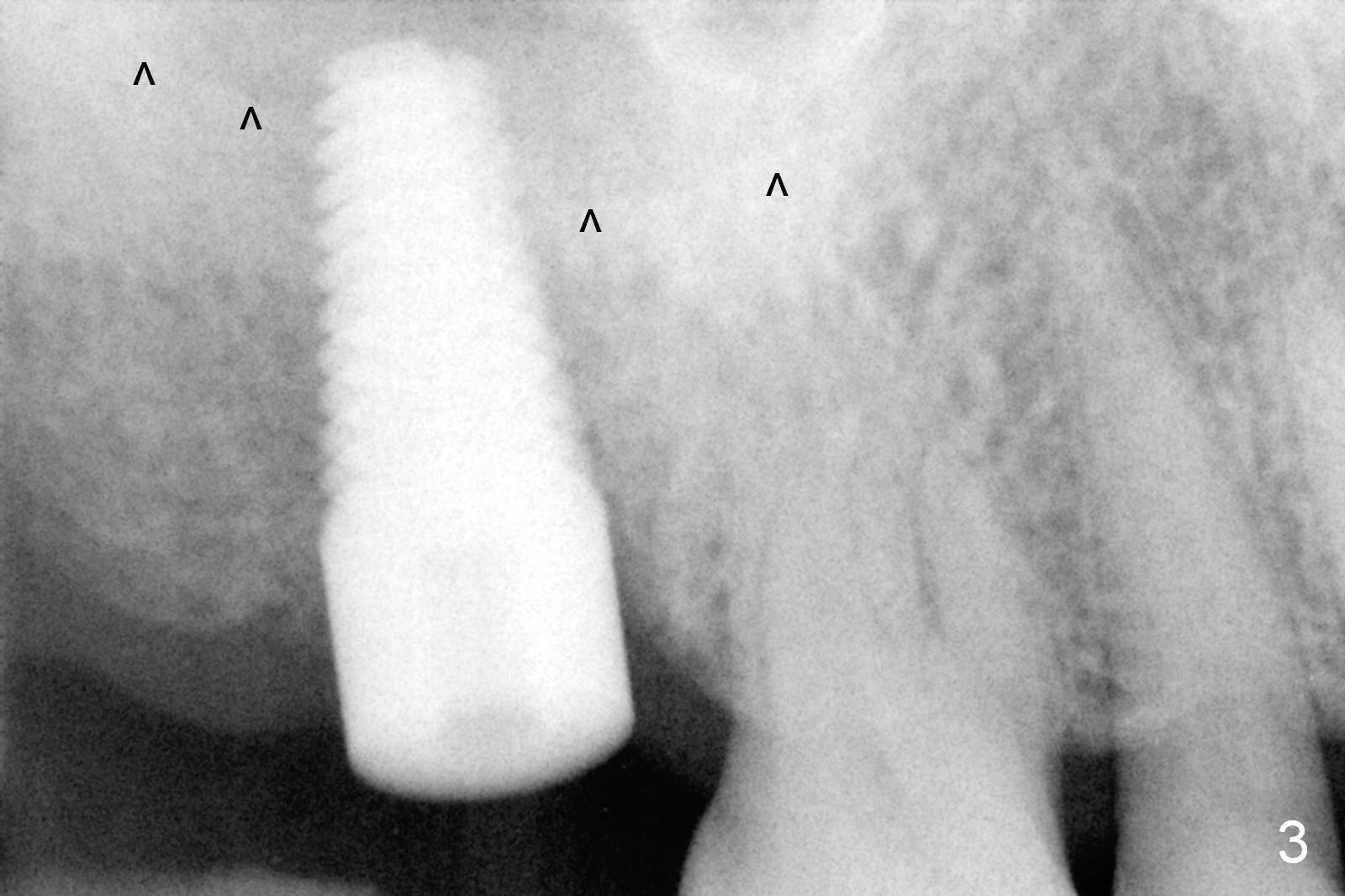
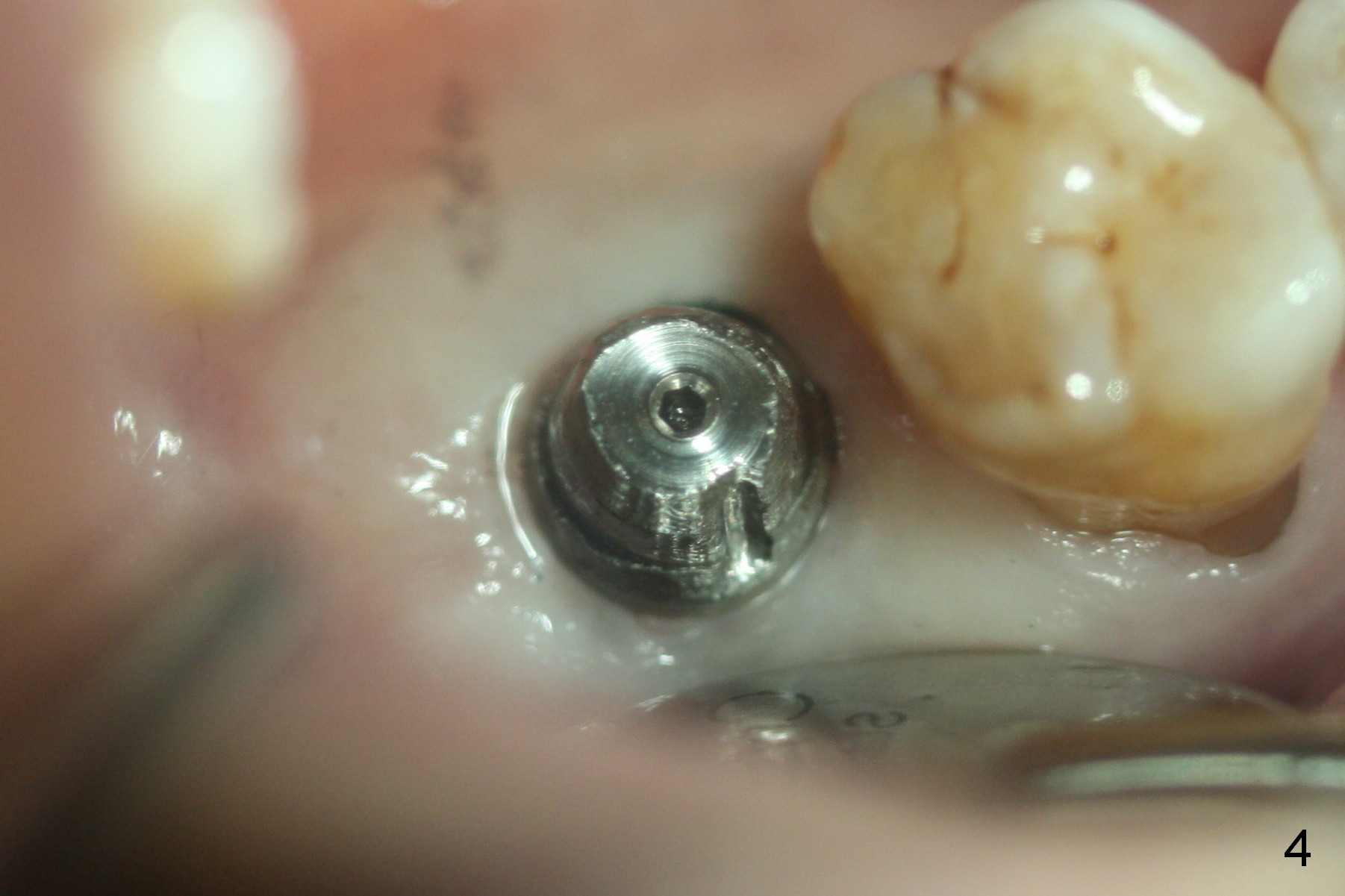
It is approximately 4 weeks post extraction when the patient returns for implant placement at the site of #15; the socket heals (Fig.1). It is easy to insert #15 blade into the socket about 10 mm, followed by 2, 3, 4 mm osteotomes at 17 mm deep. There is no air leakage for nose blowing test. A 6x20 mm tap has achieved initial stability (Fig.2; ^: sinus floor). There is no sign of sinus membrane perforation after 7x17 mm tap is removed. Insertion torque of a 7x17 mm tissue-level implant is in the neighborhood of 60 Ncm (Fig.3). It is apparent that the socket has to be obliterated to obtain primary stability, while the buccal plate is not being violated. In addition, the implant has to be as long as possible, past the sinus floor (Fig.2,3 ^) without perforation of the sinus membrane. A 5x3 mm abutment is placed immediately and prepared (Fig.4) for an immediate provisional. There is minimal hemorrhage using a small incision, osteotomes and taps.
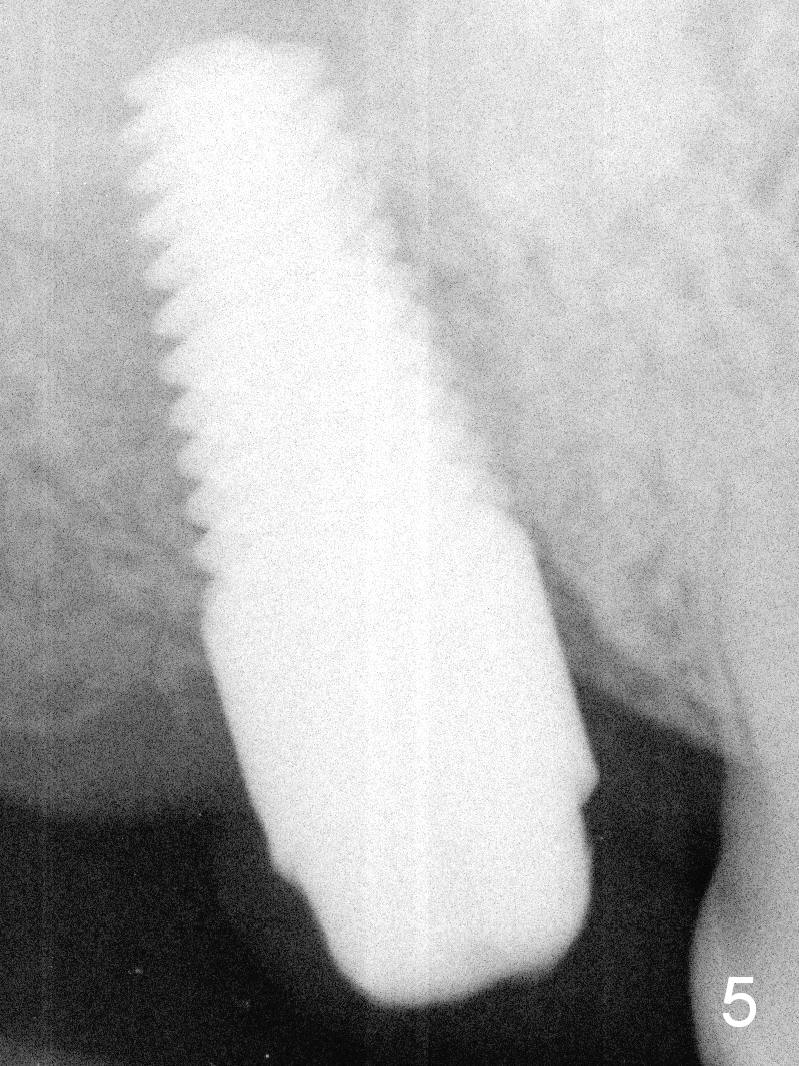
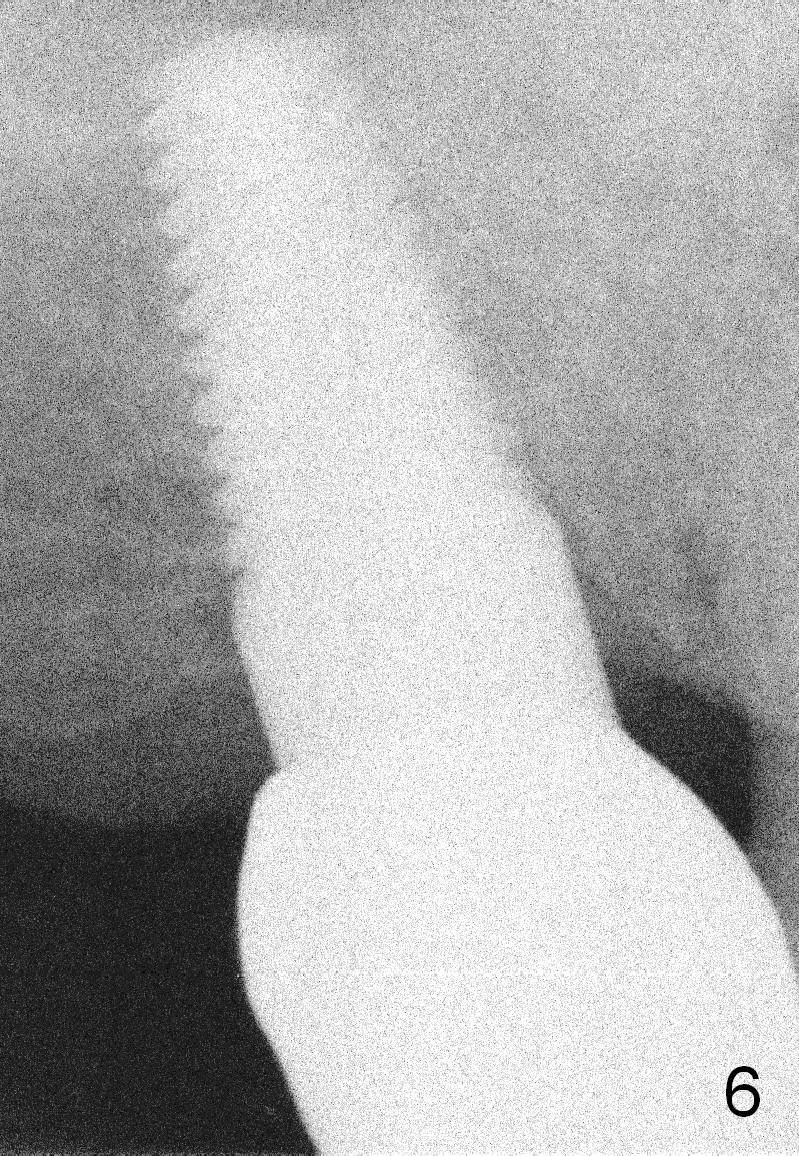
There is no complication postop. There is minimal bone loss around the implant 3 months postop (Fig.5). The patient has started to chew with the immediate provisional. The final restoration is delivered 2 weeks later. There is no bone resorption 9 months post cementation (Fig.6). The tooth #3 appears to have occlusal trauma, which is adjusted.
Return to Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 06/16/2015, last revision 07/06/2016