


|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
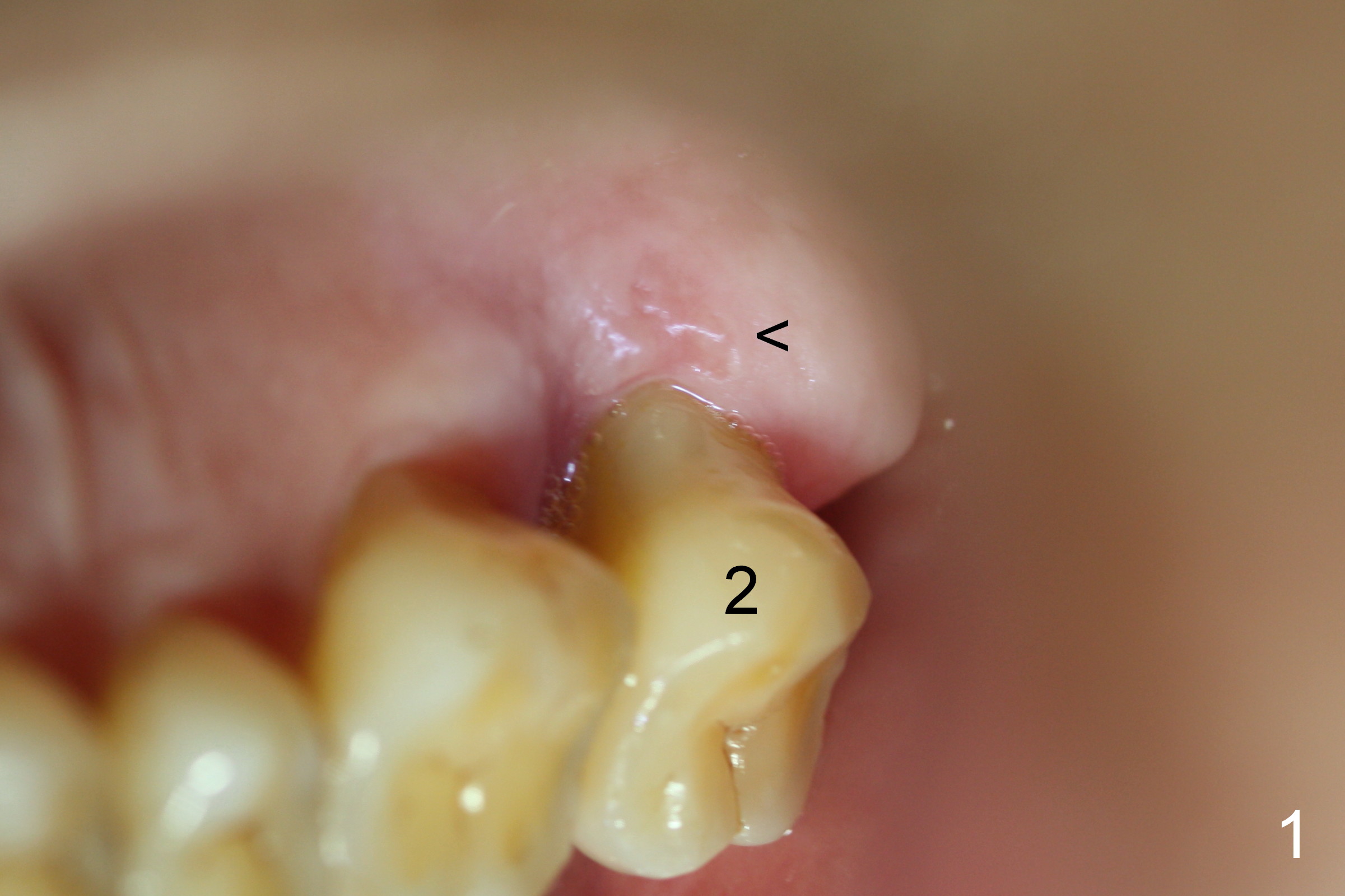
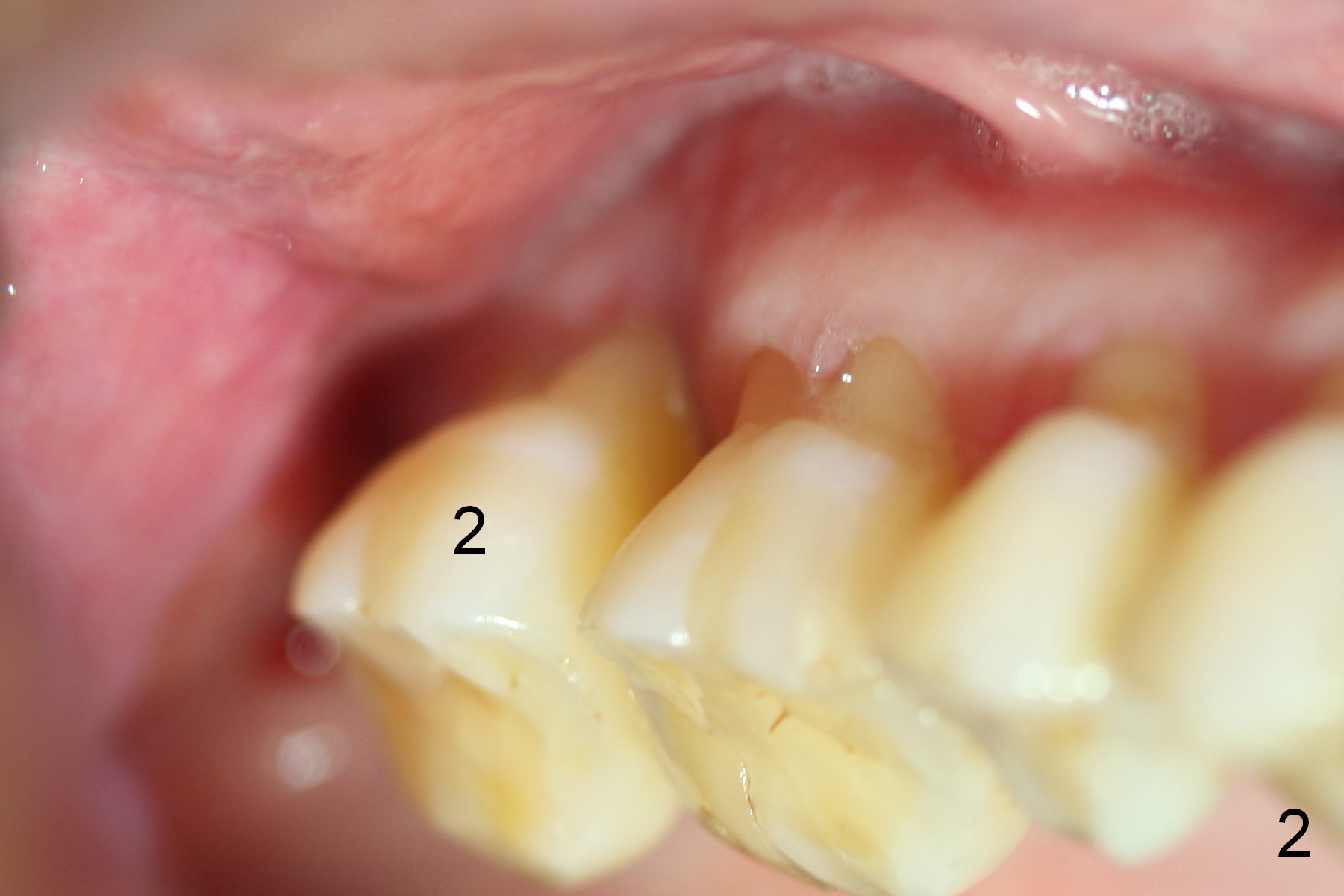
Large and Long Immediate Implant
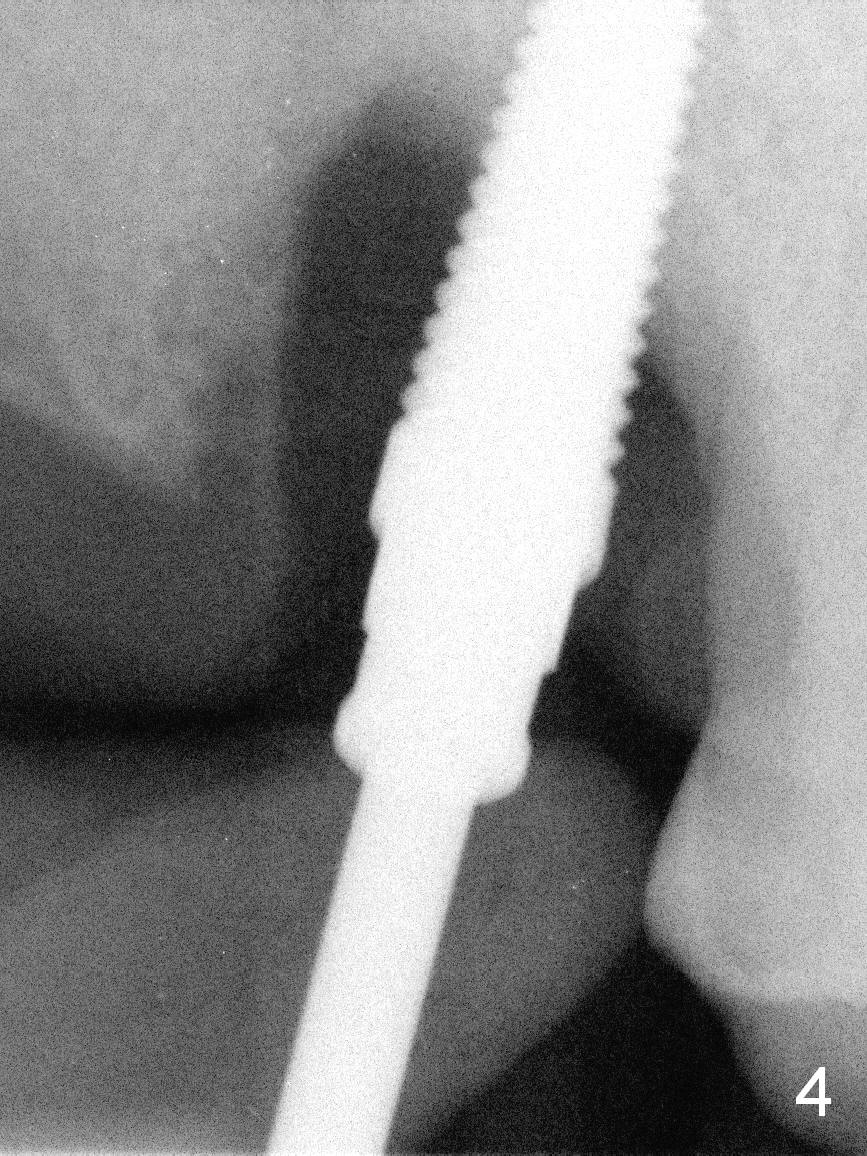
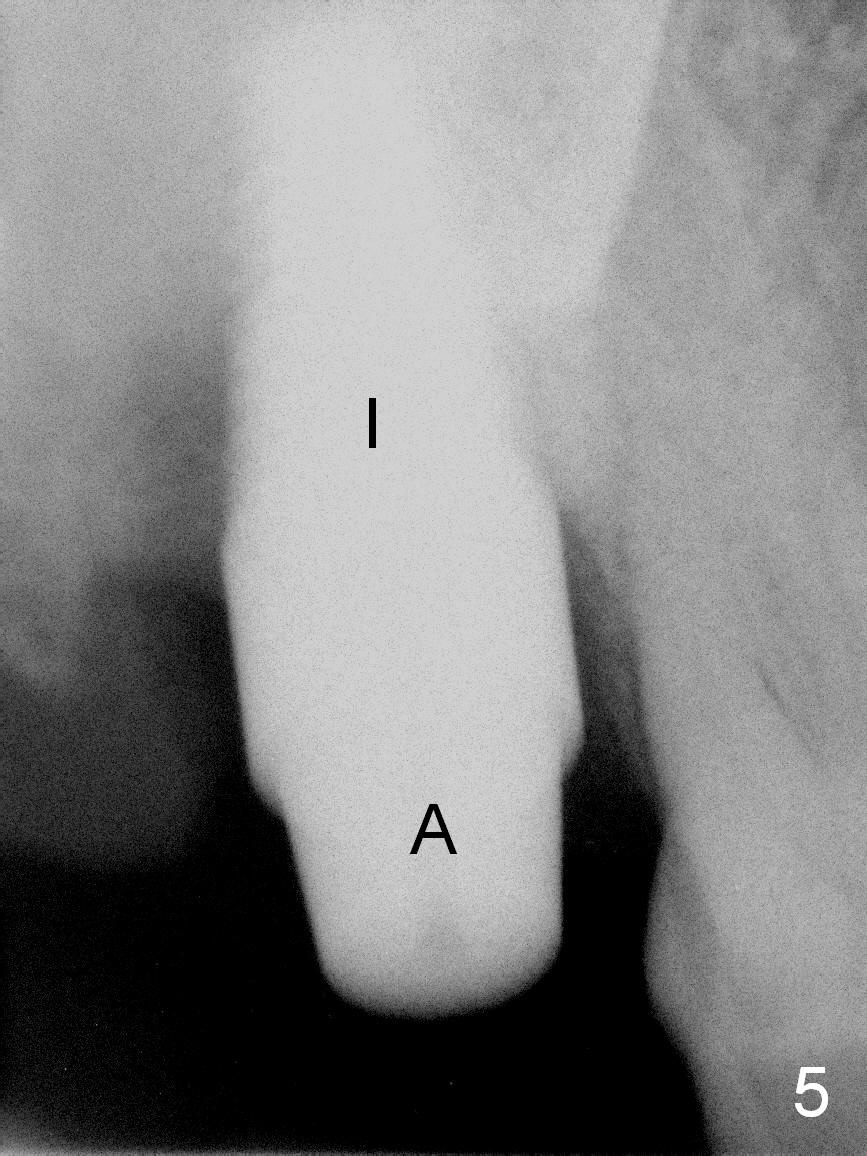
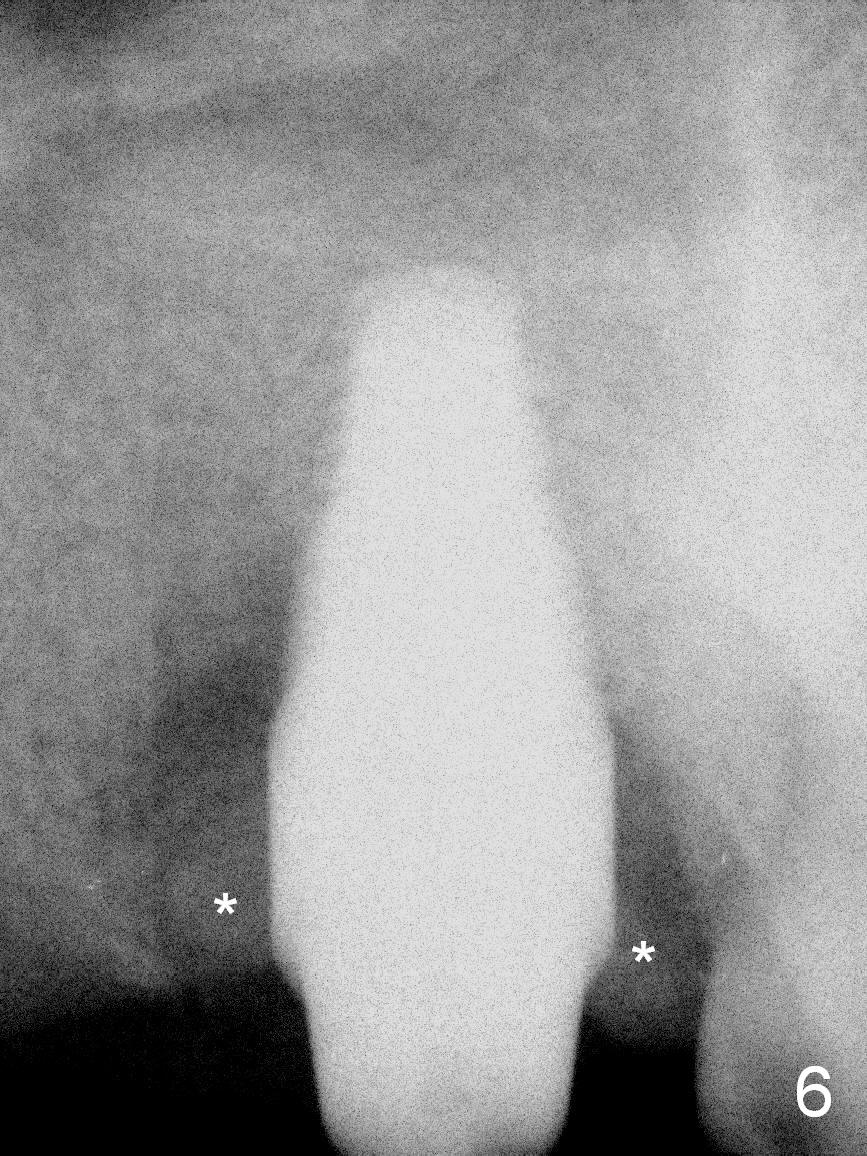
Gingival recession of the tooth #2 is severe lingually (Fig.1) and buccally (Fig.2). The mesiodistal width of the extracted tooth is 7 mm, while the buccolingual 11 mm (Fig.3). If the calculus had been removed earlier, the extraction would have been avoided or delayed. The bone apical to the socket feels like D2 bone, tested by osteotome. Osteotomy is initiated by 2 mm pilot drill, reamers and taps (Fig.4: 5x20 mm tap). After adjustment of osteotomy position with Lindamann bur, a tissue-level 7x17 mm implant is placed with insertion torque >60 Ncm (Fig.5 I); a 6x5 mm abutment is immediately placed (A). Osteogen Plug is placed in the buccal gap since it is relatively rigid, while mixture of autogenous bone, allograft and Osteogen is placed in the remaining gap, followed by Collagen Plug (Fig.6 *). An immediate provisional is fabricated and seated without cement to keep the graft in place. Since the implant is placed deeper than desired because of the buccal and lingual recession, the provisional is needed to prevent the mesial and distal gingiva from overgrowth. When the wound heals, the margin of the provisional needs to be adjusted if necessary.
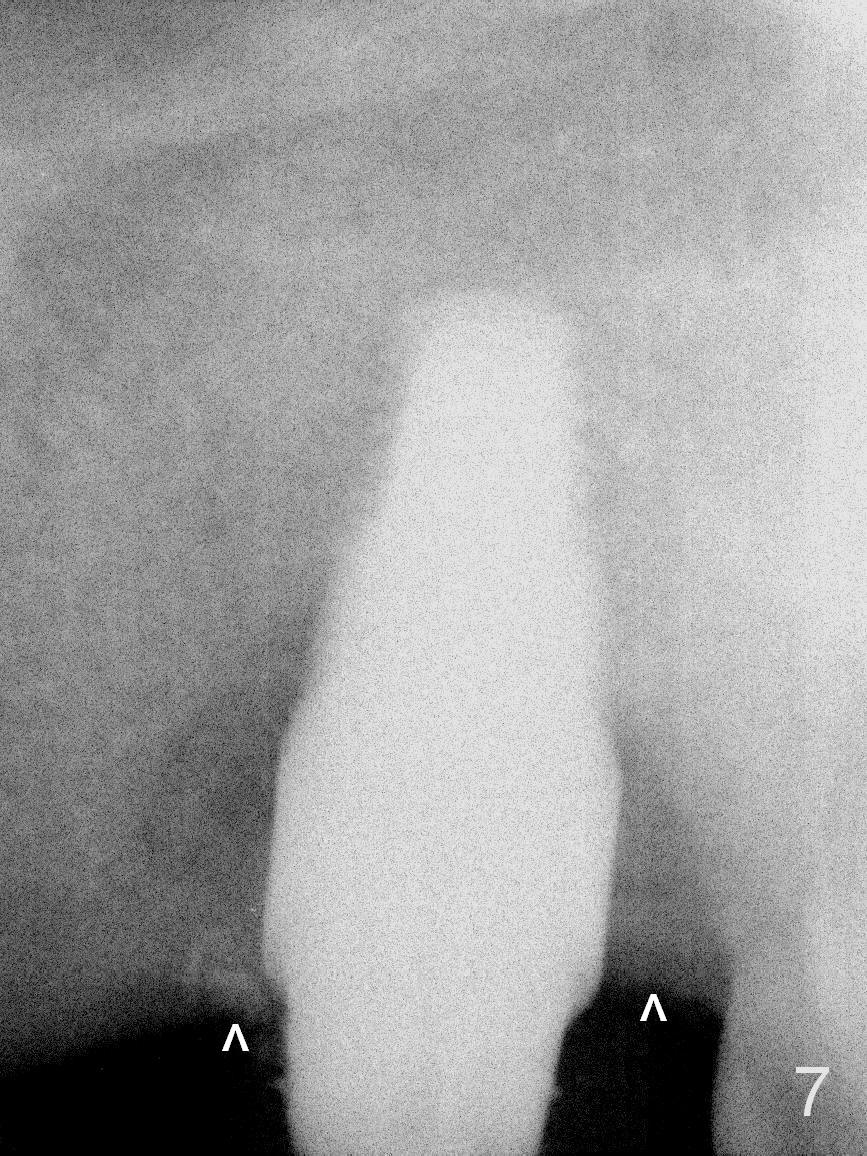
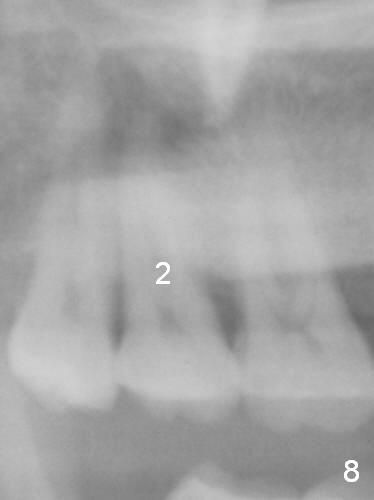
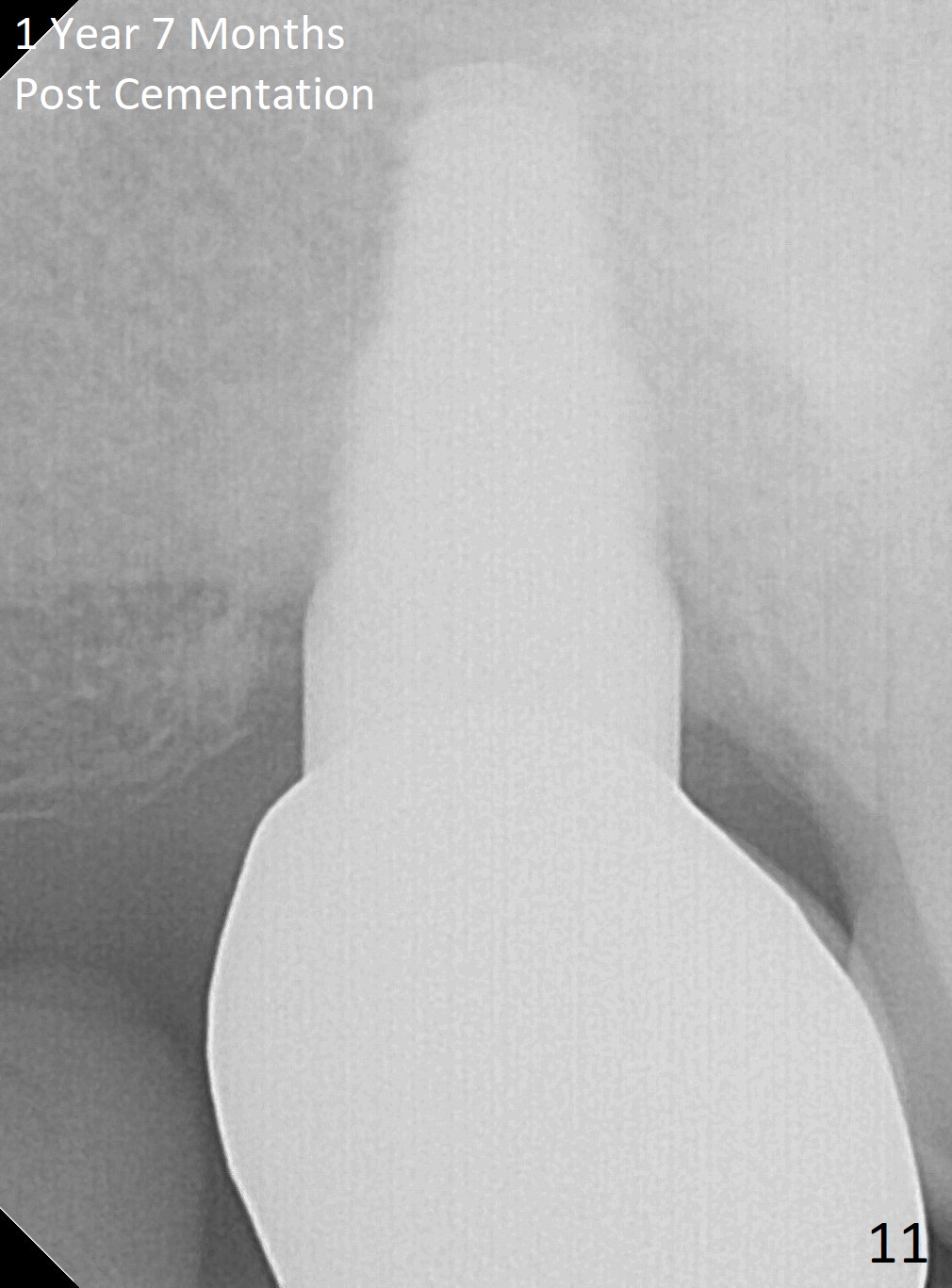
There is bone density change at the mesial and distal crests 3 months postop (Fig.7 ^) and 7 months post cementation (Fig.10 (Dec. 2016 (Pano)), as compared to Fig.8 (May 2007) and 9 (Aug 2014)). The mesial gap has apparently closed 1 year 7 months post cementation (Fig.11).
Return to Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 01/07/2016, last revision 12/31/2017