

|
|
|
|
|
|
|
|
|
|
Several Steps to Change Osteotomy Position and Trajectory
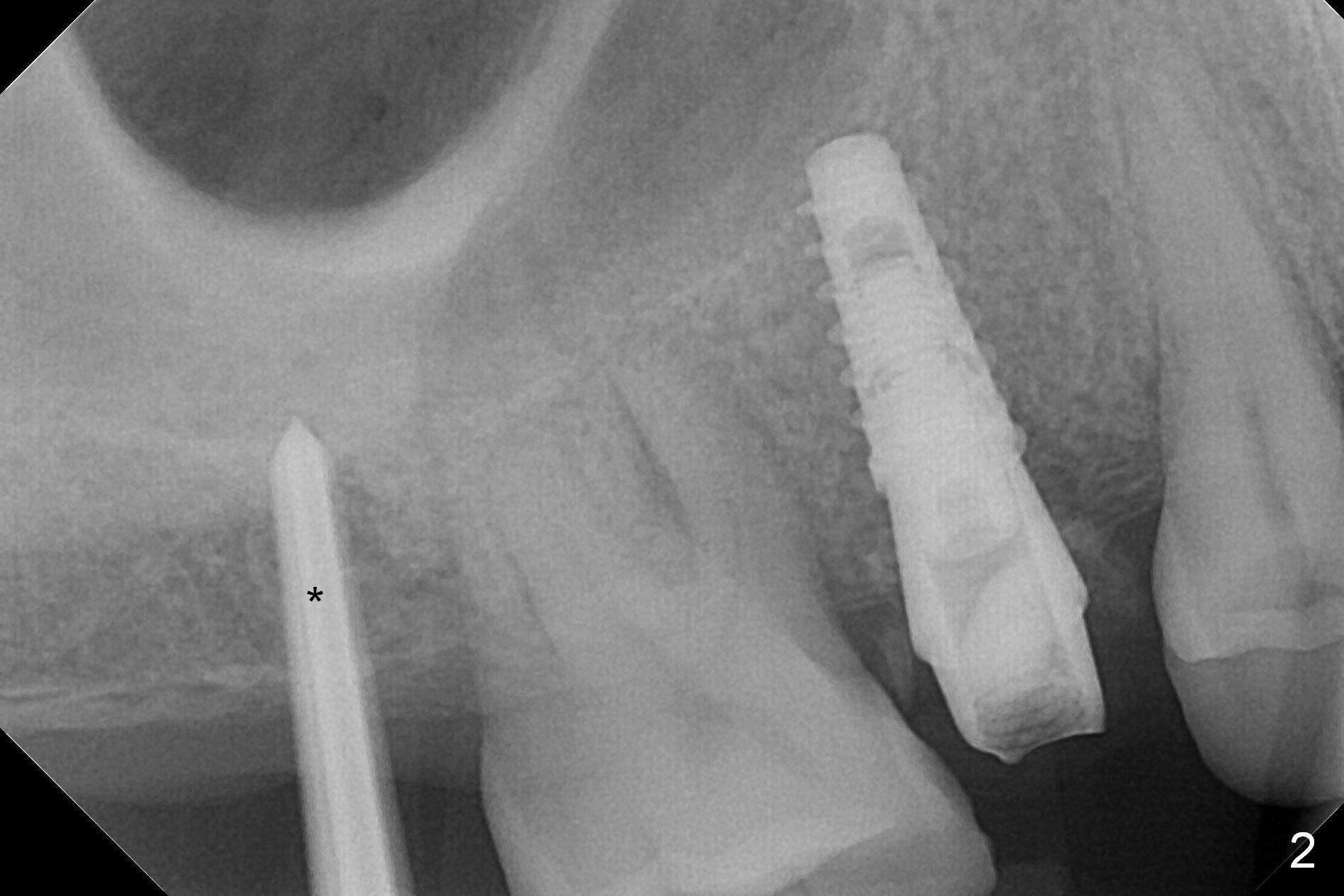
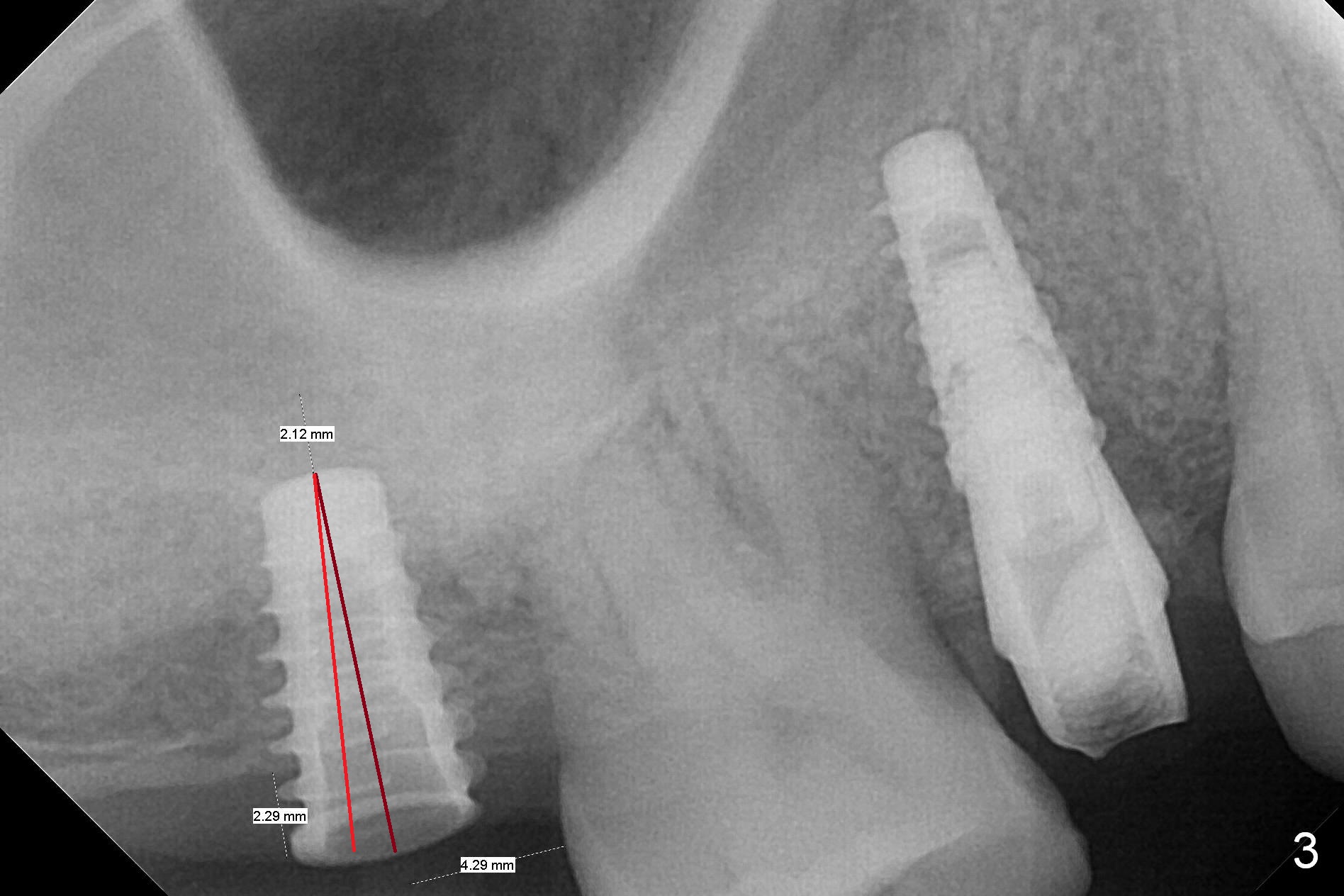
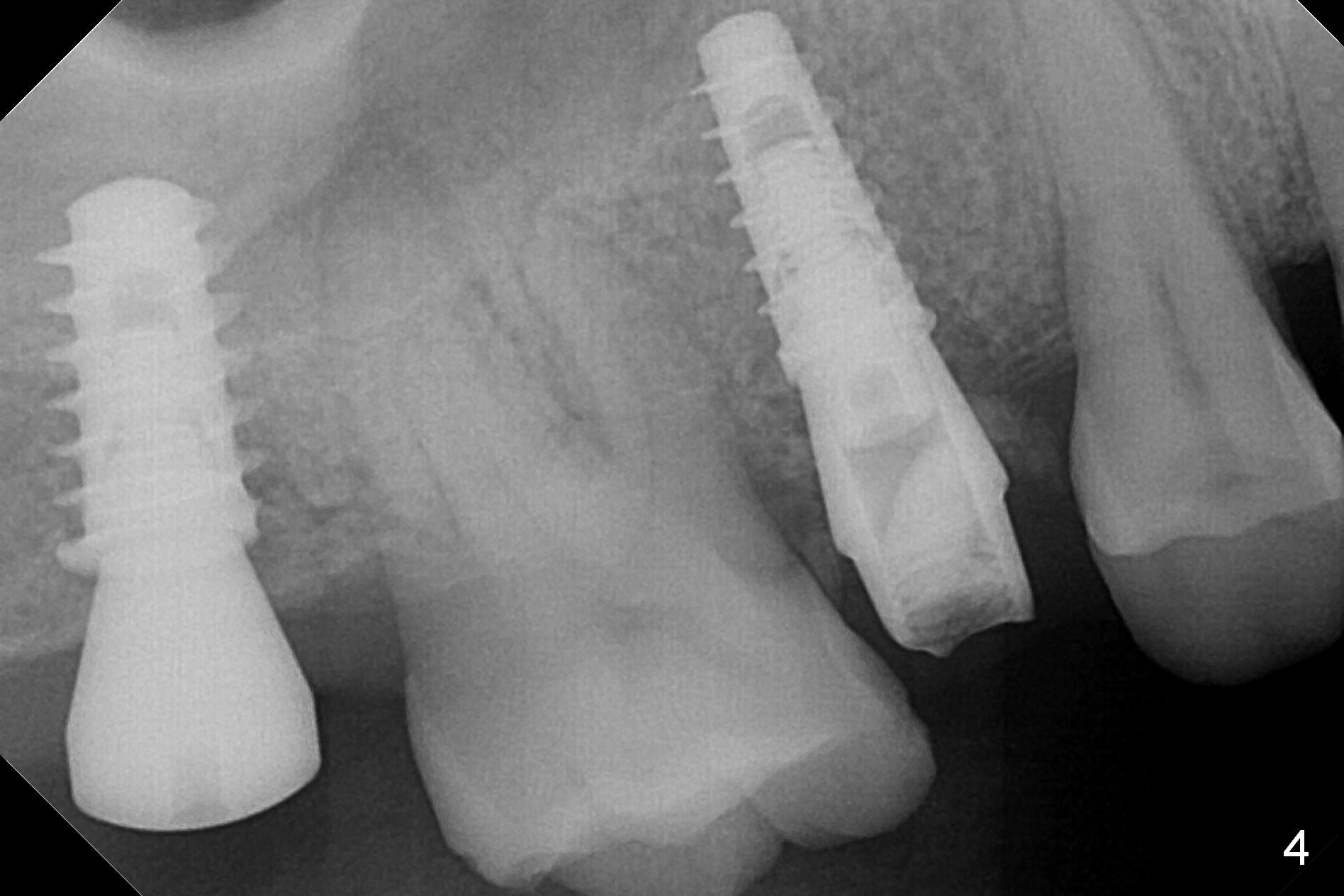
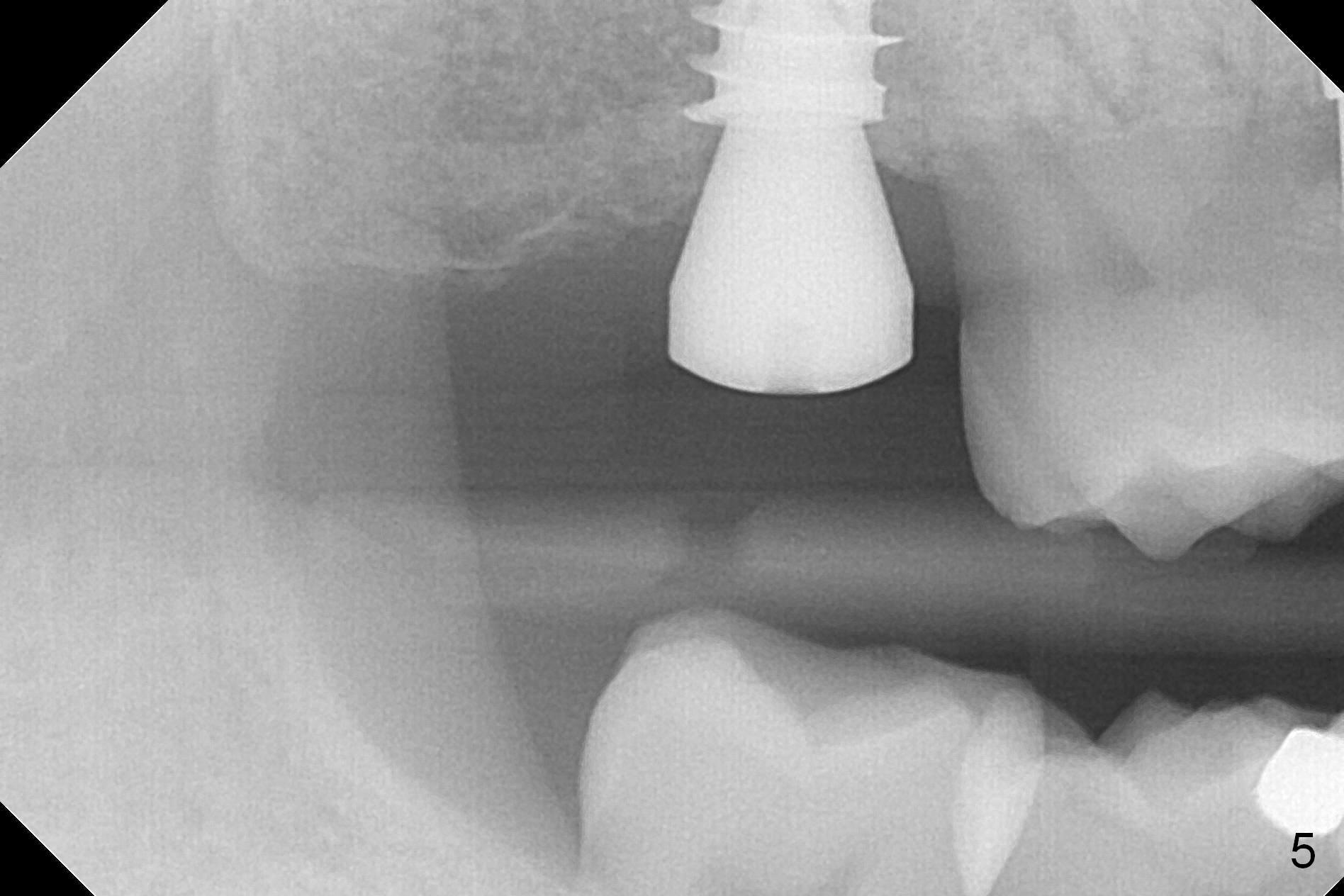
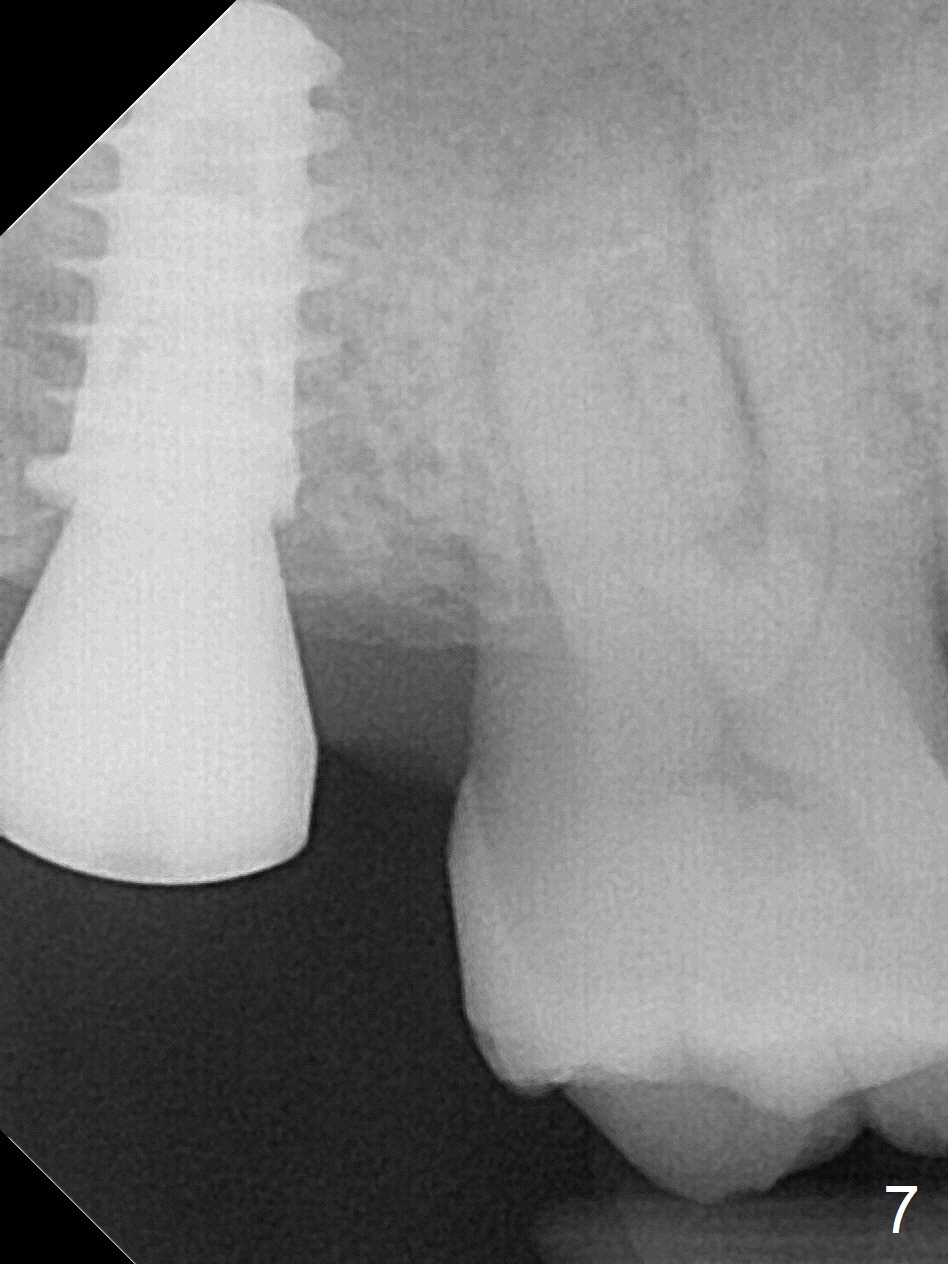
Since the ridge at the site of #2 is wide (Fig.1), Magic Split is used for access and bone density determination. In fact it enters for 9 mm (gingival level), followed by Magic Expander (ME) 3 mm (Fig.2 *). The center of the latter is 3.9 mm from the distal surface of the tooth #3. Lindamann bur is used to move the osteotomy distal, followed by sequential use of MEs until 4.3 mm one. When a 5x9 mm dummy implant is placed, its center is somewhat mesial (Fig.3 brown line). What needs to be done is change the trajectory to the red line so that the coronal end of the definitive implant (5.5x9 mm) will be placed evenly subcrestal (Fig.4,5). It is what happens, although slightly too subcrestal. Insertion torque is <35 Ncm; a 6x4 mm healing abutment is placed. ME 4.8 mm has to be tapped for 13 mm from gingival margin in order to let the implant penetrate the sinus floor. IBS implants seem to lack self tapping ability. Its tap drills should possess this capacity. Allograft/autogenous bone (harvested from dummy implant) is placed prior to implantation. The patient returns for impression 6 months postop (Fig.6,7; #4). A 5x4(3) mm abutment is placed; its height is reduced as well as the opposing supraerupted tooth (Fig.5) prior to impression.
Return to
Upper
Molar Immediate Implant
1st
Year Course
1 2
Xin Wei, DDS, PhD, MS 1st edition 01/09/2017, last revision 07/30/2017