
|
|
|
|
||
|
|
|
|
|
|
|
|
||||
Apparently Unlimited Bone Height for Upper 2nd Molar
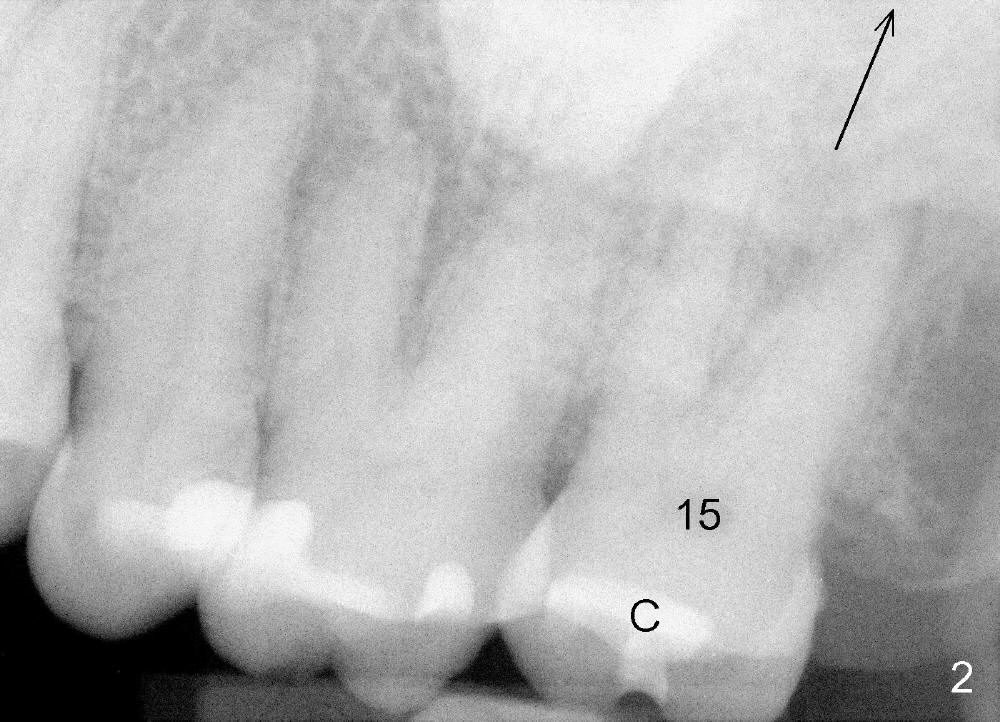
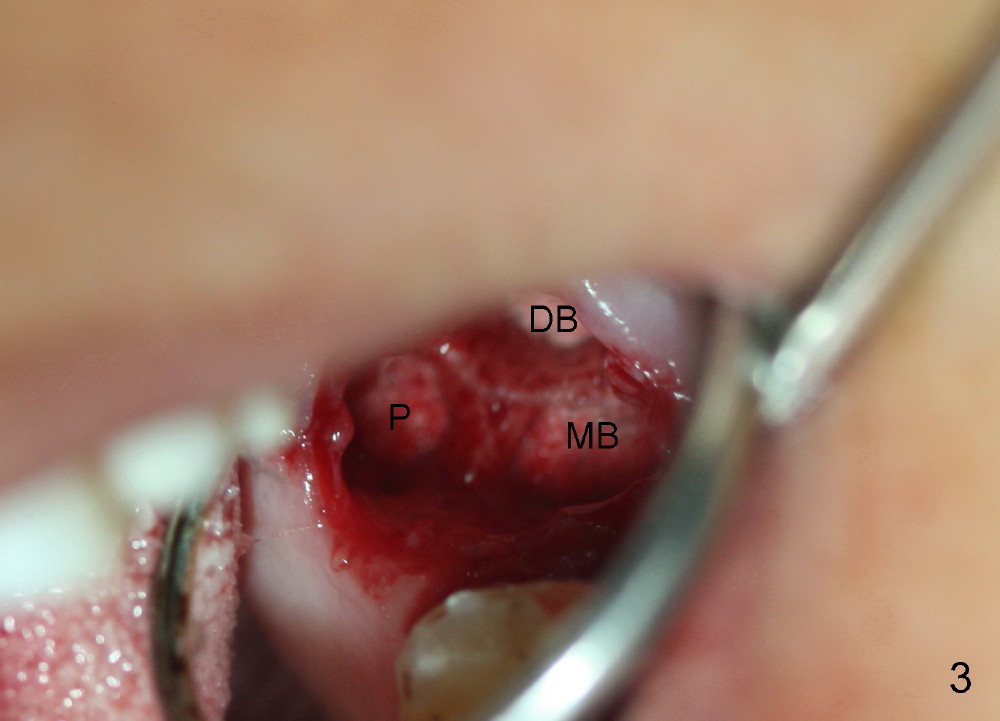
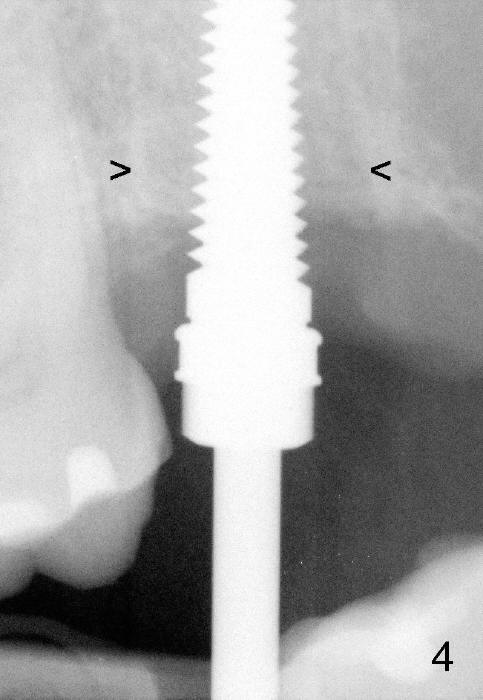
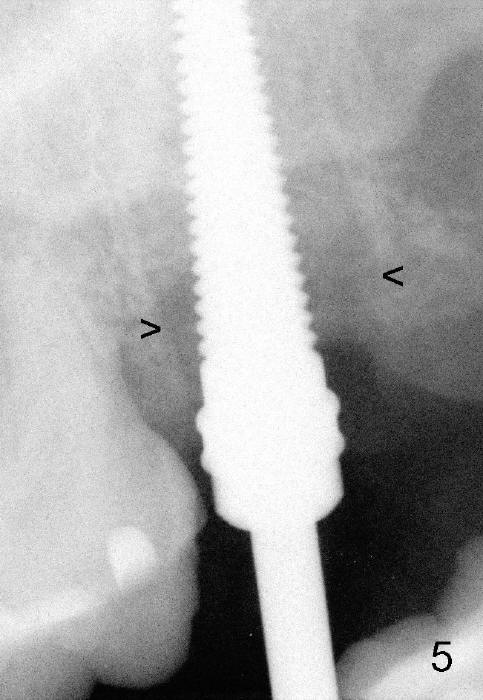
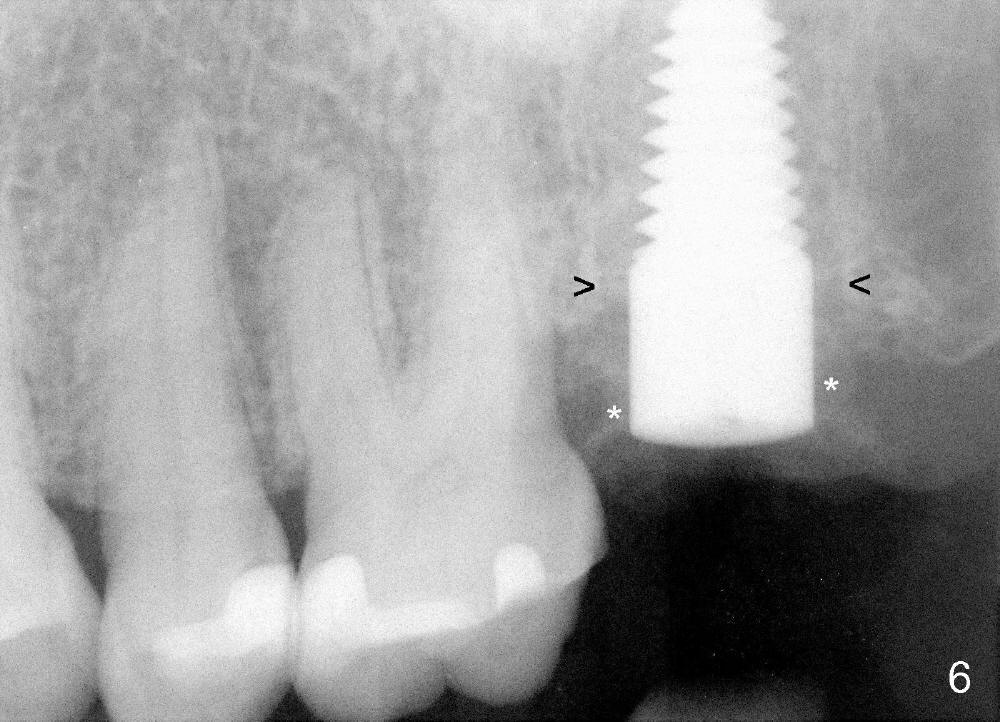
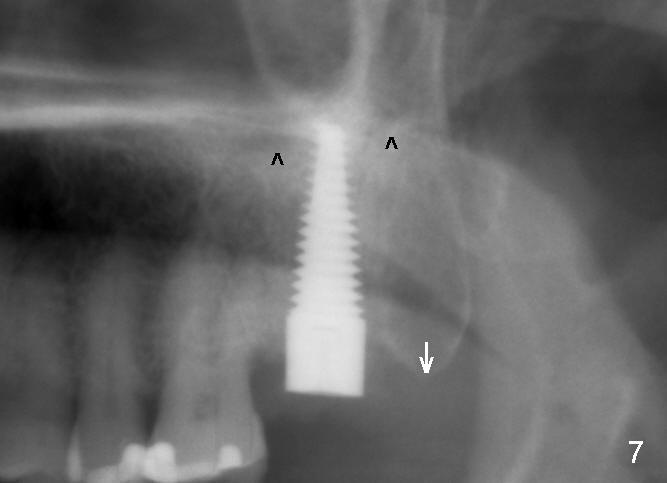
A 57-year-old lady presents for abscess buccal to the tooth #15 (Fig.1 A). Mesial and distal to the occlusal composite (Fig.2 C) is a crack line. In addition to long furcated roots, the upper border of the bone is not shown in this preop PA (arrow). Fig.3 is taken to show a thin septum surrounded by the mesiobuccal (MB), distobuccal (DB) and palatal (P) sockets (Fig.3). Osteotomy is initiated in the septum by 1.2 and 1.5 mm pilot drills, followed by 2,3,4 mm rounded tapered osteotomy at the depth of 17 mm. Nose blowing test is carried out after each step with negative result. Stability is achieved when a 4.5 mm tap is inserted at 17 mm, but the upper end of the tap is not visible (Fig.4,5). When a 5 mm tap is placed, stability is decreased, probably because the coronal end of the septum starts to break down (due to expansion). To re-gain stability, the 5 mm tap needs to go deeper. A 6 mm tap also achieves satisfactory stability at 20 mm. When the tap is removed, there is no air leakage. A 6x20 mm implant is placed with insertion torque > 60 Ncm; the upper end of the implant is still out of view in PA (Fig.6). Another problem is that the implant needs to go deeper to obtain sufficient occlusal clearance. The lower first molars and the 2nd premolars are missing. A panoramic X-ray has to be taken to show the apical end of the implant: ~ 3 mm into the sinus (Fig.7 ^). The maxillary tuberosity appears to grow downward (arrow). In other word, the tooth #15 appears to have been intruded due to overloading.
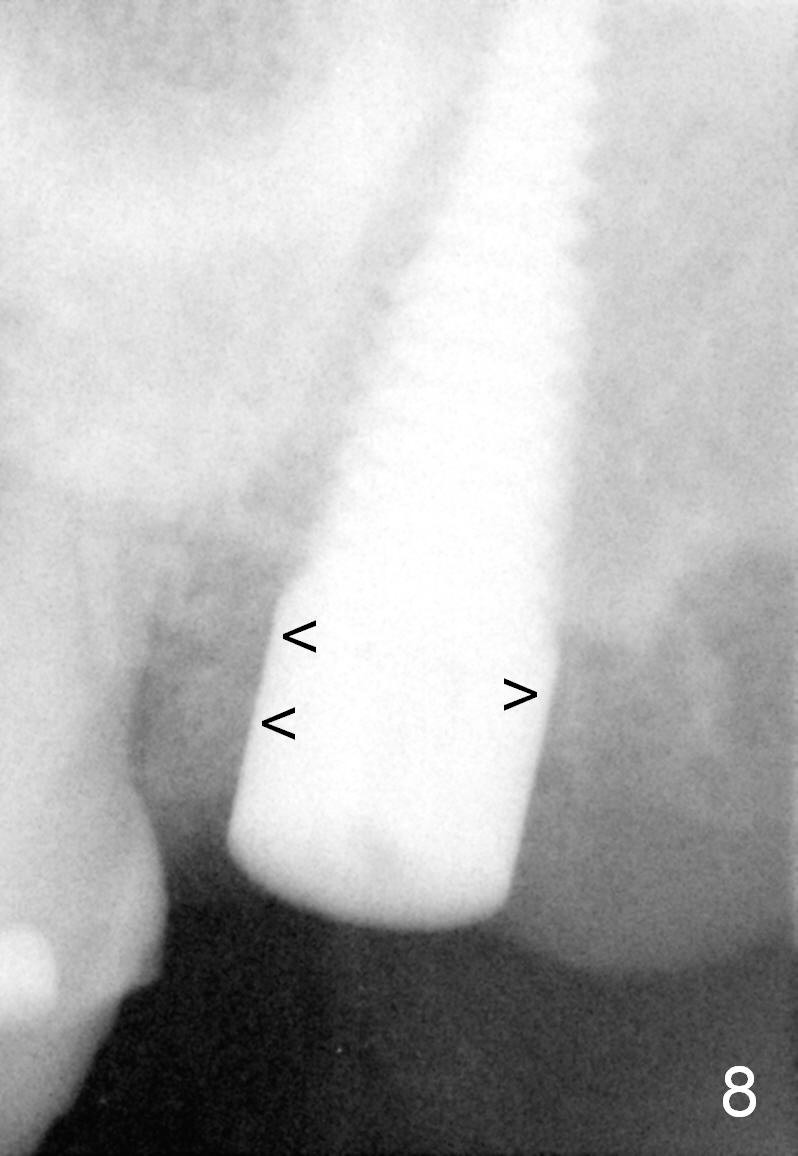
The mesial and distal socket spaces apparently disappears 3 months postop (Fig.8).
Return to Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 12/12/2014, last revision 07/31/2015