




|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
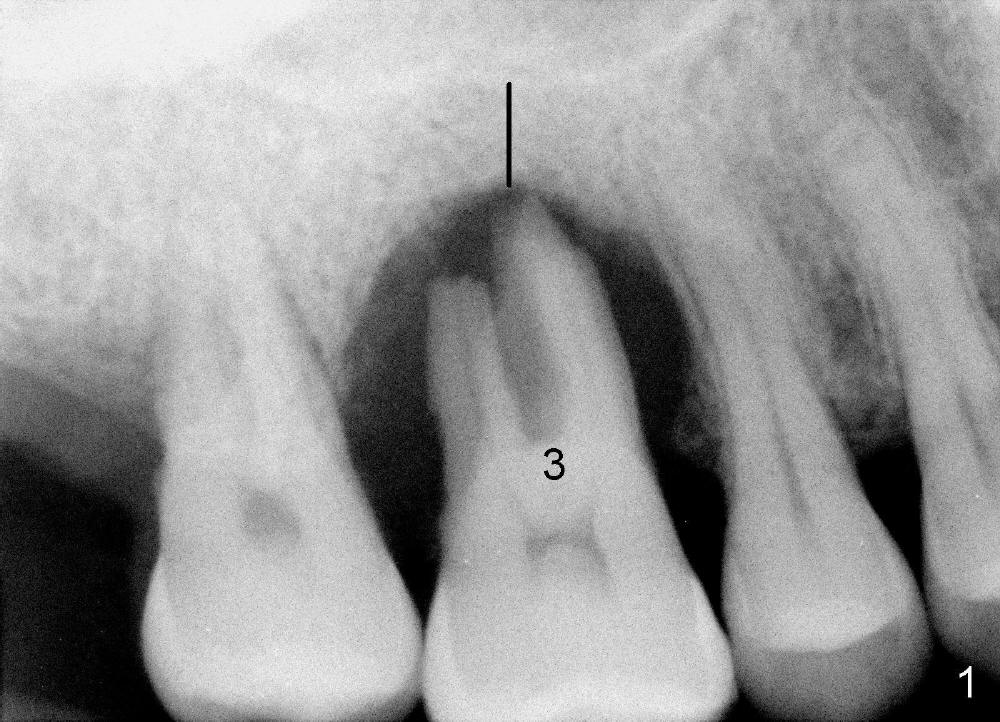
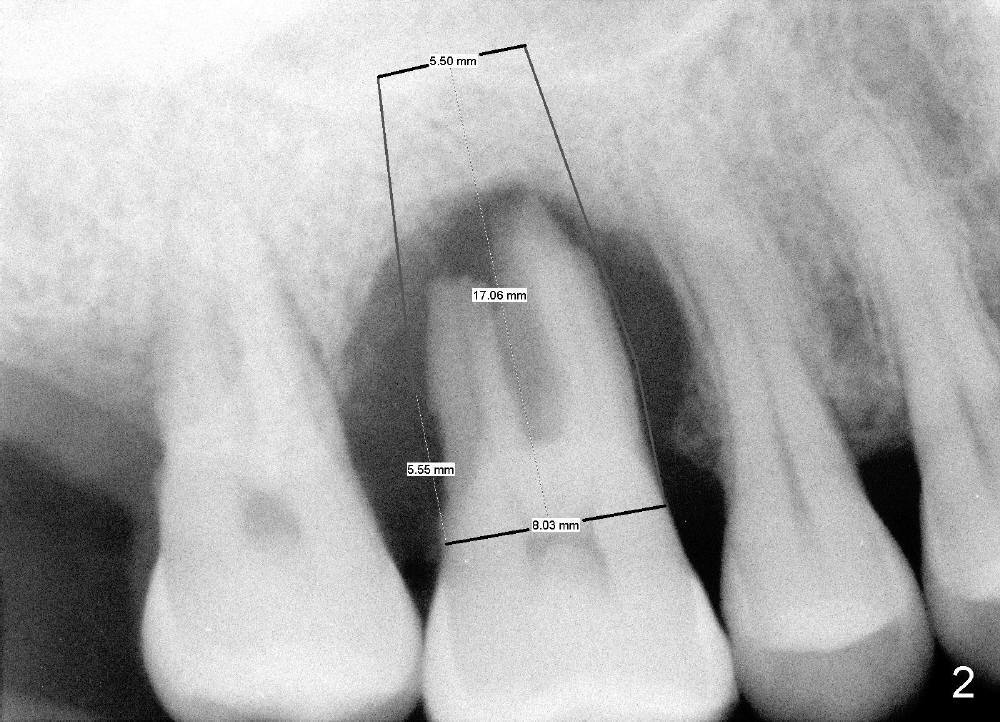
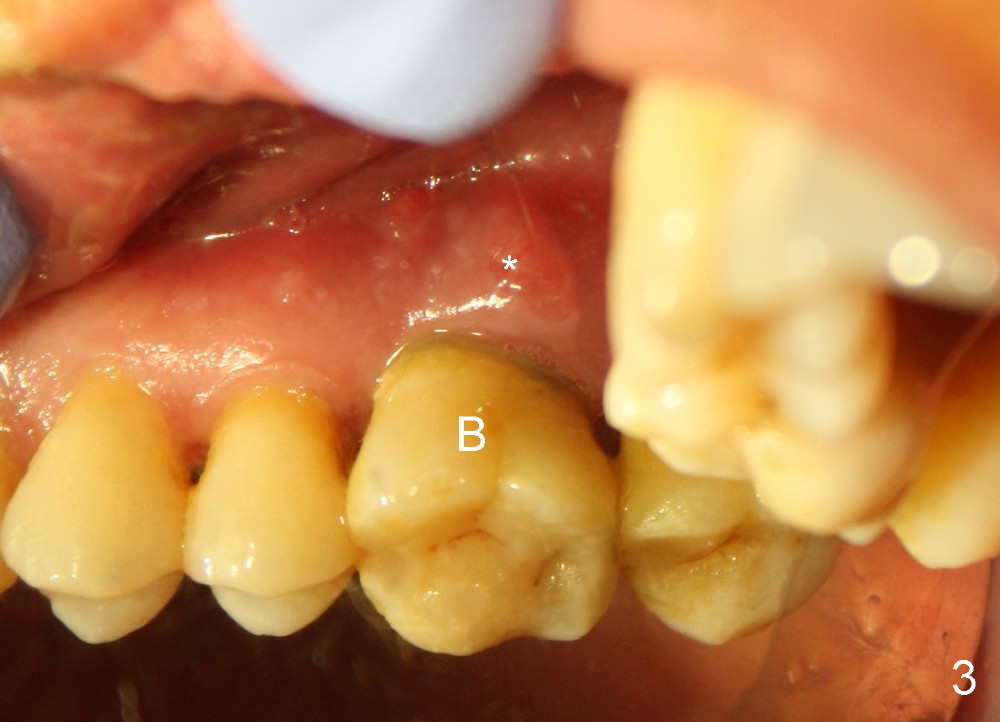
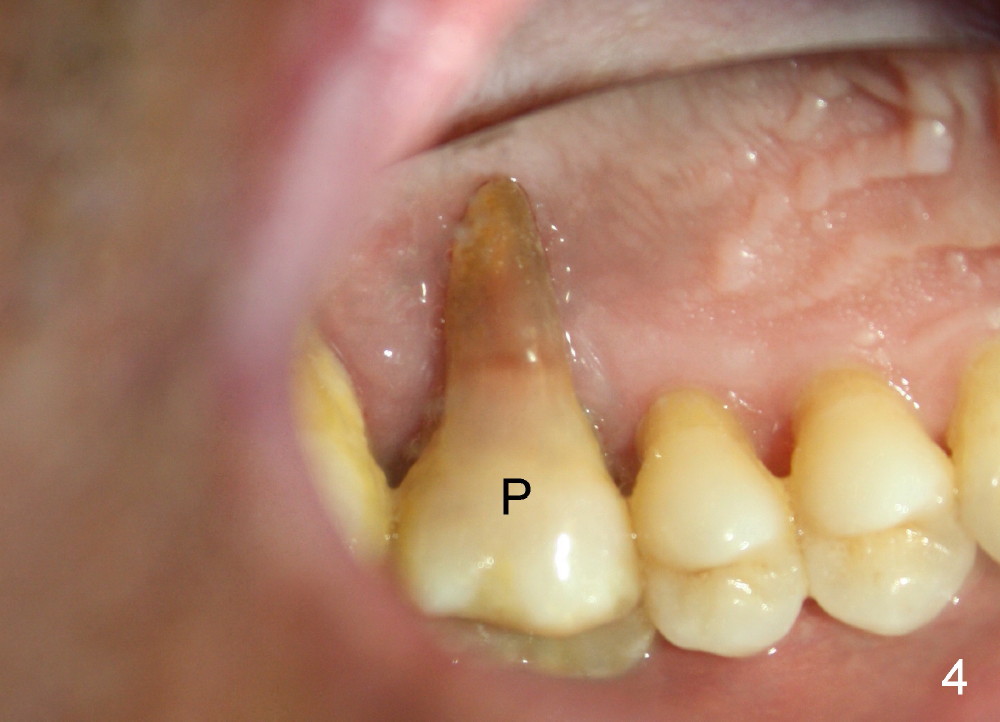
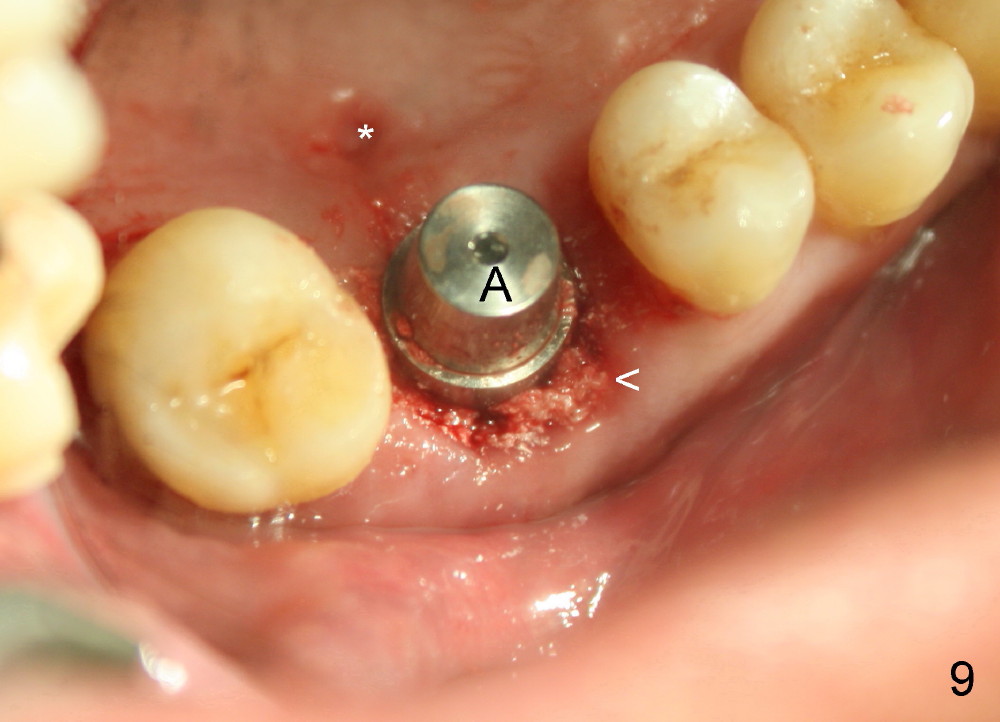
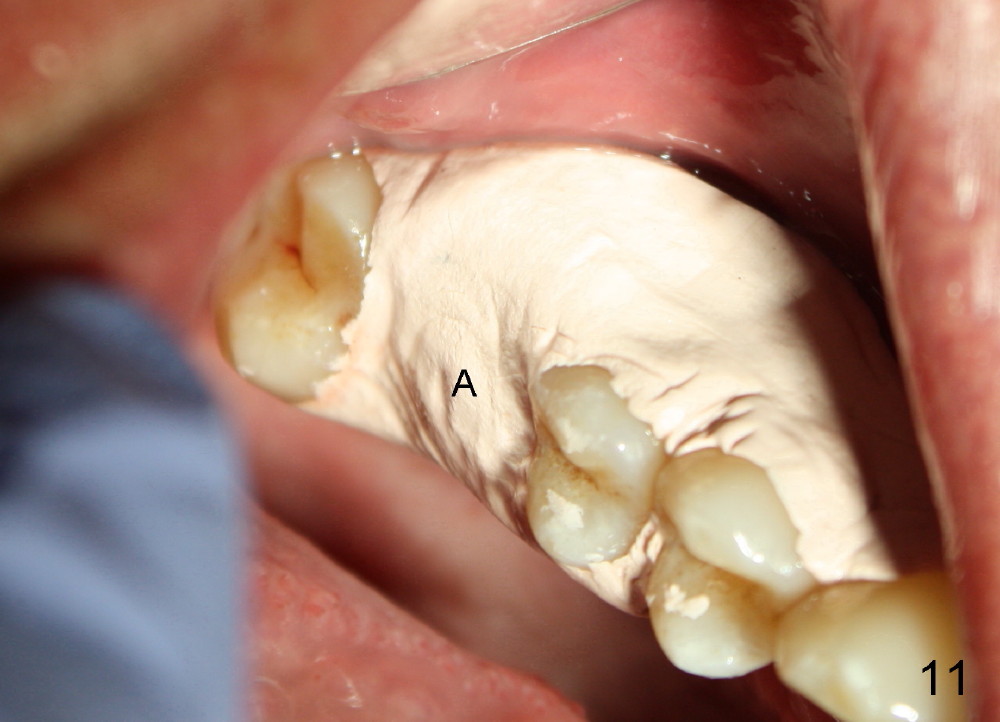
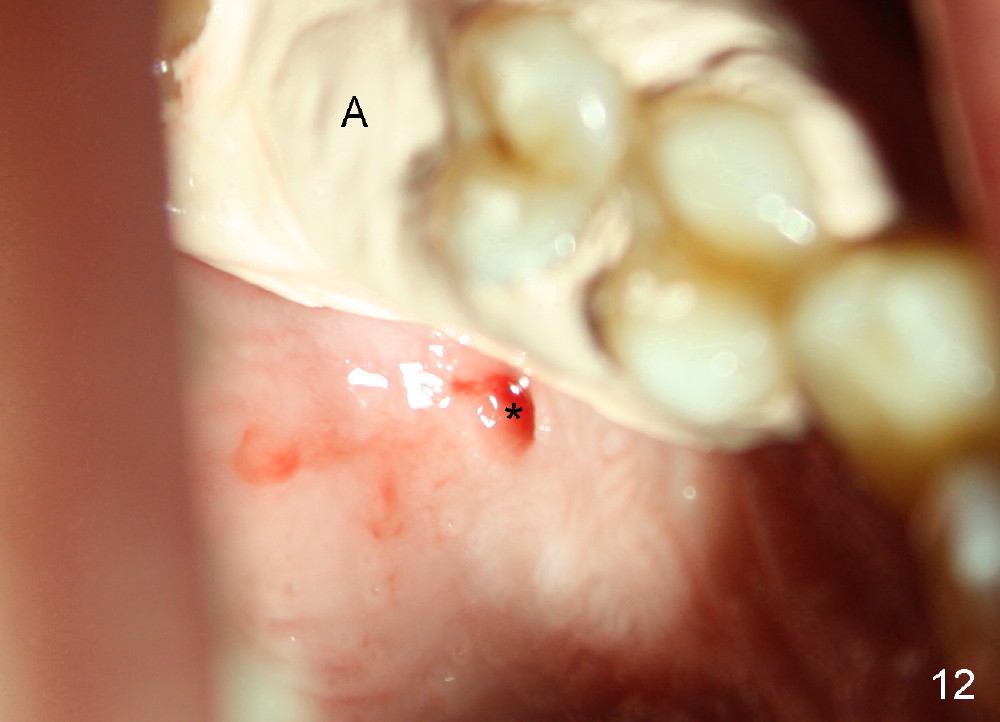
Perio Dressing Closes Molar Socket after Immediate Implant
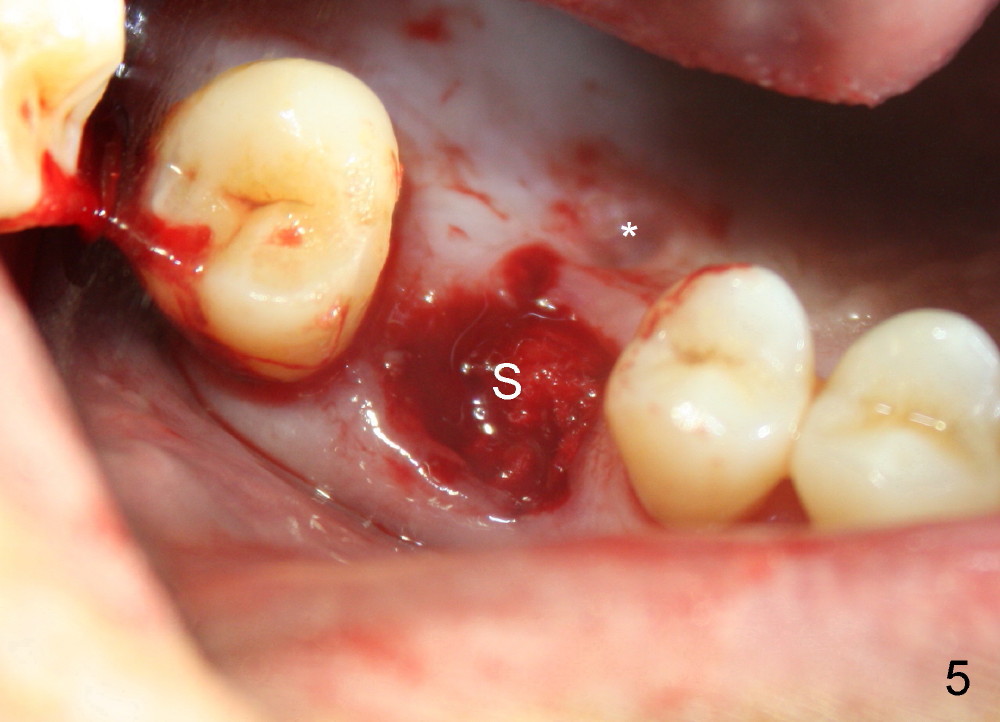
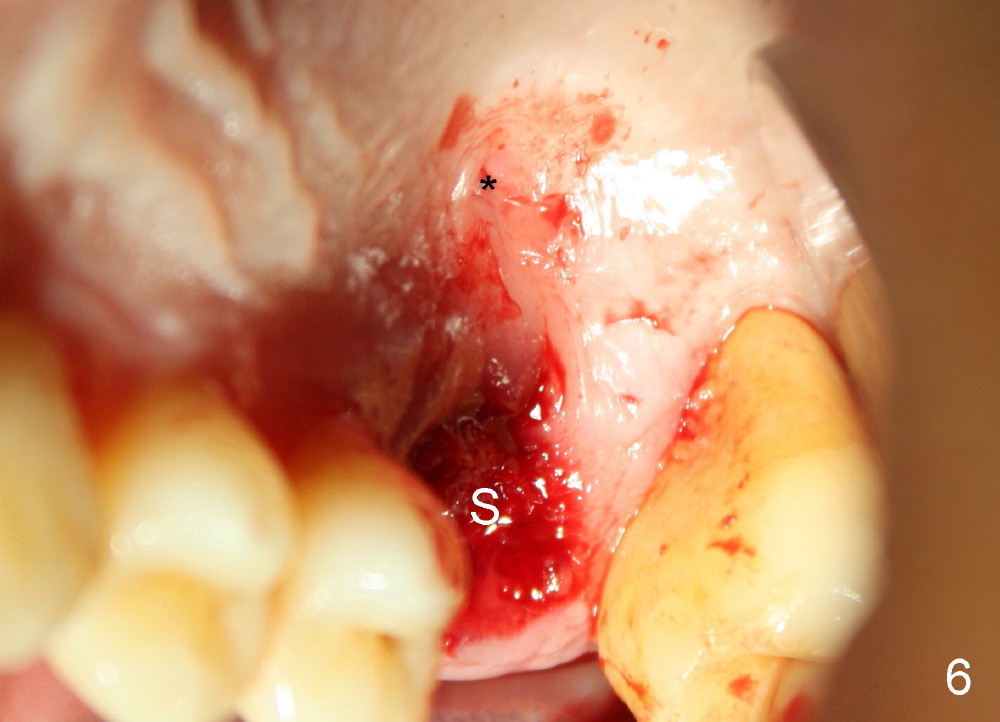
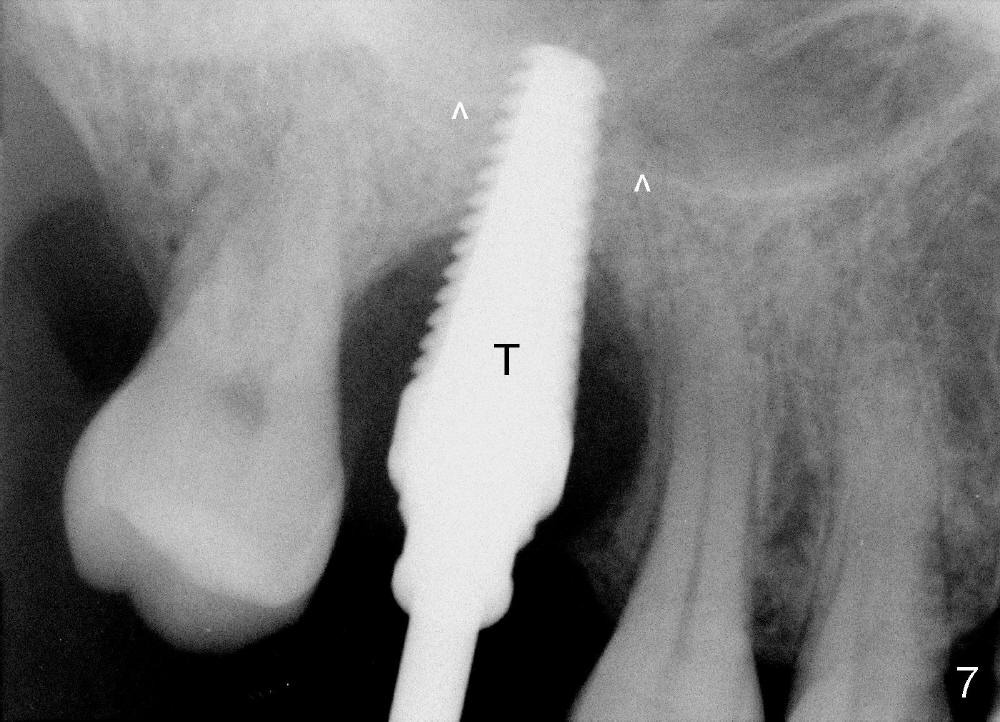
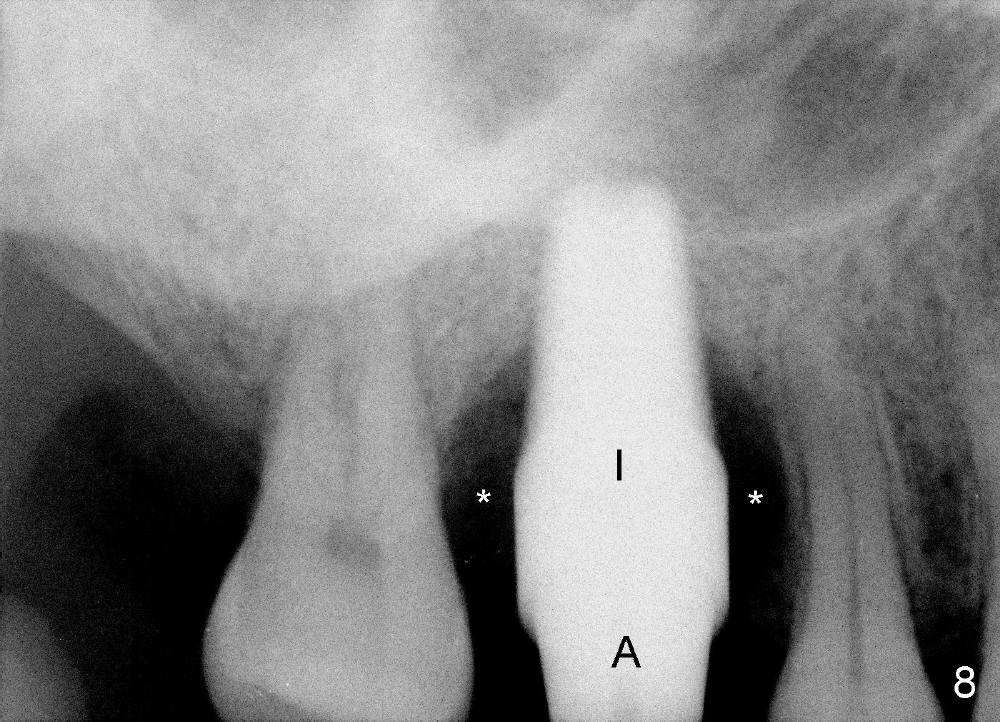
The upper right 1st molar of a 48-year-old man has severe perio endo disease (Fig.1 #3); the bone height for immediate implant (Fig.2) is about 3.5 mm (Fig.1 vertical line). There is a buccal (Fig.3 B) abscess (*); the palatal (Fig.4 P) root is exposed. After extraction, the socket available for immediate implant (Fig.5,6 S) is buccal (without septum), whereas the apex of the palatal root is far away from the main socket. In fact there is an advantage: the socket is smaller. Osteotomy is created in the main socket as palatal as possible, using osteotomes, reamers and taps (Fig.7 T). The sinus floor is lifted (Fig.7 ^). When 7x17 mm implant is placed (Fig.8 I), the insertion torque is >60 Ncm. The remaining socket (Fig.8 *) is to be packed with mixture of autogenous bone, allograft and synthetic bone (Osteogen) (Fig.9,10 <). Immediate insertion of an abutment (Fig.8-10 A) helps retain perio dressing (Fig.11,12). No collagen membrane is used in this case to cover the bone graft before placement of perio dressing. Postop the patient cannot tolerate oral Amoxicillin because of stomach upset. The dose is reduced. Two weeks postop, the perio dressing is stable, but discolors (Fig.13). When the dressing is removed, the buccal bone graft is exposed, which is not abnormal. What is unusual is discoloration (Fig.14). The significance of the latter is not revealed until 3 months postop when the patient remains asymptomatic, but there is an apical fistula (Fig.15 <). There is a communication between the fistula and the buccal sulcus of the implant: water passing freely. Based on the position of the buccal plate of the neighboring teeth (*), the buccal plate of the implant should be lost, which is consistent with finding of PA (Fig.16, as compared to Fig.8). Guided bone regeneration seems necessary.
Return to Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 09/06/2014, last revision 01/19/2018