|
|
|
|
|
|
|
Use of Temporary Abutment to Close Socket of a Molar
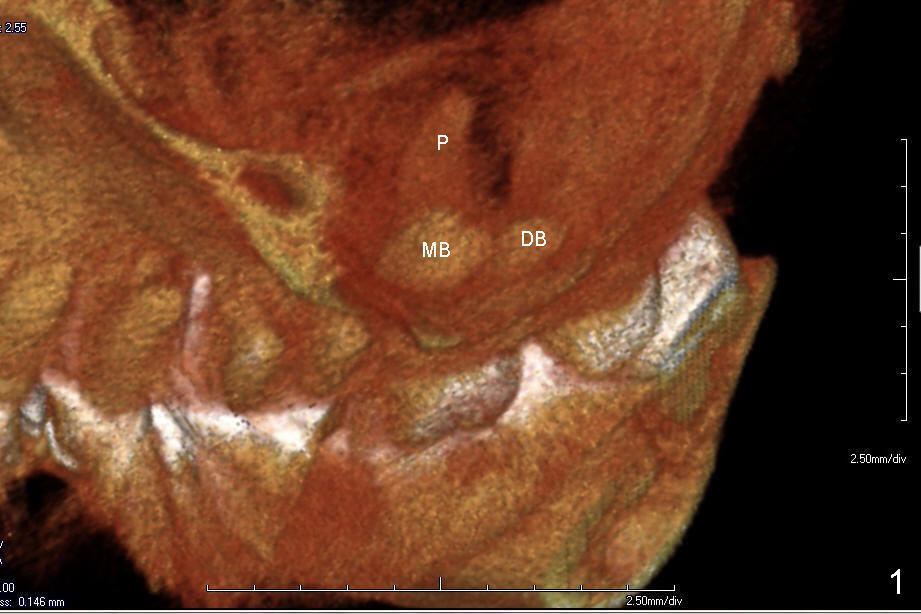
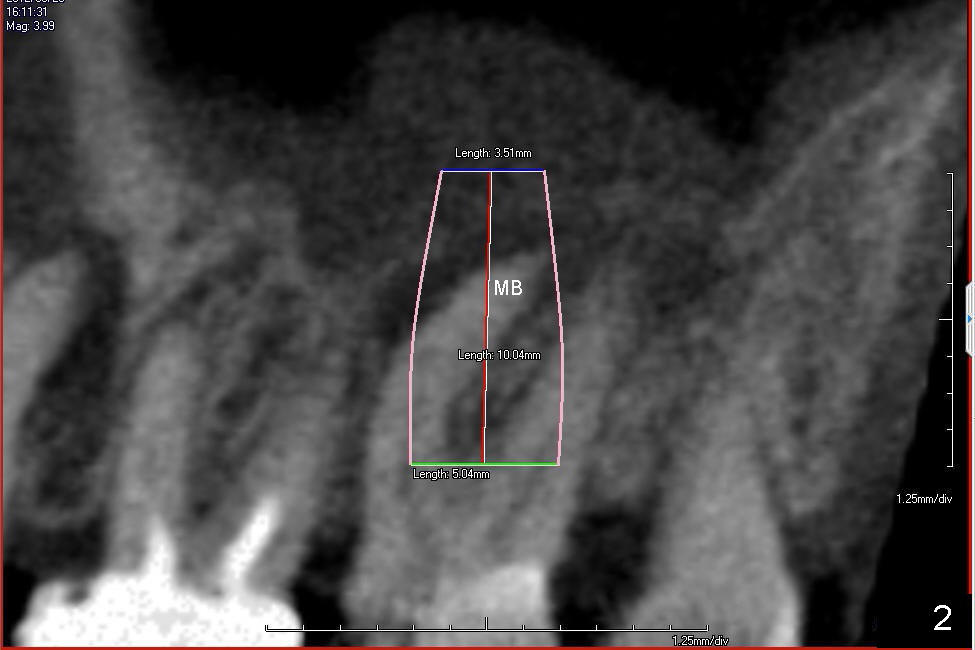
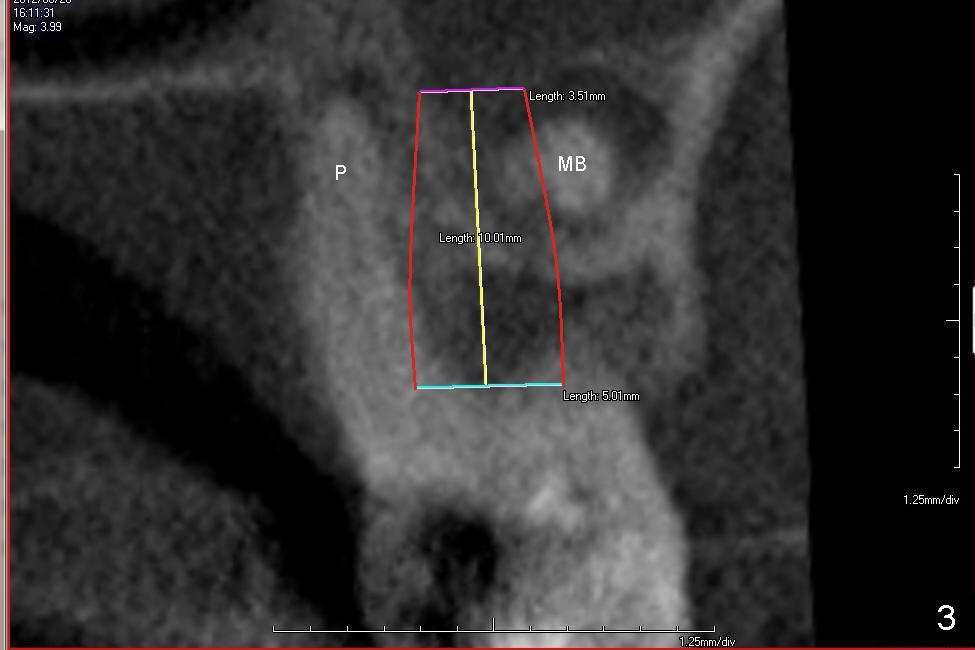
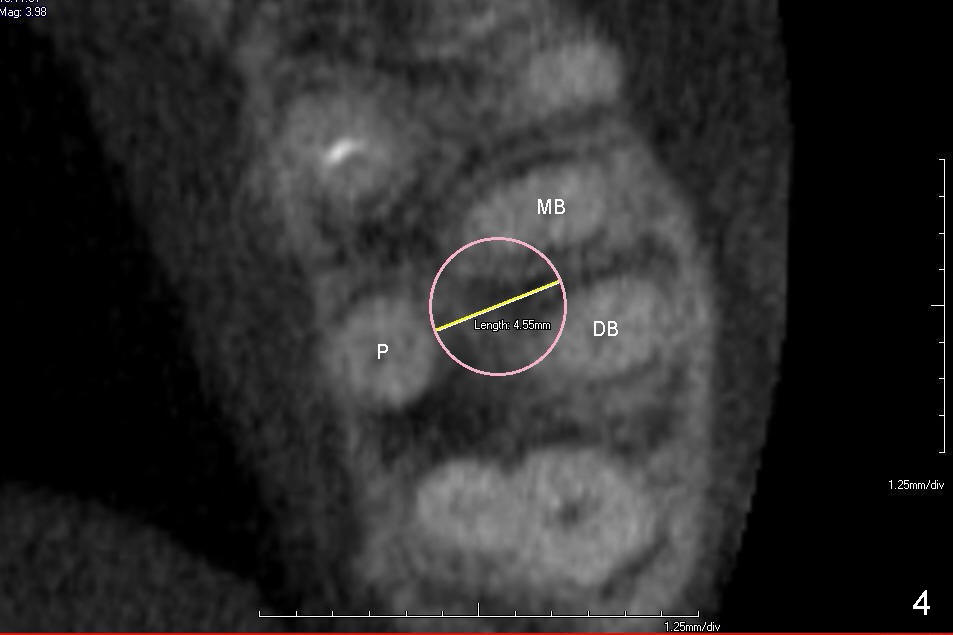
Clinically the proximal caries of the tooth #15 of a 66-year-old lady is subgingival and nonsalvageable. CBCT images show that roots are widely divergent (Fig1 (3D), 2 (Sagittal), 3 (coronal), 4 (axial section). Prepare surgical handpiece for sectioning. The mesiobuccal (MB, Fig.2) root tip is curved. It may break. Root tip picks should be available. Extensive apical lesions in Fig.1-3 suggest that there is abundant granulation tissue, which will be removed more easily with a new instrument: a serrated curette, than the regular curette or Molt curettes.
If the septum is big and strong enough, start with 1.5 mm pilot drill,
followed by RT2, alternated with reamers and RTs. Then a 4.5 or 5 x10 mm submerged implant
is placed. A temporary abutment is placed. A temporary crown is
fabricated to close the socket. There is no occlusal contact with the
opposing tooth,
at all. If the septum is
destroyed by the infection, a larger implant is used instead, probably
cylindrical.
Xin Wei, DDS, PhD, MS 1st edition 02/15/2014, last revision 02/16/2014