|
|
|
|
|
|
|
|
|
|
Osteotomy in Soft Bone
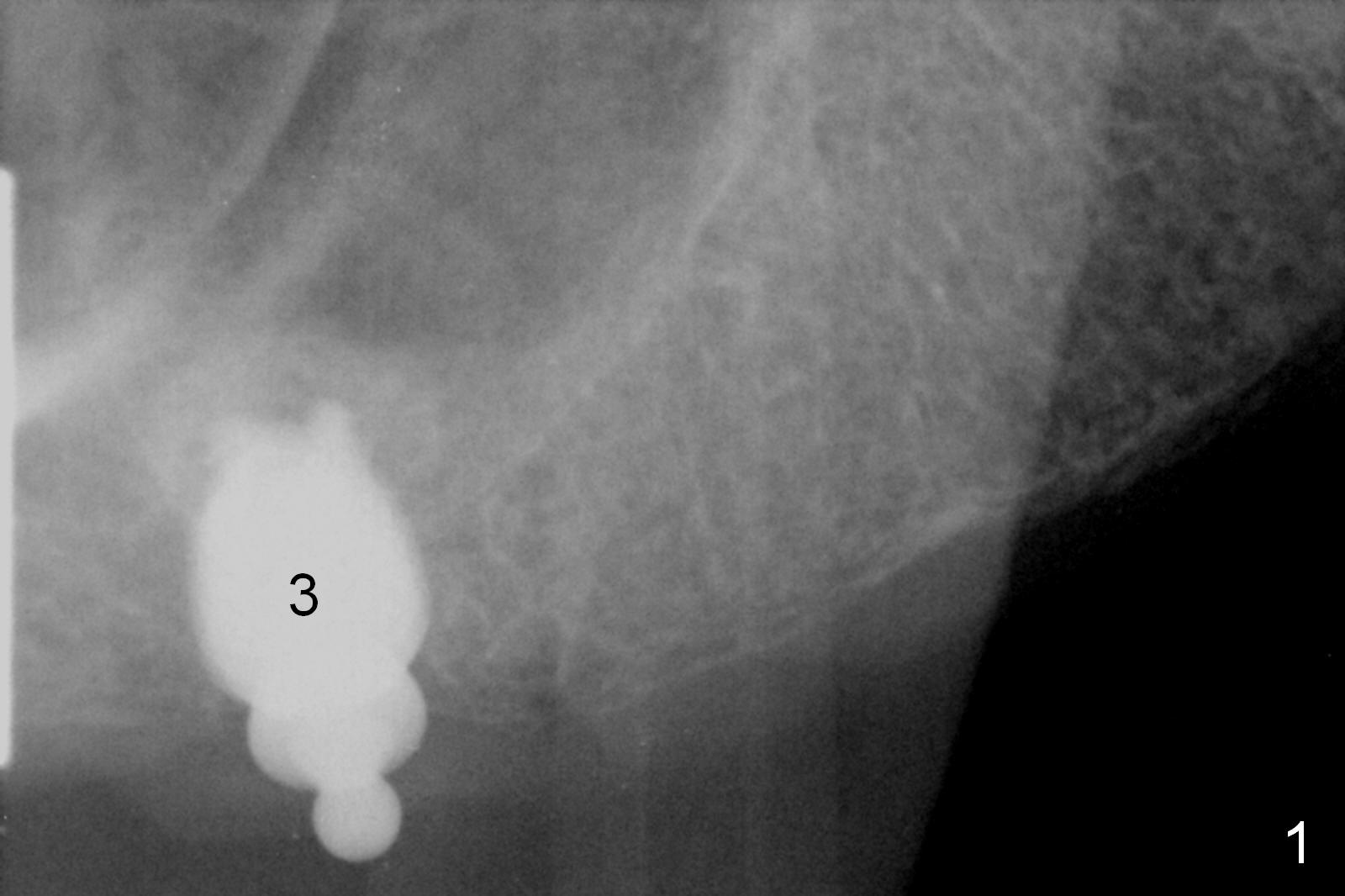
Osteotomy at the site of #3 turns out to be easy, starting with 2 mm initial drill, 2.8 and 3.6 mm round drills at 5 mm. The depth intends to increase to 6 mm, in fact to 9 mm without sinus membrane perforation. The osteotomy continues to increase by using 4, 4.5, 5, 5.3 and 5.9 mm taps at 6 mm deep. Allograft/Osteogen is placed for sinus lift prior to inserting a 5.9x6 mm SM implant (>50 Ncm, Fig.1).
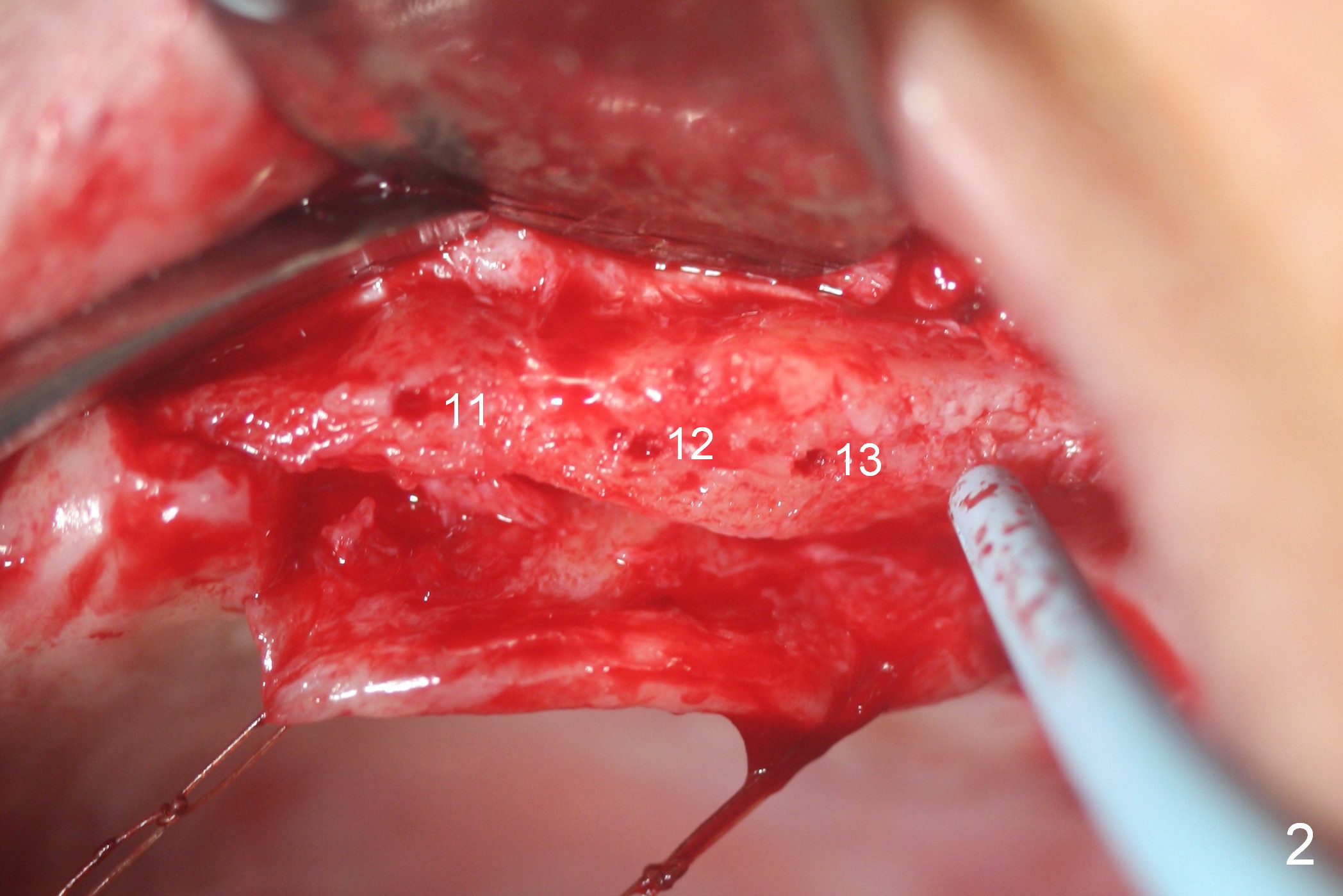
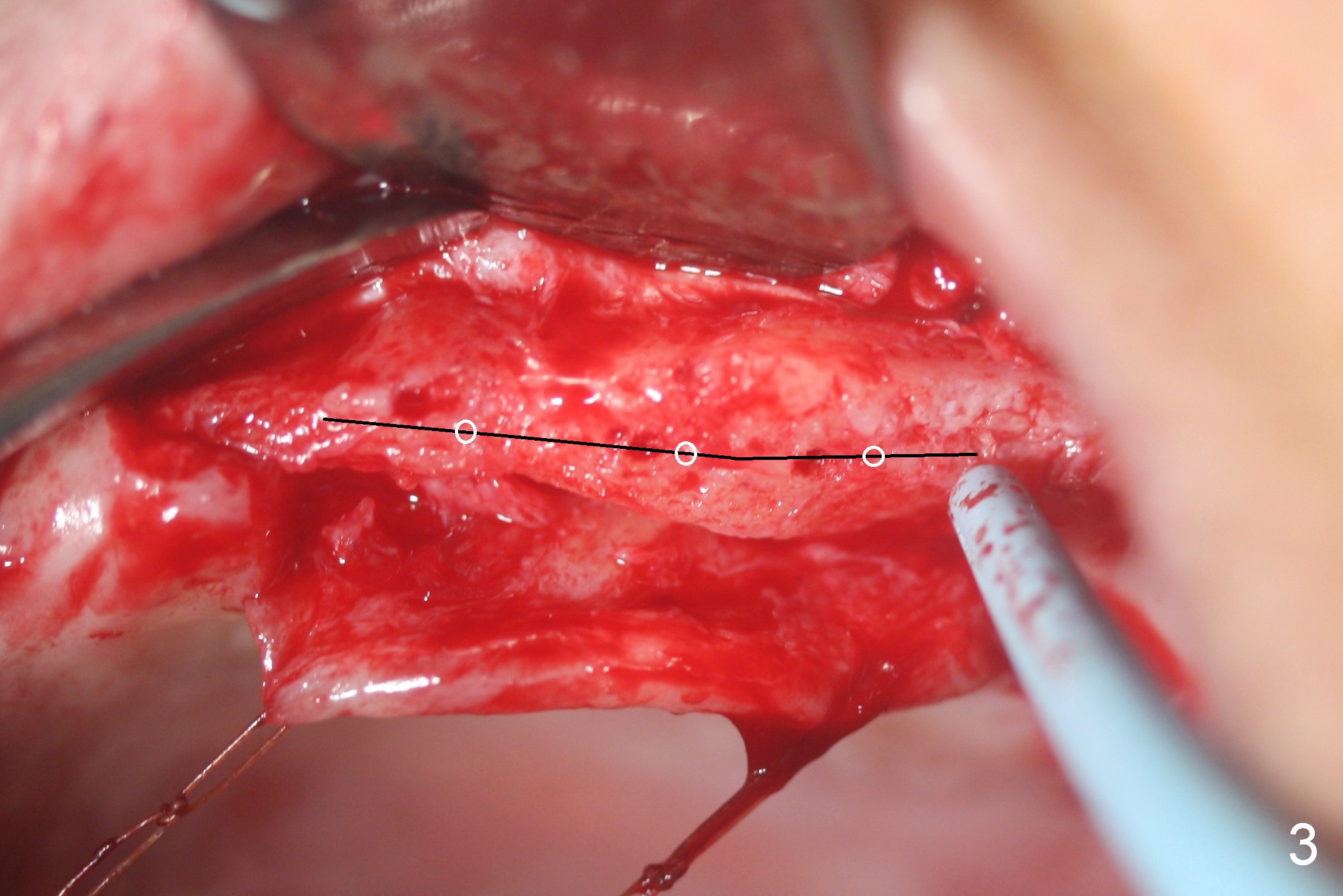
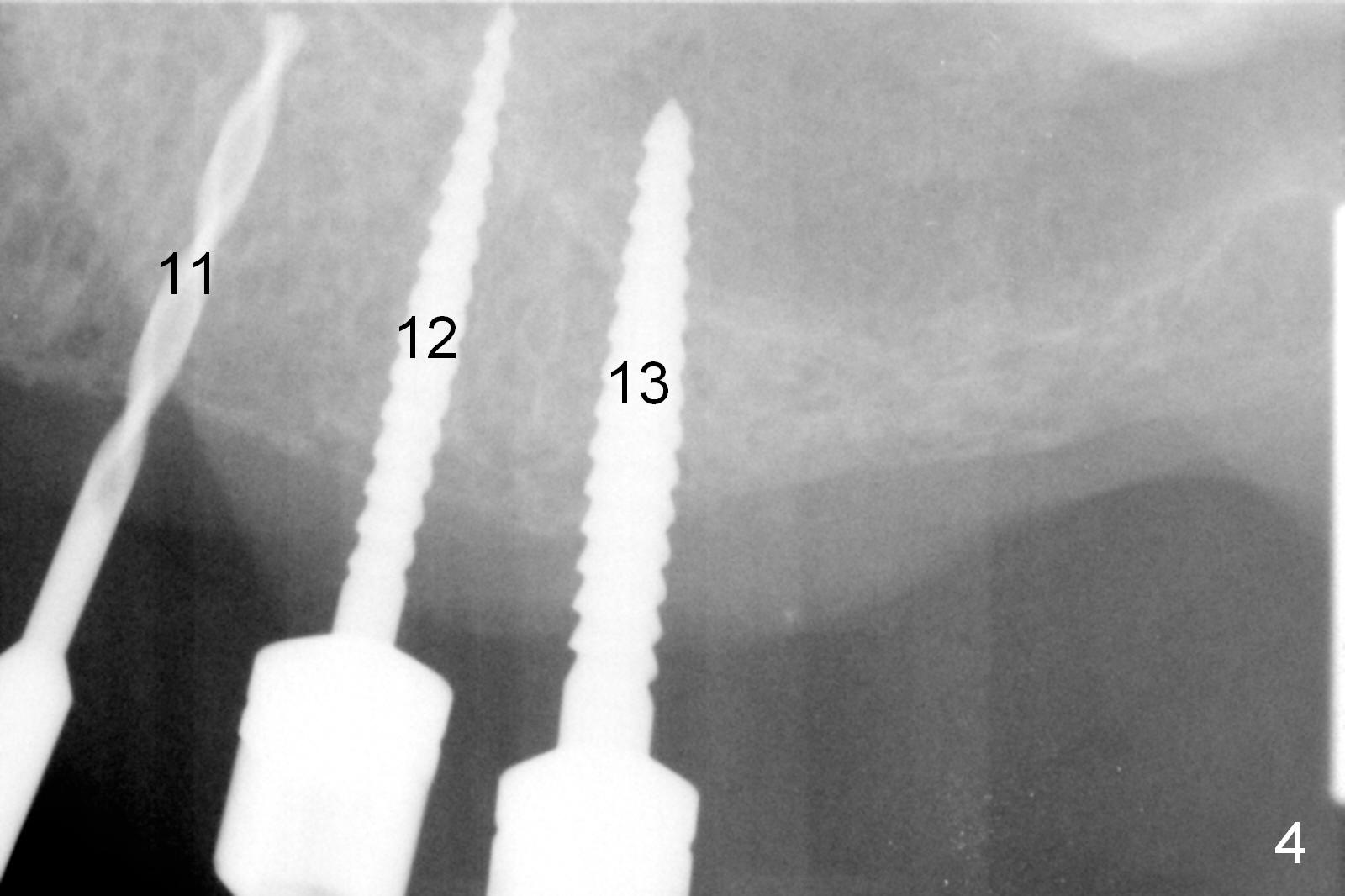
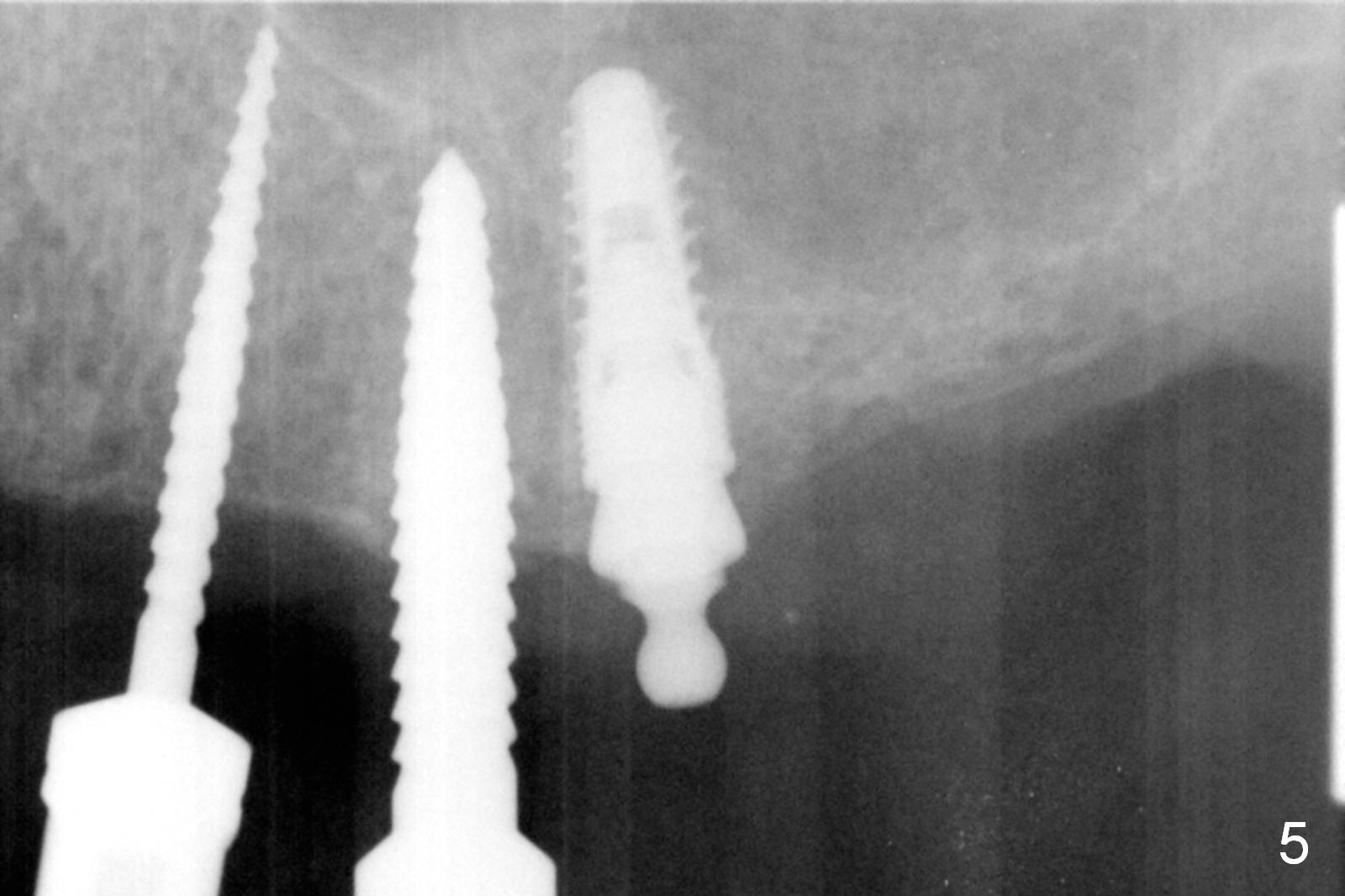
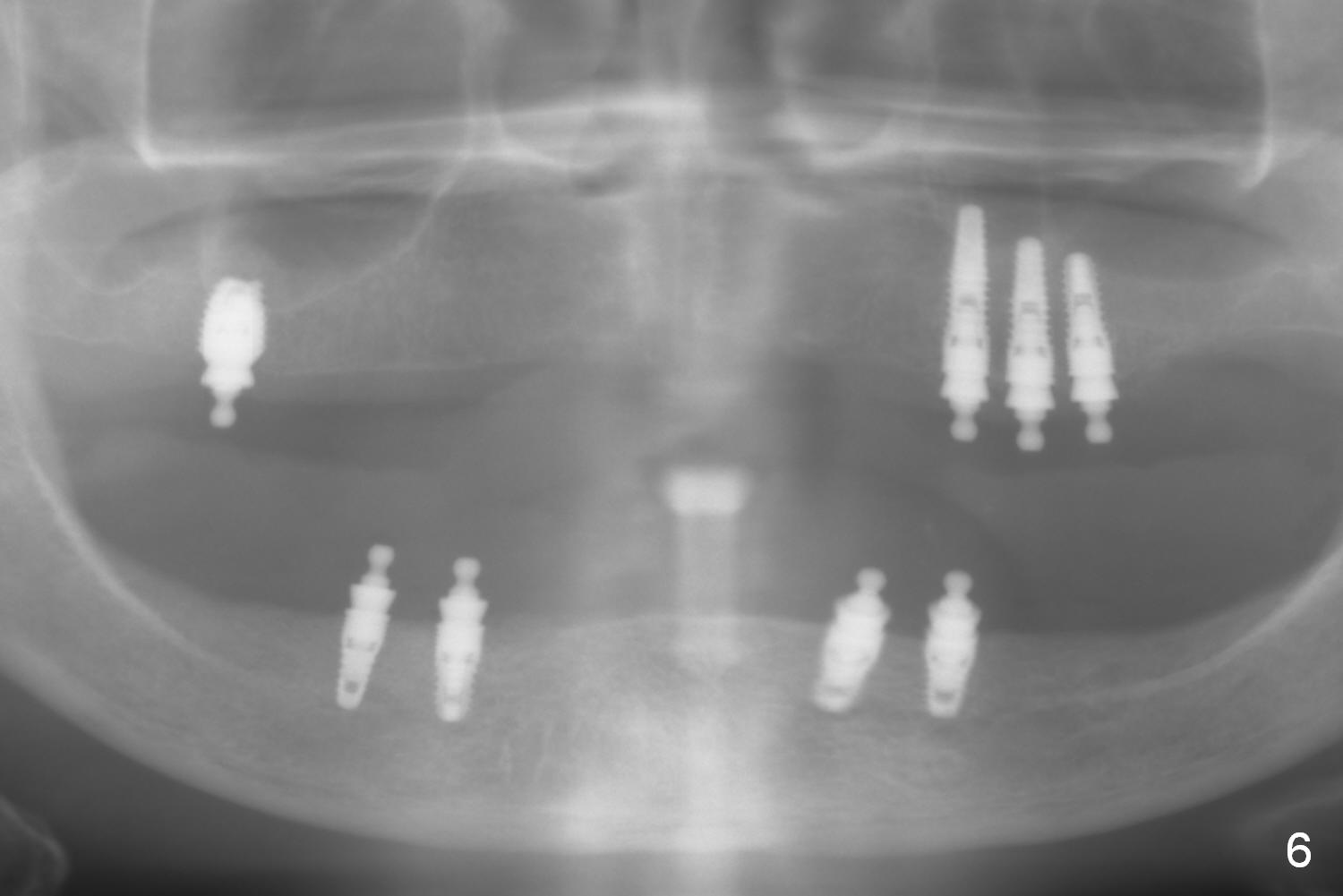
Osteotomies at #11-13 are initiated prior to incision (Fig.2). The ridge at #11 is narrow. The osteotomies are distalized as shown in Fig.3 white circles; the ridge is split with 13 mm wheel saw. Since the buccal plate is softer than the palatal one, ridge split is closer palatally (Fig.3 black line). Osteotomies starts with 1.2 mm initial drill (Fig.4: at #11), followed by bone expander 1 (1.0/1.6 mm; Fig.4: at #12), 2 (1.3/2.3 mm, Fig.4: at #13), and 3 (1.7/3.1 mm, Fig.5: at #12) before placement of small diameter implants (3.8 mm, Fig.5: at #13). The lengths of the implants at #11-13 are 14,12 and 10 mm, respectively (Fig.6). The insertion torque is ~ 35 Ncm. Ball abutments are placed immediately. The upper denture is so retentive that soft reline is not needed. The procedure goes on smoothly because of the soft bone.
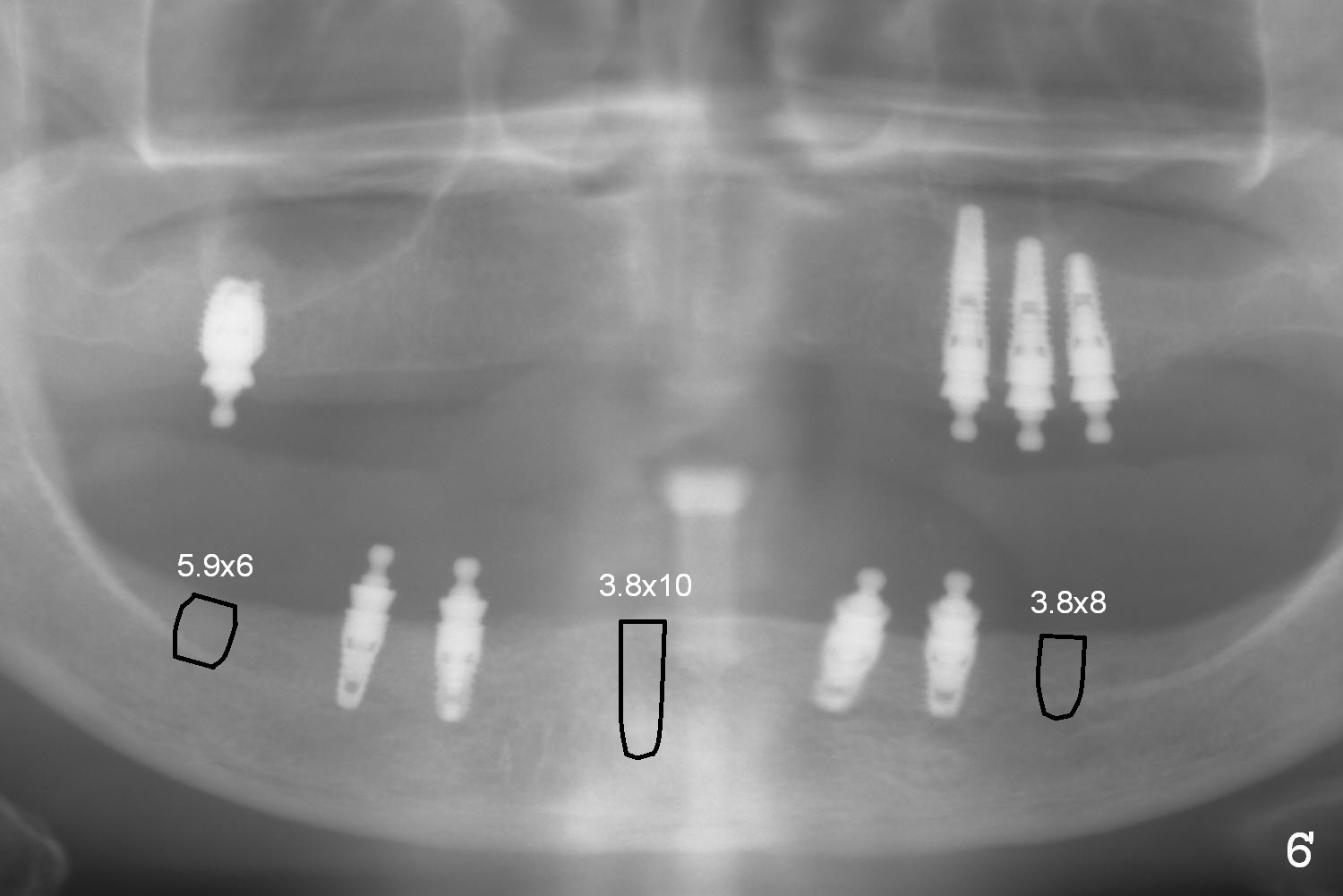
It is 2 weeks post lower implant placement. Since the patient tolerates the previous 2 procedures well, 3 more implants will be scheduled 1-2 weeks (Fig.6' black outlines). Either ball or cemented abutments will be placed, depending upon the time left and primary stability. For the former option, soft reline is expected. For the 2nd one, prefabricated full-mouth crown form should be taken out of the box in the lab.
Return to Upper Arch Implant
Xin Wei, DDS, PhD, MS 1st edition 06/23/2016, last revision 07/13/2016