






|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Soft Bone
The 78-year-old lady returns for #20 residual root extraction; it appears that the tooth has been prepared before (Fig.1 arrowheads). The extraction socket is oval in the opening (Fig.2) with the mesiodistal dimension (arrowheads) larger than the buccolingual one, whereas the typical lower premolar socket is wider buccolingually. No matter what, the osteotomy is placed as lingual as possible.
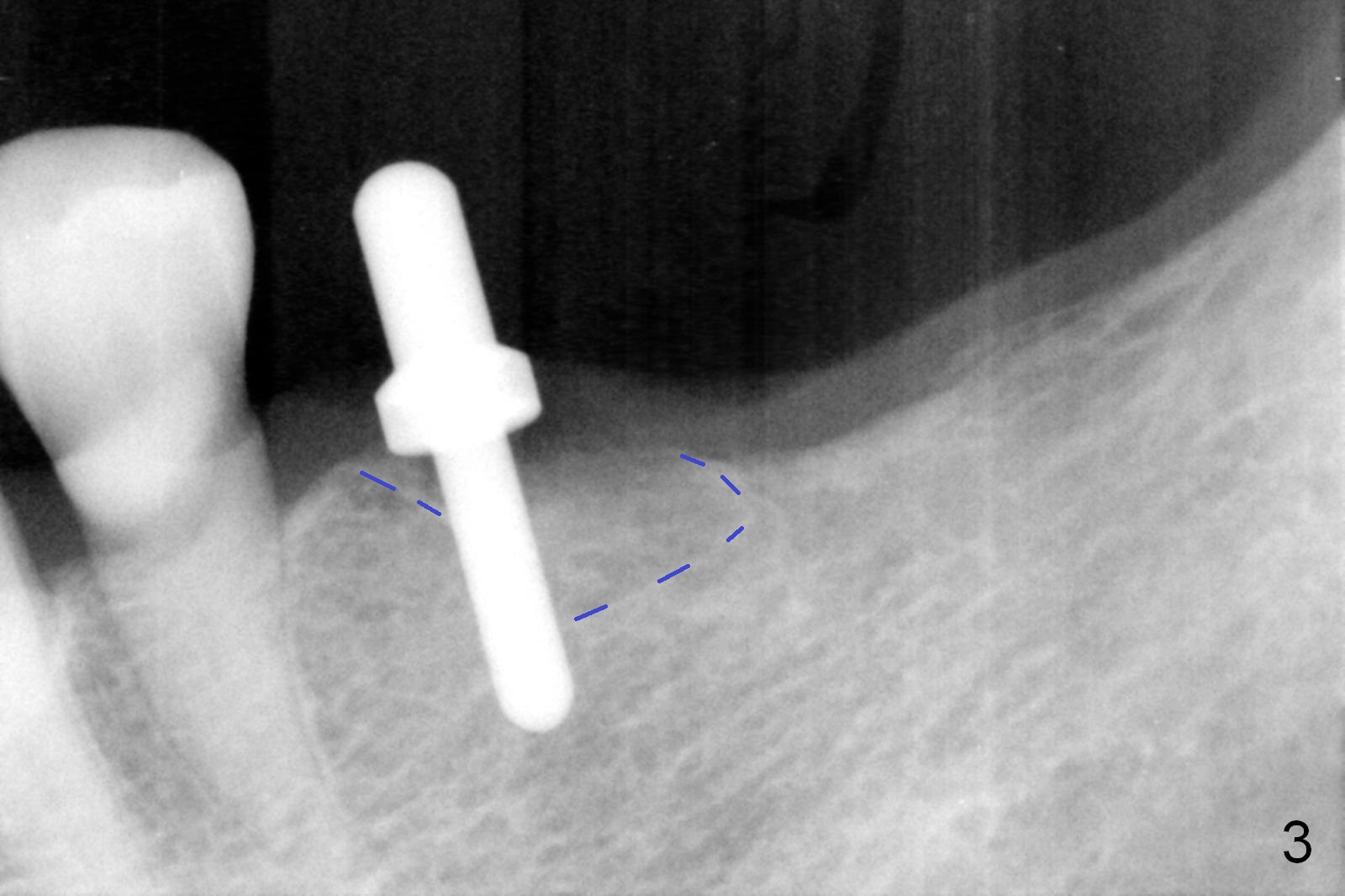
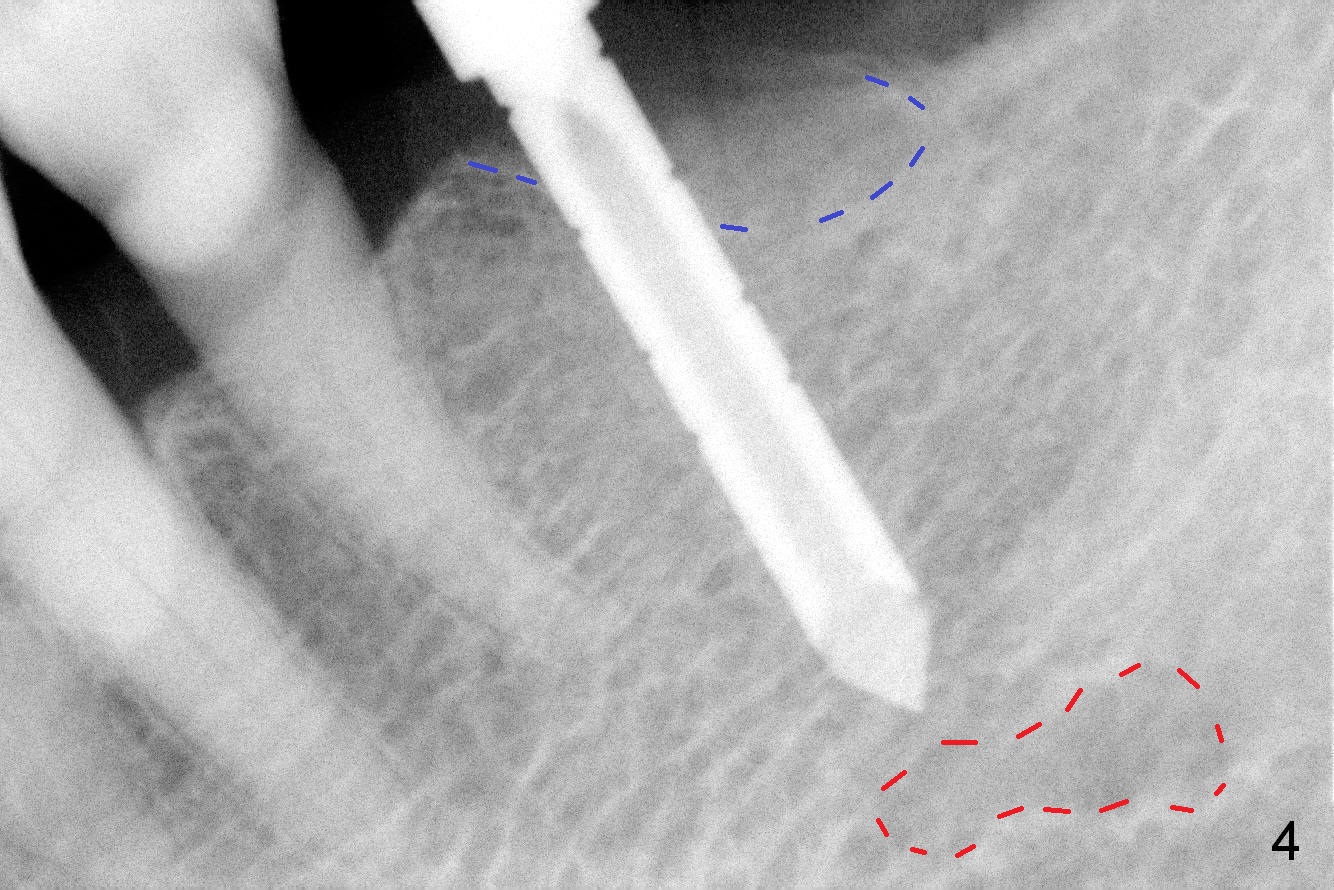
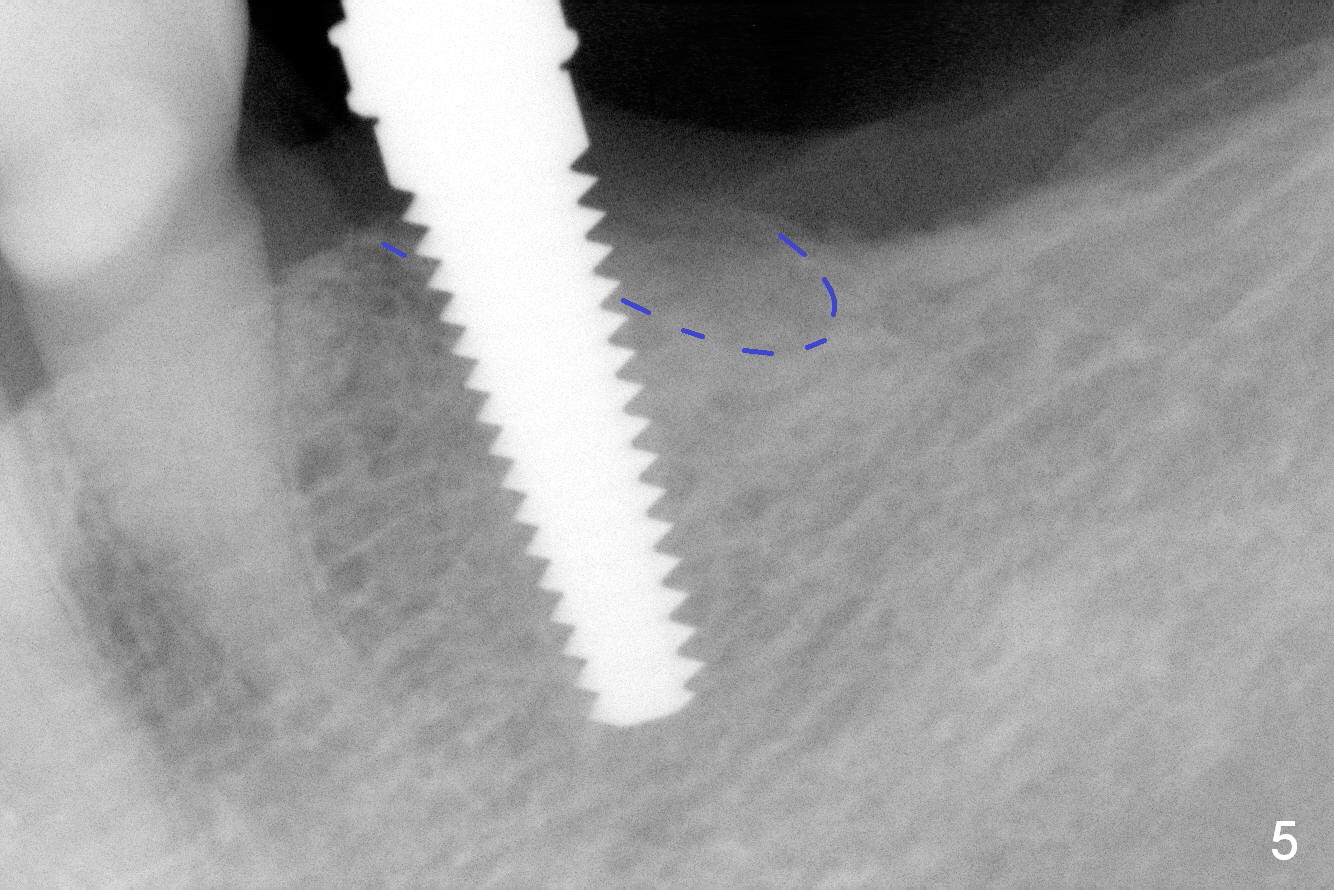
The trajectory of the initial osteotomy is within normal limit (Fig.3 (blue dashed line: socket), but the bone is soft. So the osteotomy is extended 17 mm from the gingival margin (Fig.4, compare to 14 mm as planned); it appears that it is close to the assumptive Mental Loop (red dashed line). For safety, further osteotomy is confined to 14 mm (Fig.5 4.5 mm tap). The implant is 4.5x14 mm with insertion torque <35 Ncm. The distal gap is so small that it is impossible to place collagen membrane. It is difficult to place bone graft. An immediate provisional is placed to close the socket. Perio dressing is also placed. There is no symptom of nerve damage postop.
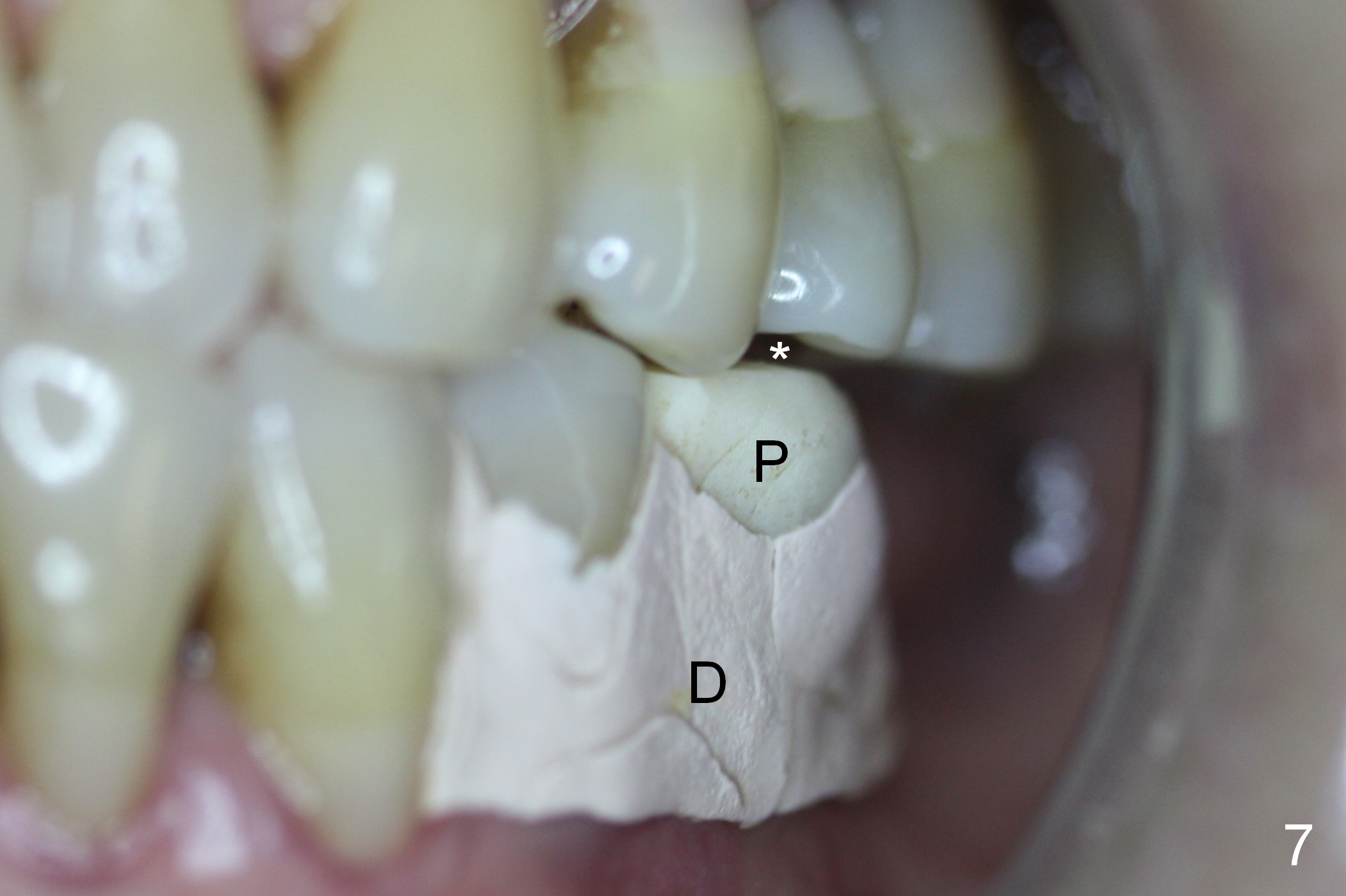
The patient returns asymptomatic 8 days postop. She prefers to have the perio dressing (Fig.7 D) removed (Fig.8) for comfort. The provisional was fabricated with the wider mesiodistal dimension to cover the socket (Fig.2). Since the socket has basically closed except mesial (Fig.9 *), the provisional is modified so that the mesiodistal dimension is within normal limit (Fig.10). The provisional is relined without reprep and then re-cemented.
Three months postop, the implant and the immediate provisional are stable; the original socket appears to disappear (Fig.11). What should be done at the sites of #18 and 19, considering the narrow ridge (Fig.2,6) and soft bone? One or 2 implants?
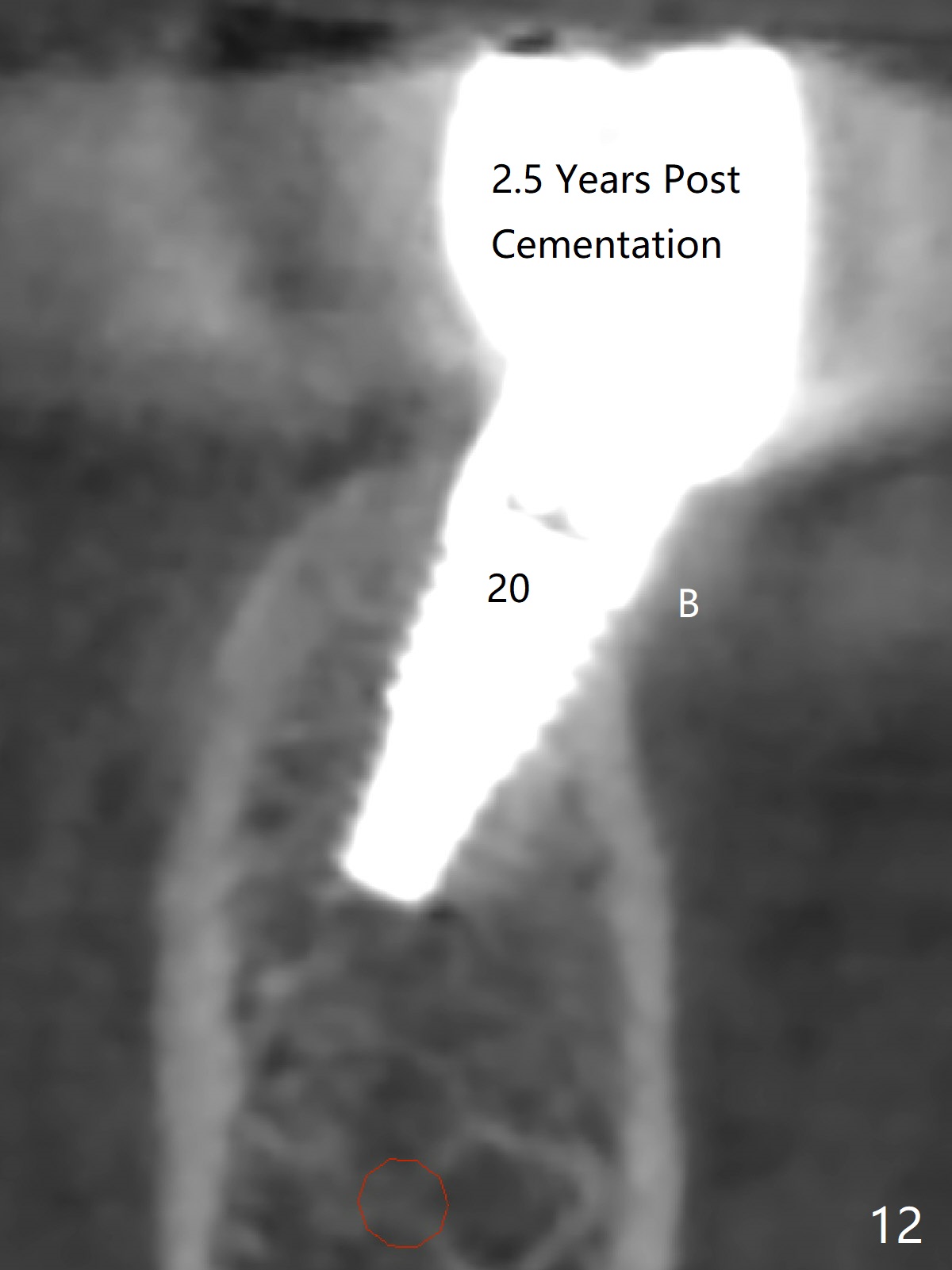
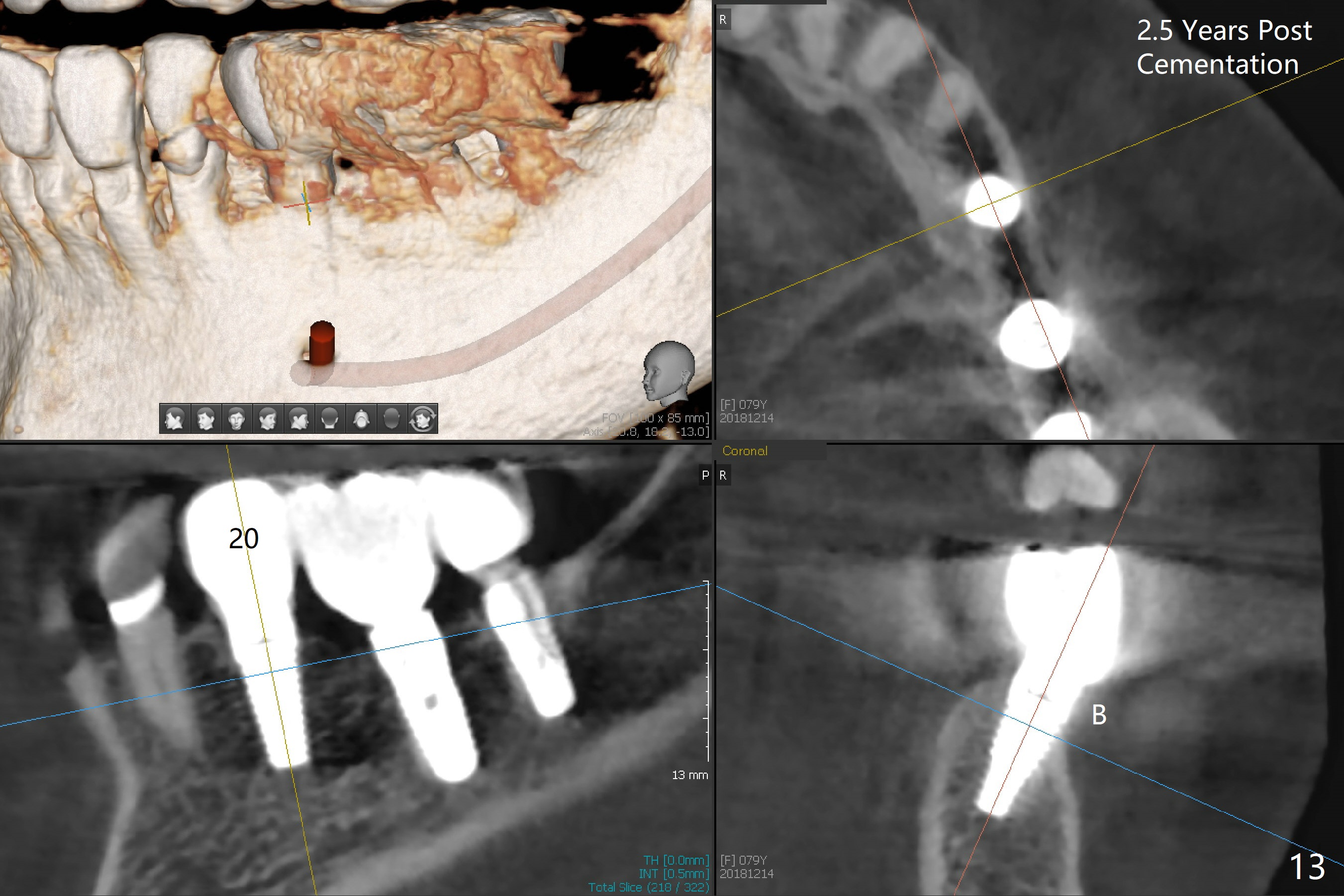
CT taken 2.5 years post cementation does not show buccal (B) or lingual bone loss at #20 (Fig.12-13).
Return to Lower Bicuspid
Immediate Implant,
Posterior Immediate Provisional,
18/19
Xin Wei, DDS, PhD, MS 1st edition 04/30/2015, last revision 12/27/2018