

|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
Molar Immediate Implant Trajectory is Controllable
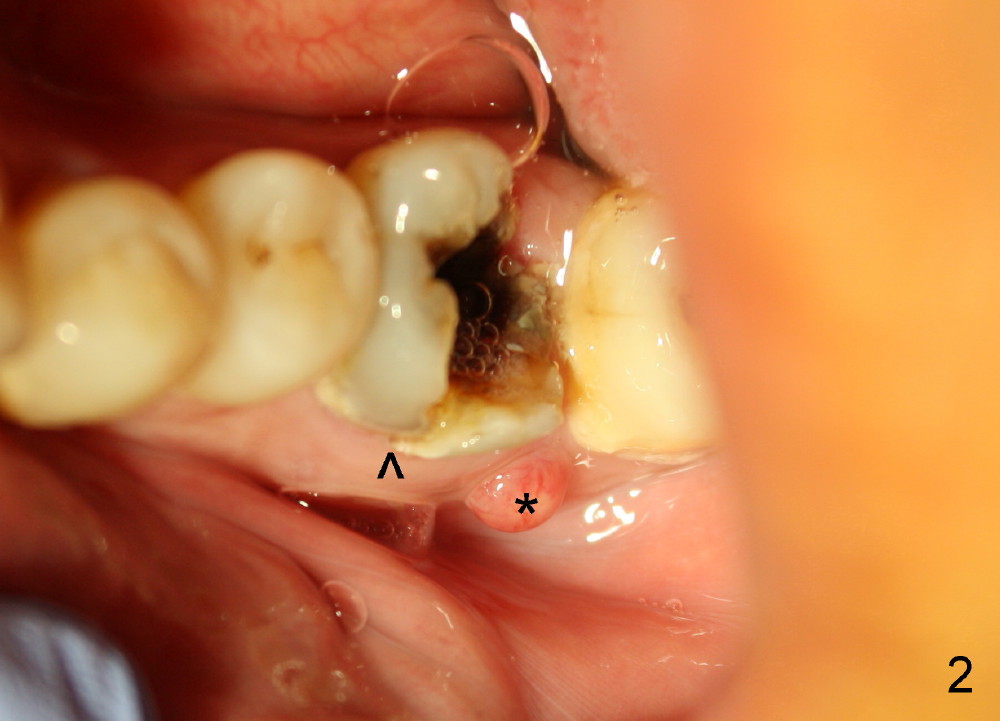
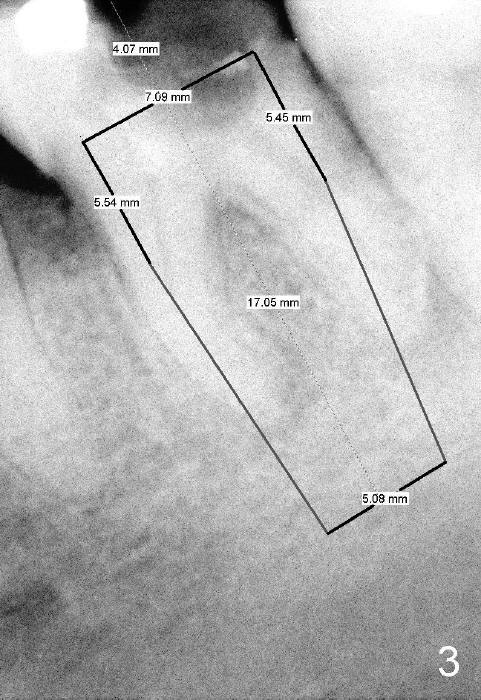
The lower left 1st molar of a 56-year-old phobic man is nonsalvageable (Fig.1,2) and is planned to be replaced with a 7x17 mm implant (Fig.3). The tooth is extracted with sectioning. The socket is thoroughly debrided and soaked with Clindamycin. Osteotomy is created in the middle of the septum with osteotomes and 2 mm pilot drill and 2.5-4 mm reamers. It appears that 1-2 mm new bone has been incorporated into the osteotomy.
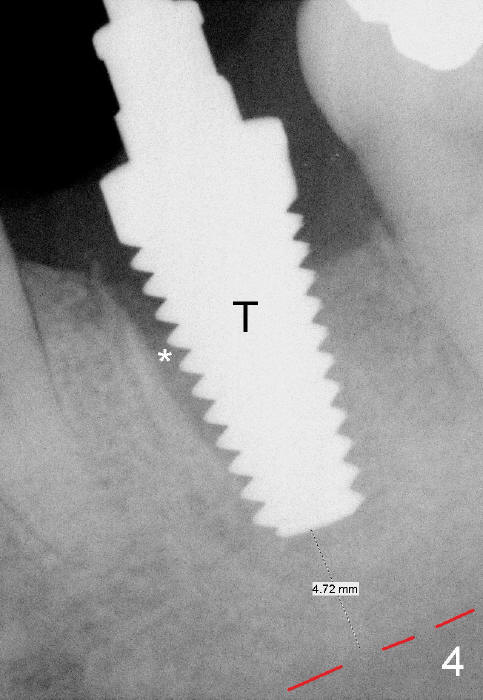
Fig.4 shows 7x17 mm tap in place (with some stability); there is 4-5 mm of bone between the bottom of the osteotomy and the inferior alveolar canal. Probably due to pre-existing infection (Fig.2 <), pain is not controlled completely, even after inferior alveolar block is administered. In addition, there is constant hemorrhage from the bottom of the osteotomy.
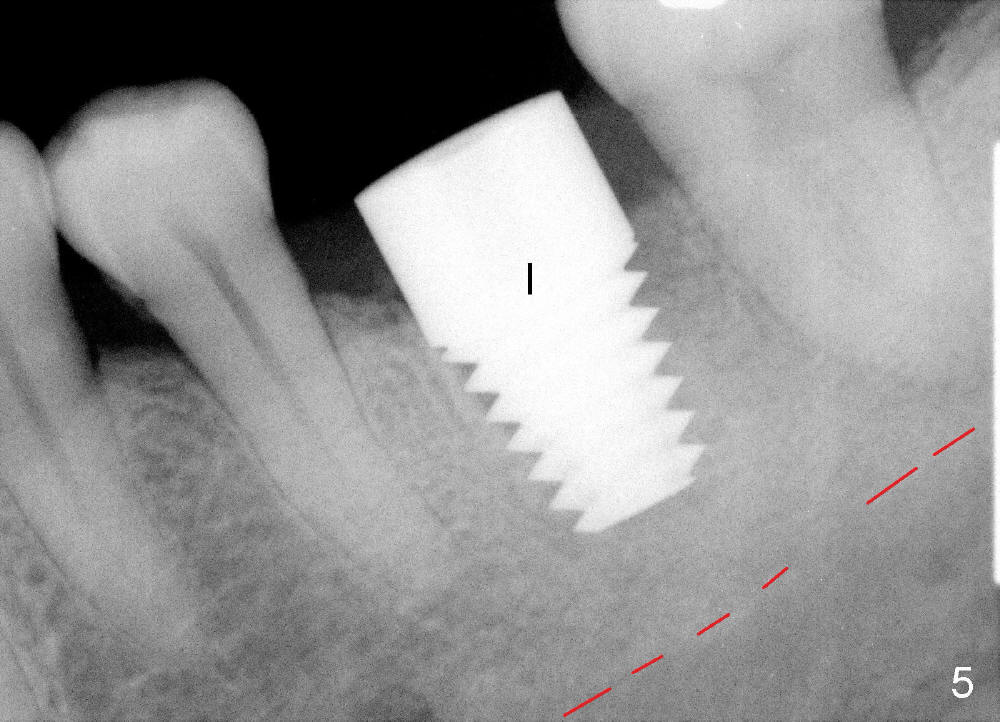
Deeper osteotomy is not pursued. Instead, a larger implant is placed (8x14 mm), resulting in almost obliterating the socket (Fig.5) with insertion torque of more than 60 Ncm. The trajectory is favorable to restorativon. With practice, the molar immediate implant trajectory is controllable.
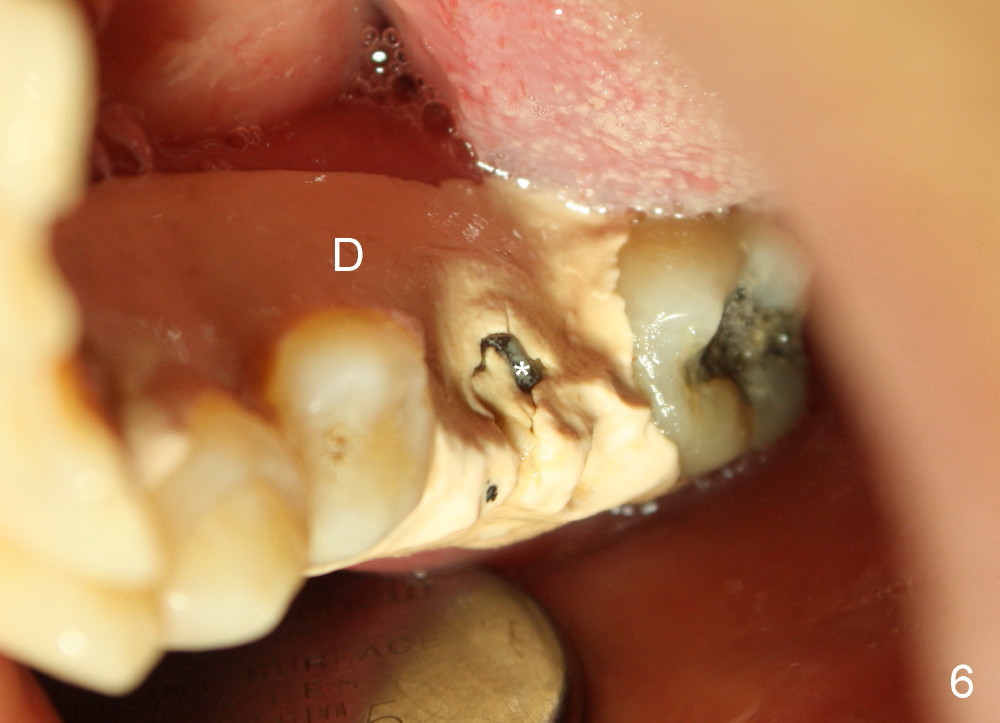
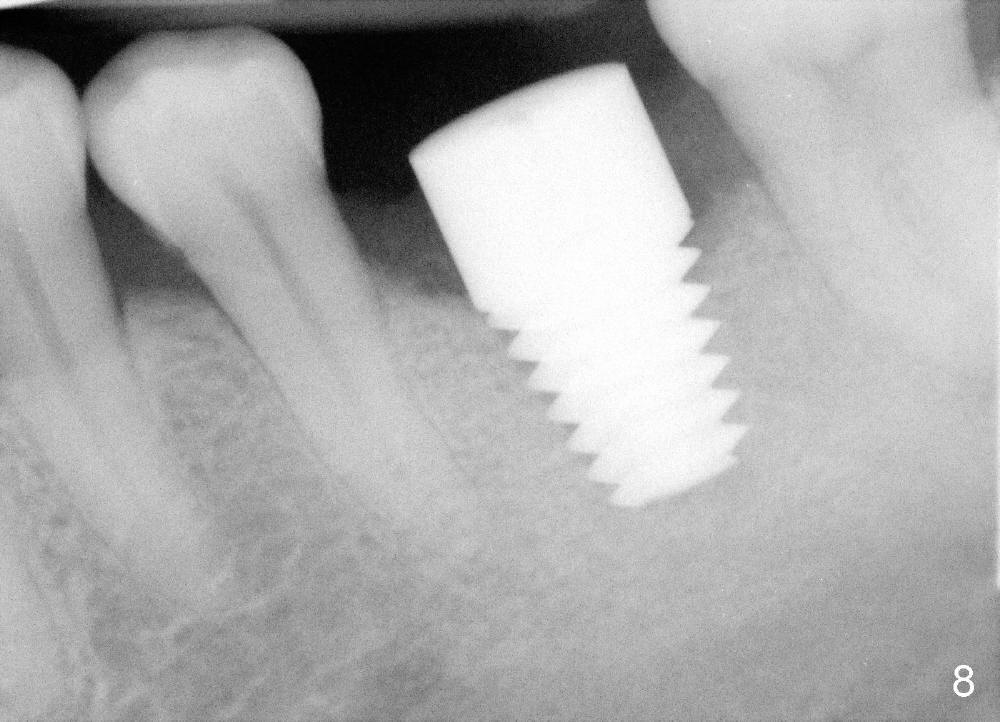
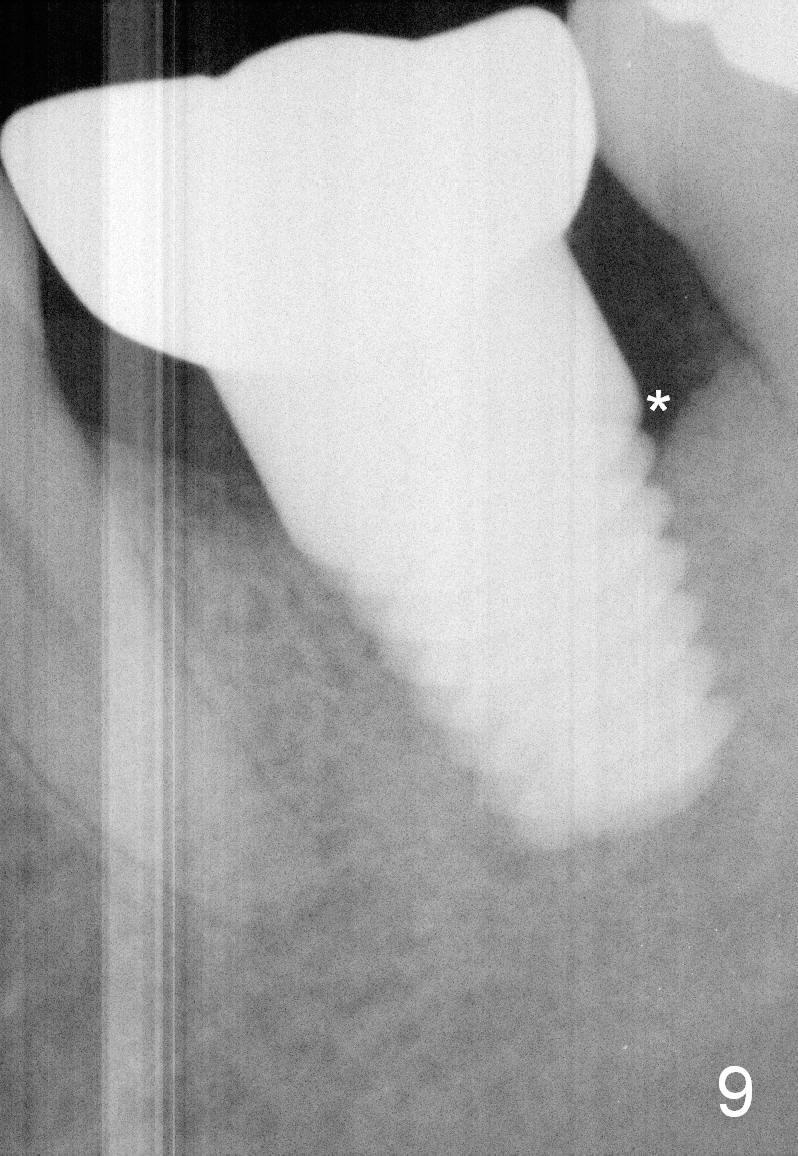
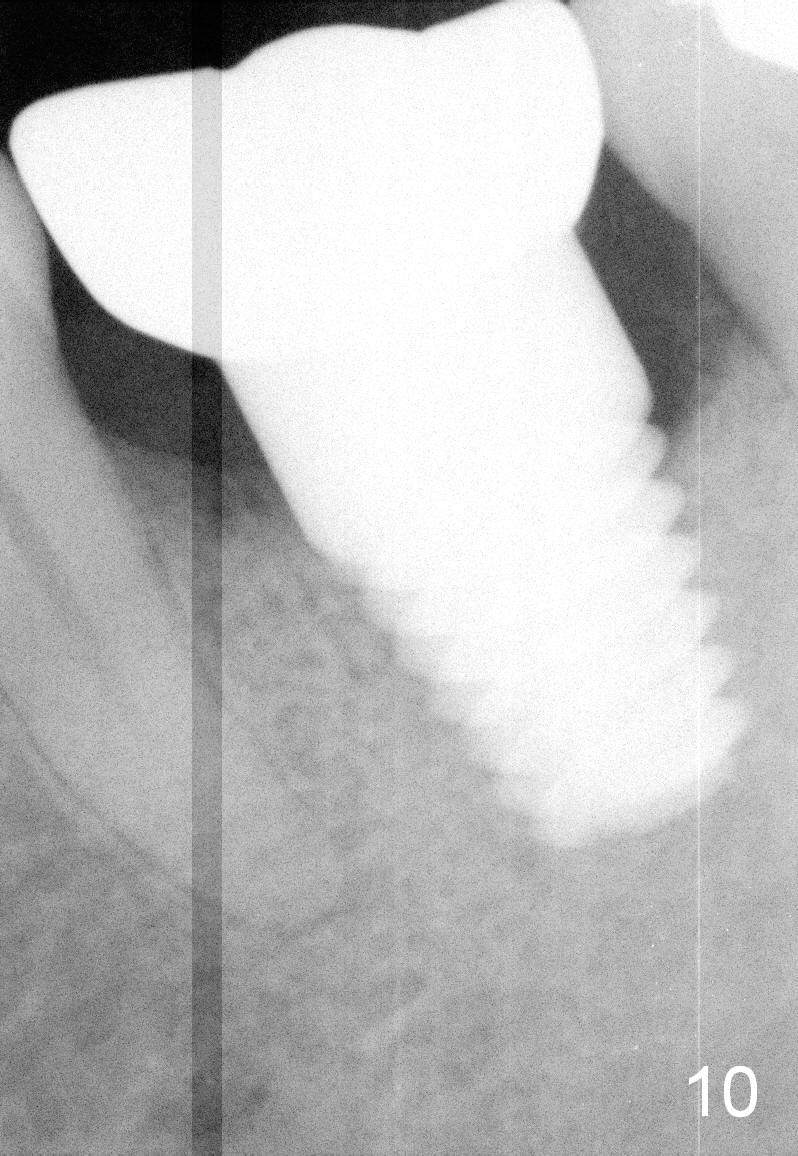
With insertion of the abutment (Fig.6 *), perio dressing (D) is able to stay in place 8 days postop. When the patient returns for follow up 22 days postop, the implant (Fig.7 I) is surrounded by the healthy gingiva. The wound healing is related to protection of the perio dressing, which was kept in place by the abutment (A). The bone appears to have grown into implant threads 3.5 months postop (Fig.8). It appears that the distal crestal bone continues to be resorbed slowly 4 months post cementation (Fig.9,10 *, as compared to Fig.5,8), although there is no gingival erythema. The patient complains of tight contact between #18 and 19. The resorption may be less with a smaller implant.
Return to Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 07/04/2014, last revision 04/11/2015