%20abutment.jpg)

|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
|
|
|
|
|
|
|
|
||||
Flapless and Dual Osteotomy Approaches
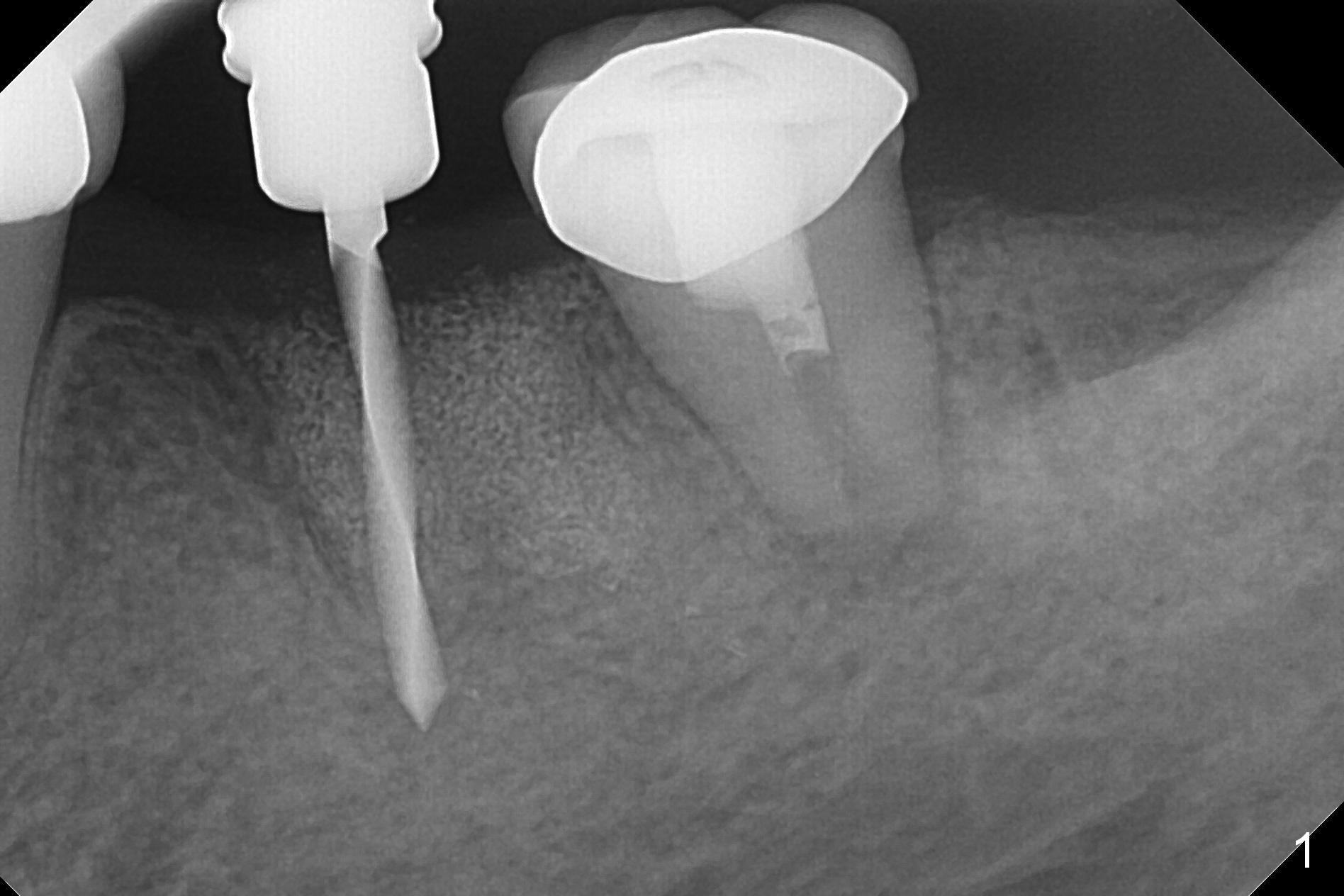
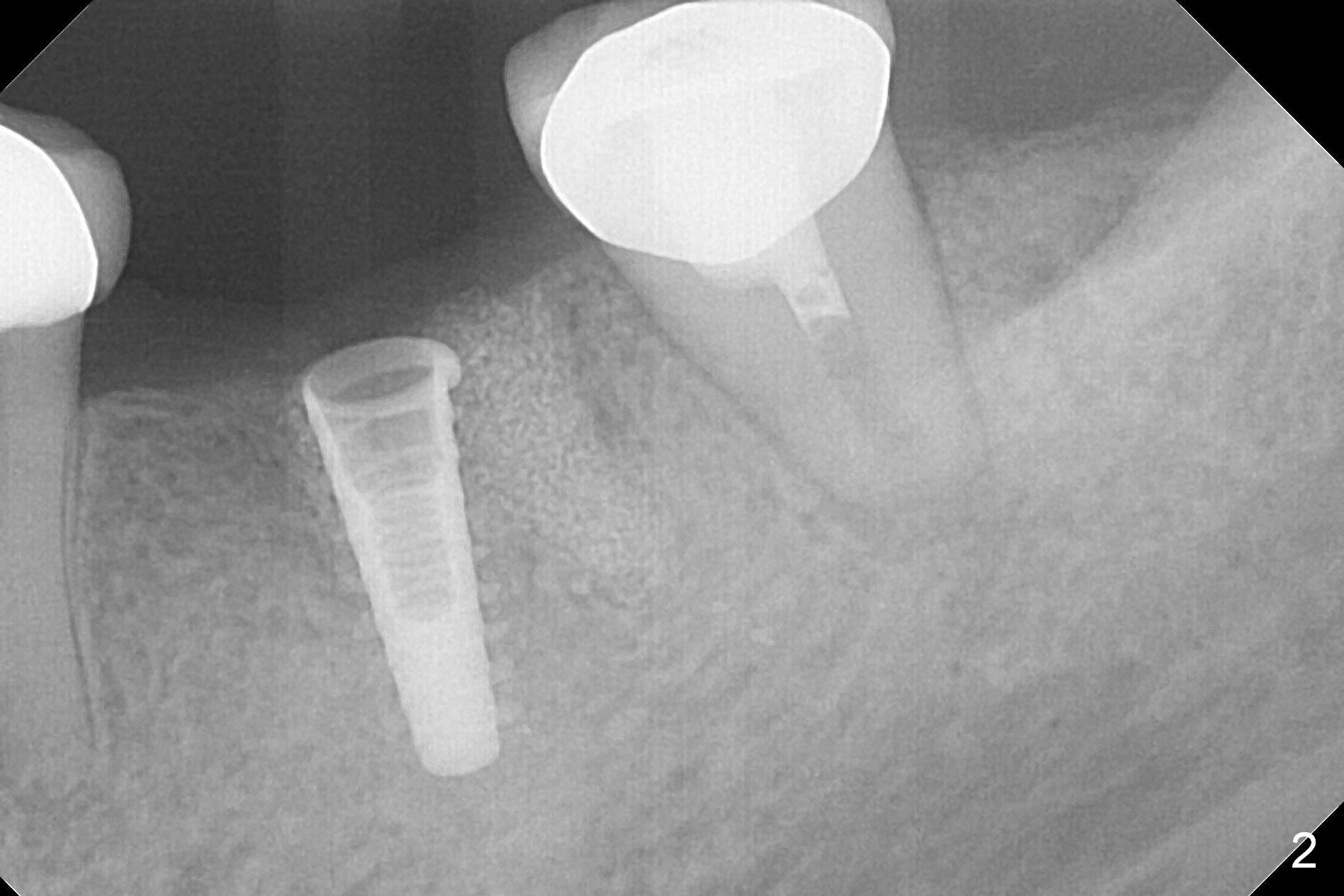
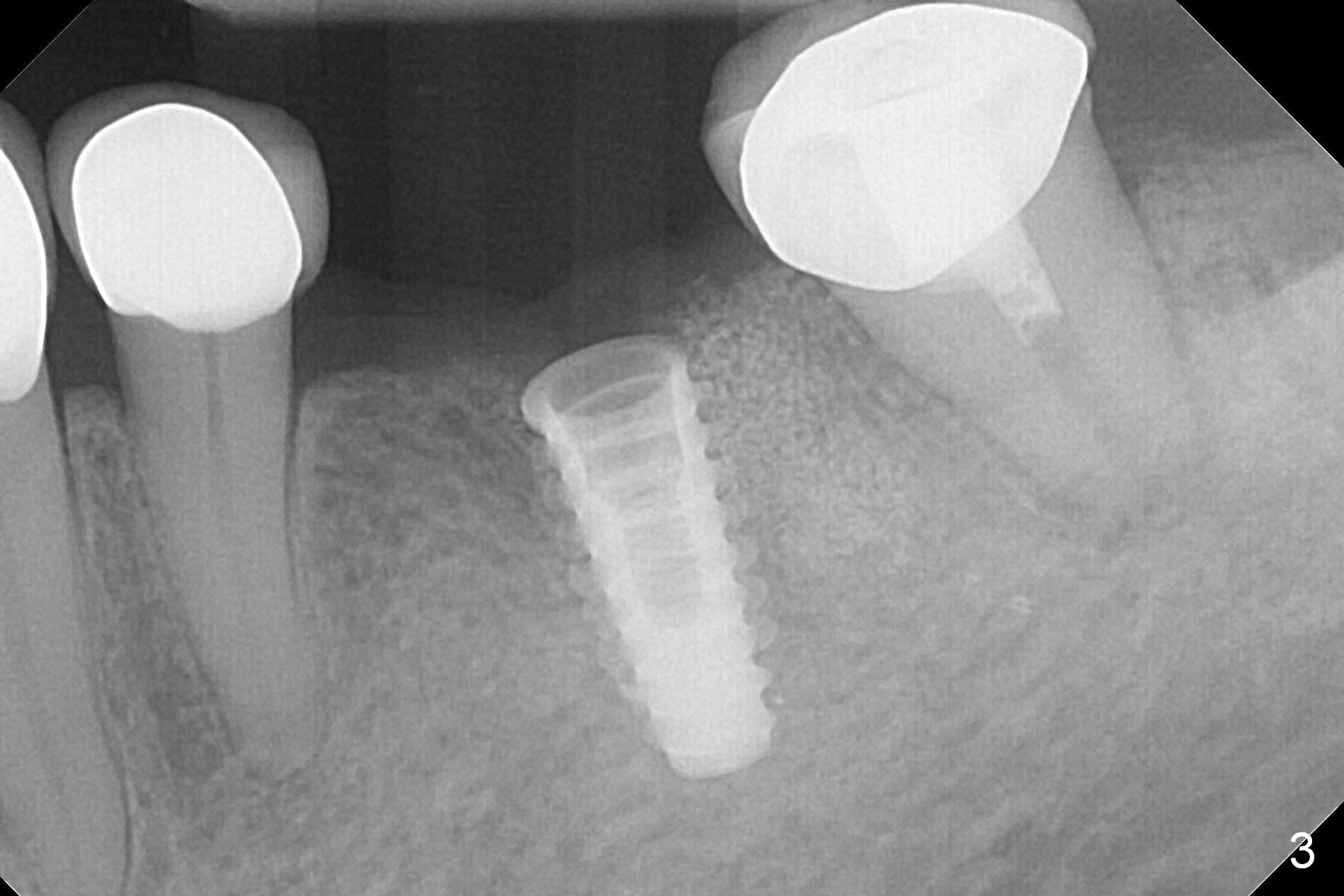
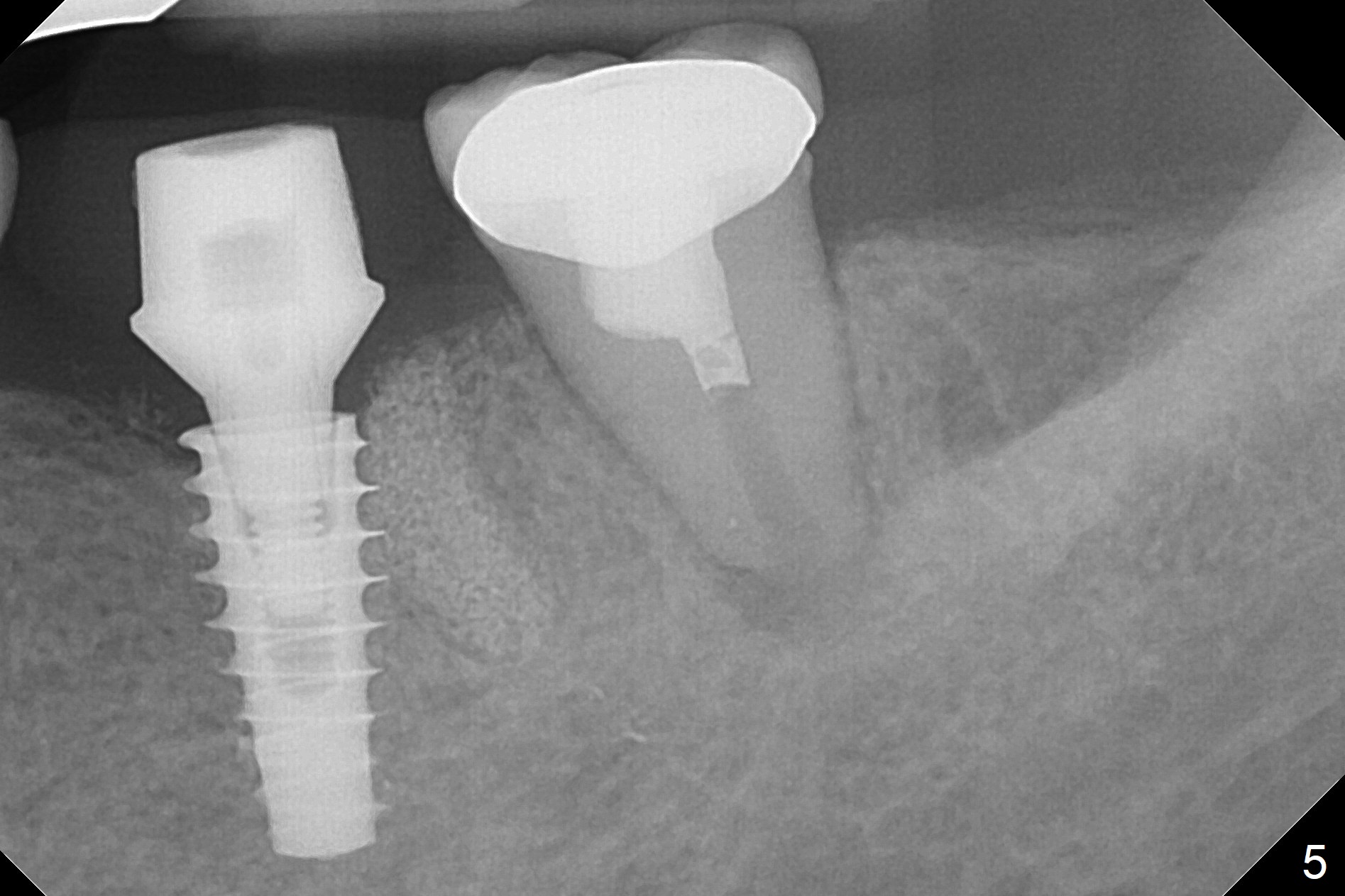
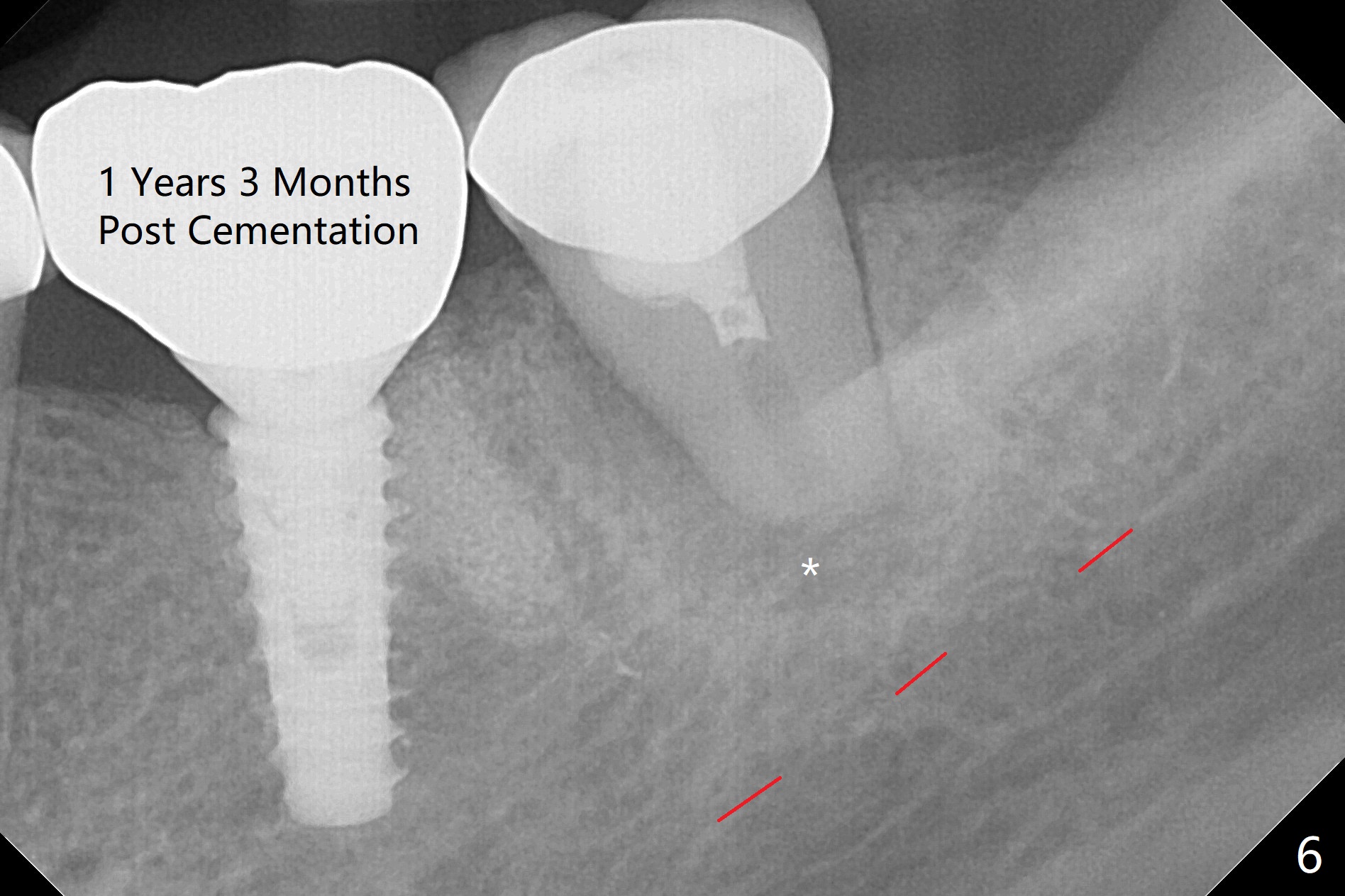
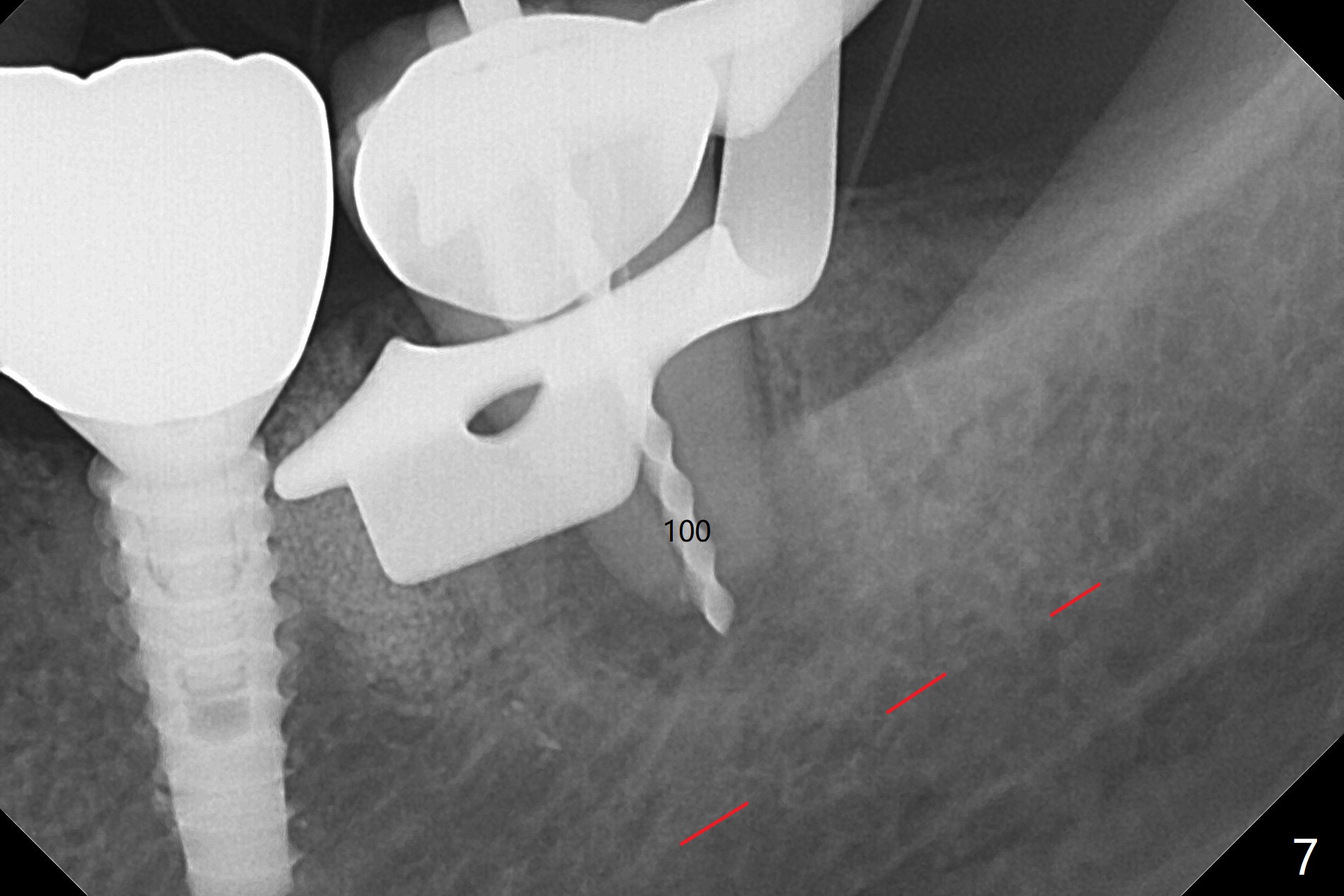
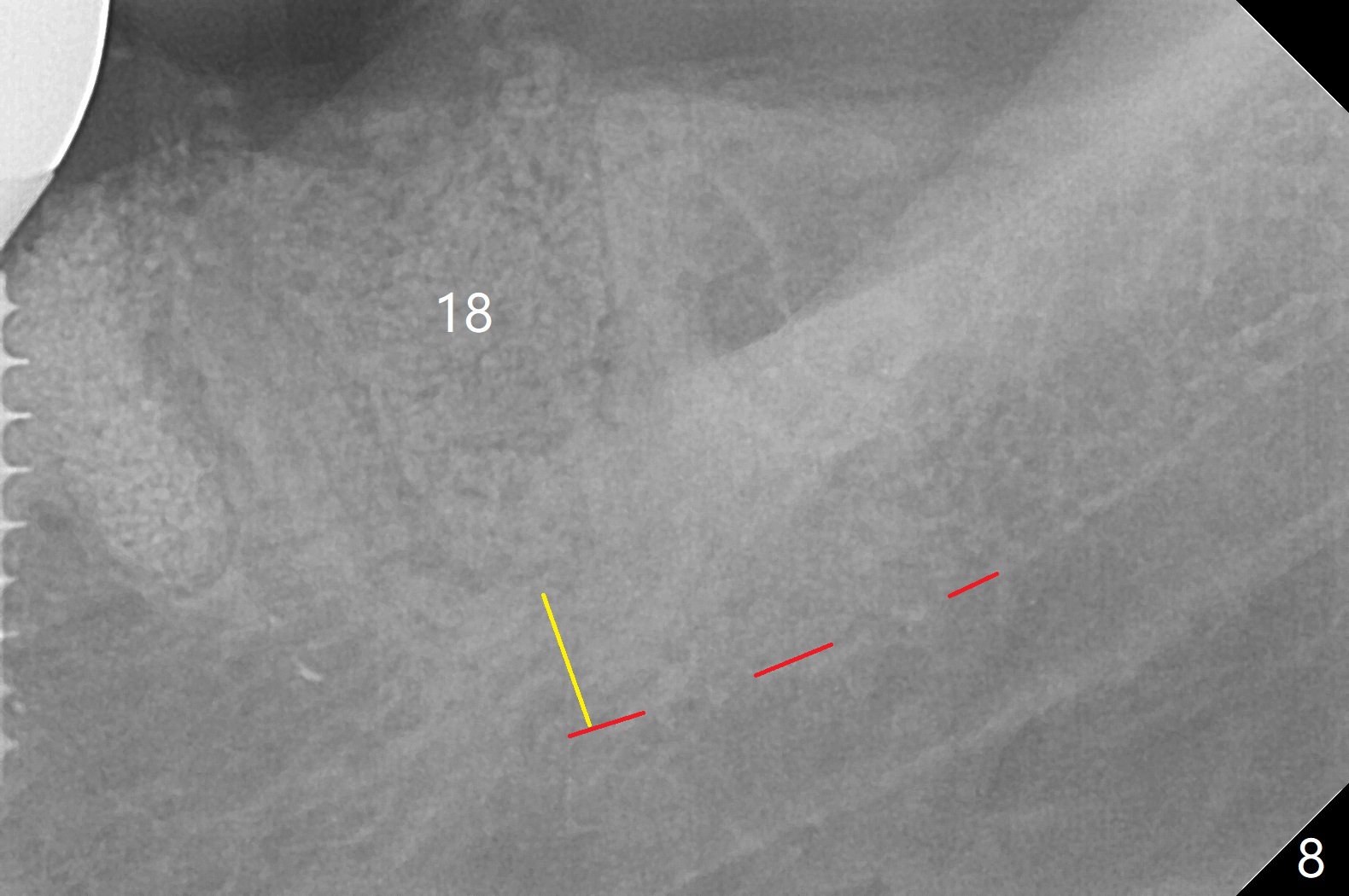
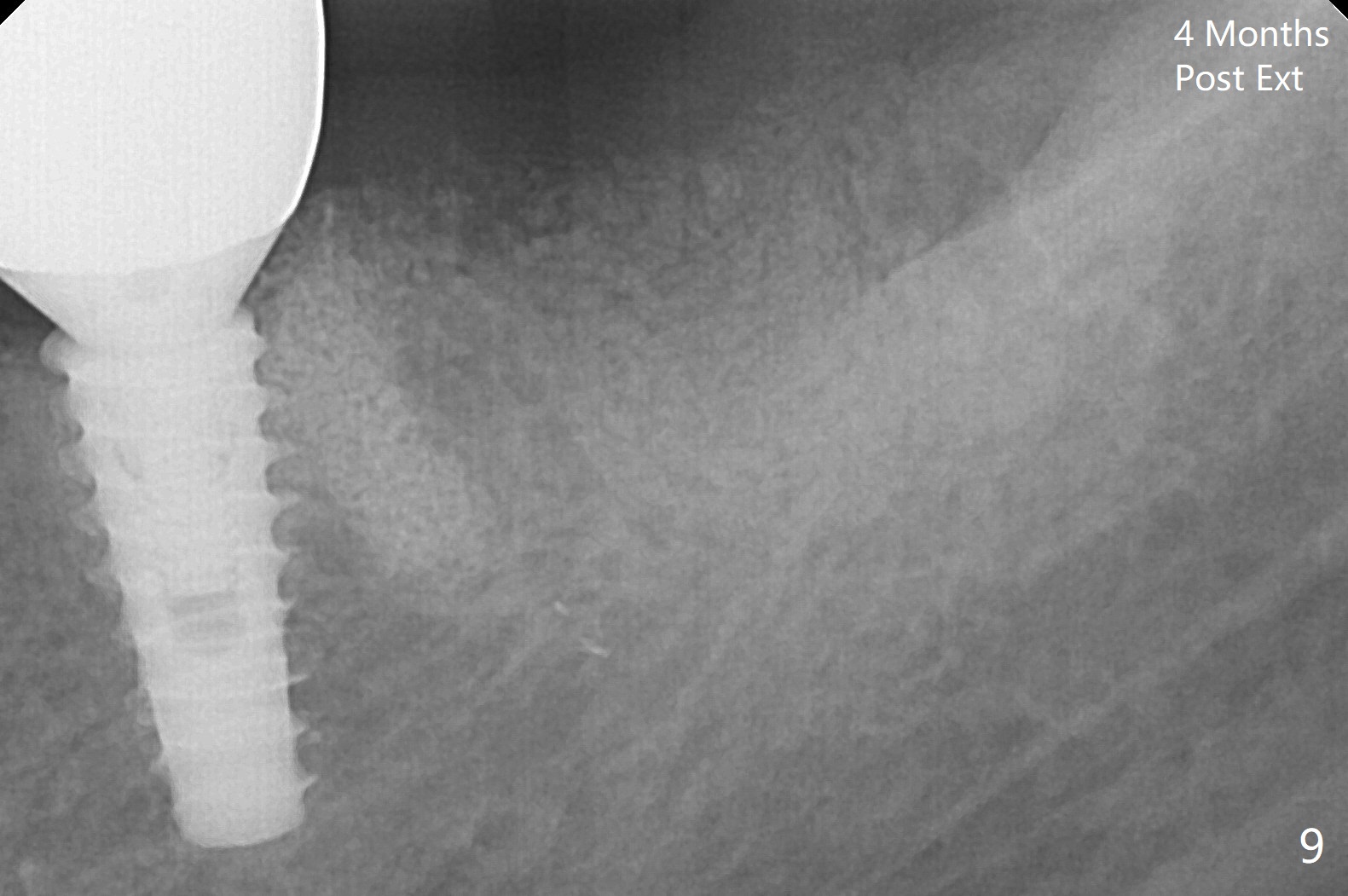
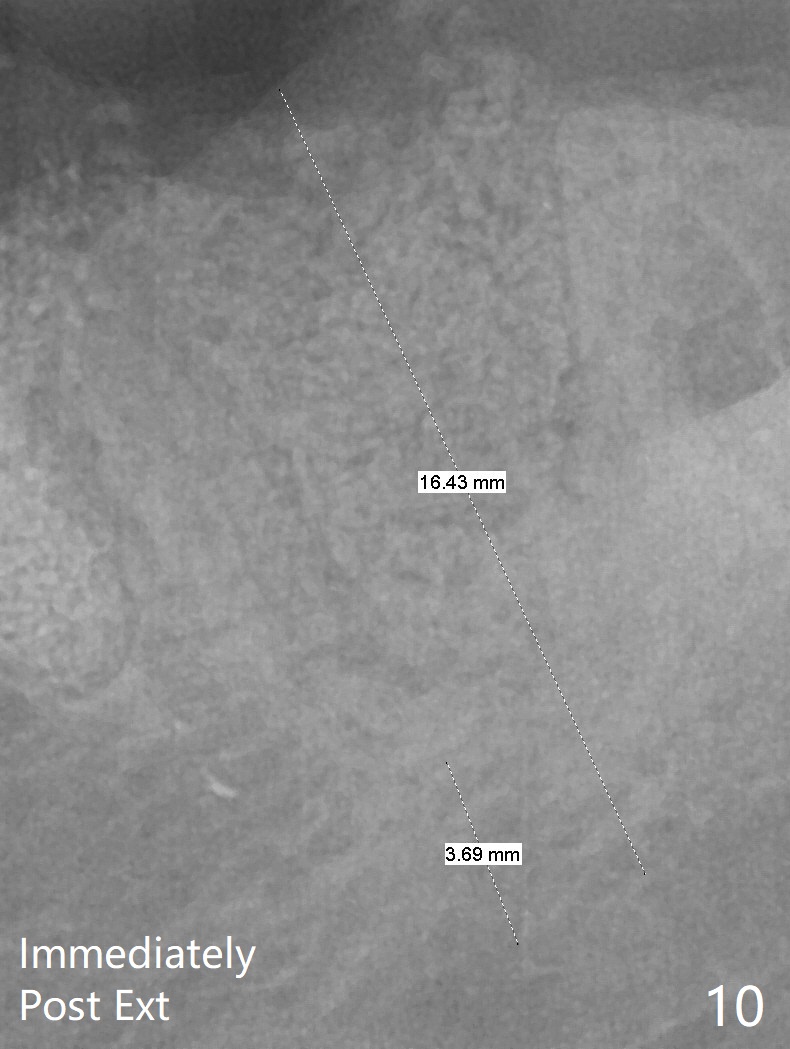
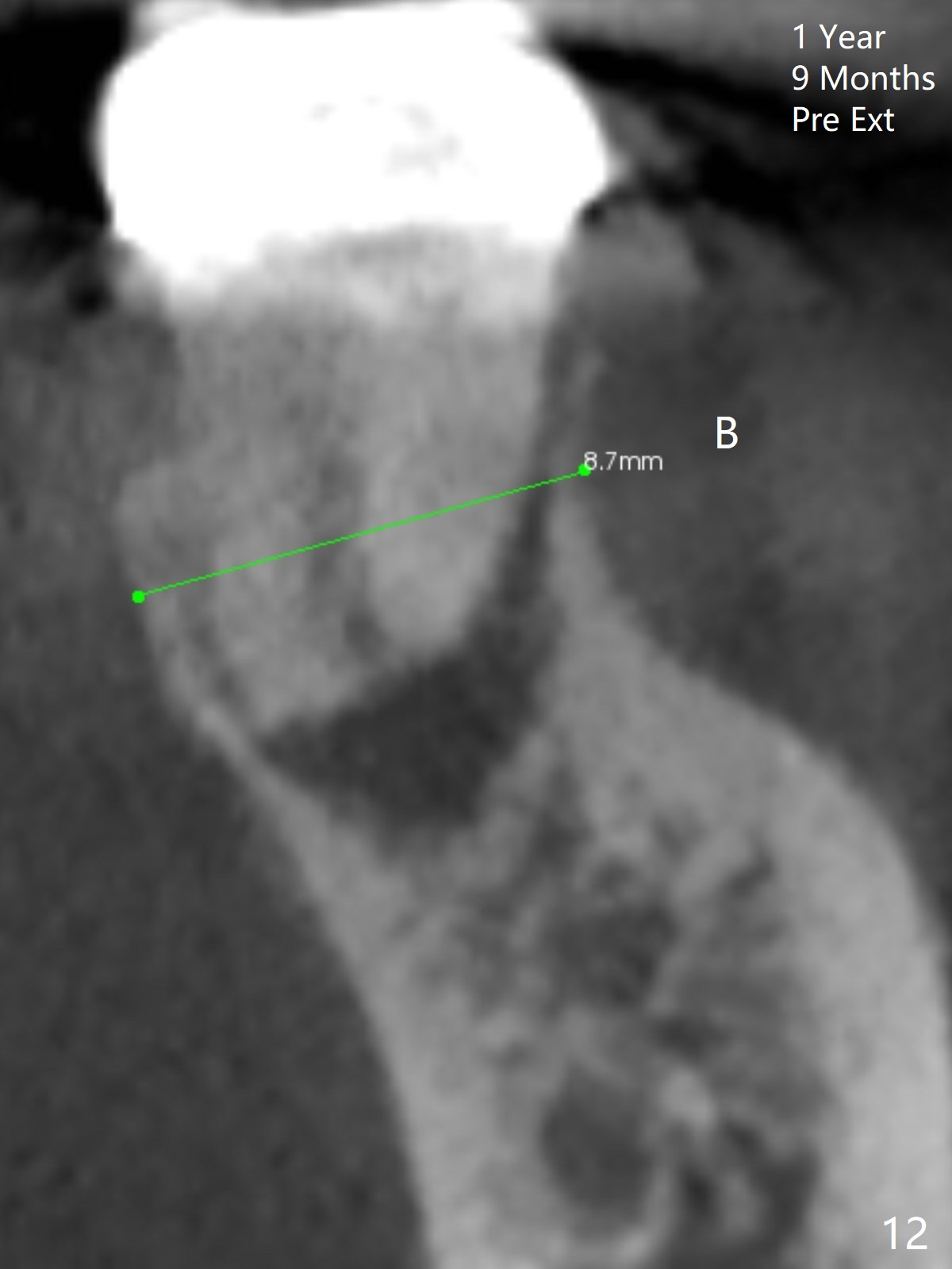
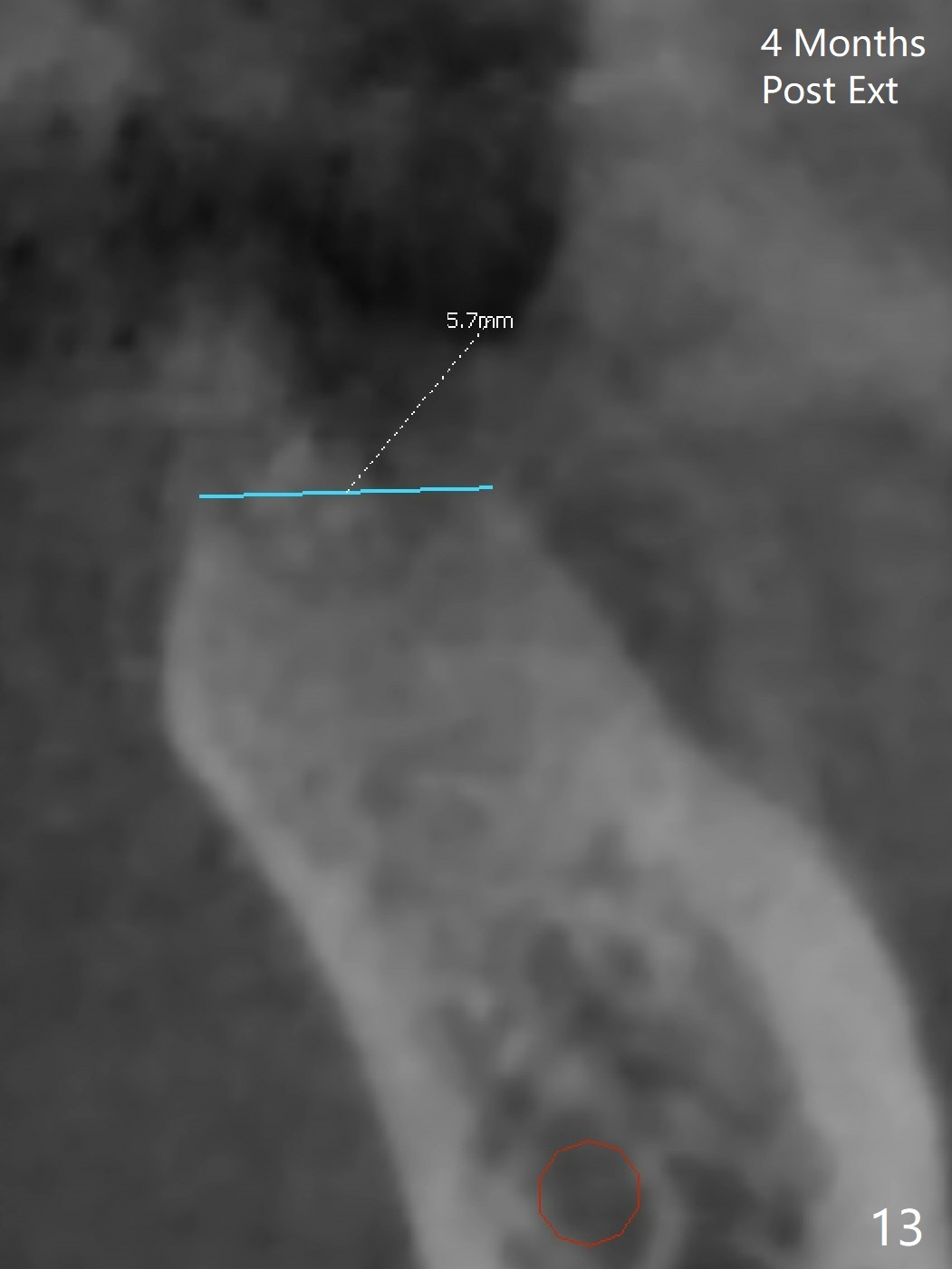
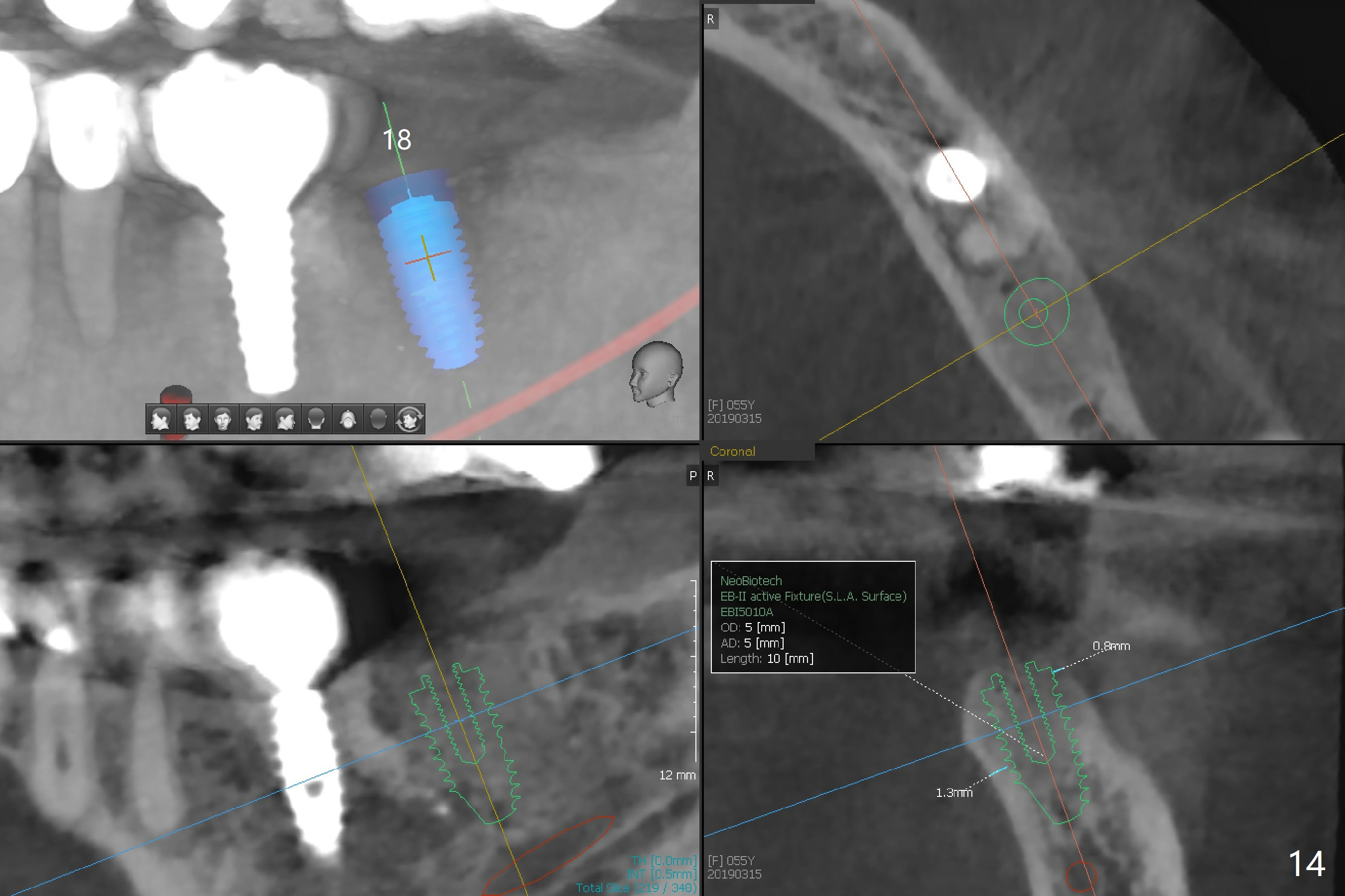
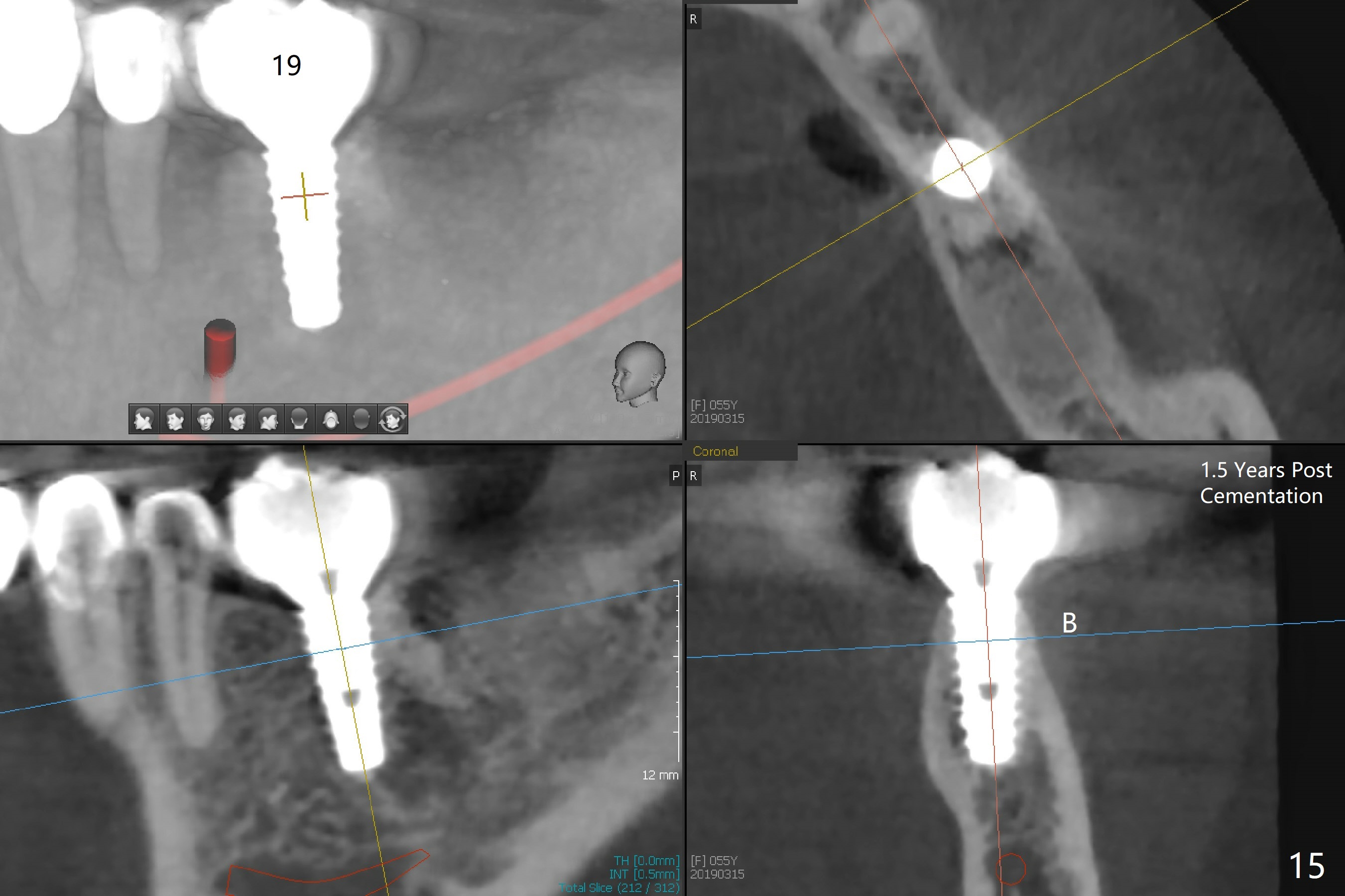
After making a 10 mm incision at the site of #19, #15c blade is used as an osteotome to start bone expansion, followed by Magic Split and Magic Expander (ME, 3 mm in diameter). The depth is approximately the bottom of the mesial socket. The osteotomy beyond the socket has to be done with 1.6 mm pilot drill (Fig.1) in combination of ME. Following ME 4.3 mm and Magic Drill (MD) 3.8 mm for 15 mm (gingival level), a 4.5x11 mm dummy implant is placed with 50 Ncm (Fig.3); the implant looks narrow for the edentulous space. After ME 4.8, MD 4.3 for 13 mm and Final Drill for 15 mm, a 5x11 mm IBS is inserted with >50 Ncm (Fig.3). With 2 more turns of the implant, a 6.5x4(2) mm abutment is placed (Fig.4). Periodontal dressing is applied around the abutment for additional retention. A provisional is fabricated 3 weeks postop. The provisional and abutment are loose 4 months postop (Fig.5). After retightening the abutment, impression is taken for final restoration. There is no bone loss 1 year 3 months post cementation (Fig.6). After use of #100 file (Fig.7), the canal is debrided with #140 file with 1.5 mm shorter in working length with placement of Calcium Hydroxide paste. Pain gets worse post RCT retreatment. There is limited native bone for primary stability when an immediate implant is placed (red dashed line: the superior border of the Inferior Alveolar Canal). Prepare IS regular and extra wide kits and tissue-level implants (>5 mm). Socket preservation may be done instead. If the socket is large and the vein is not so small, prepare PRF. In fact blood drawing fails. When the tooth is extracted, it is sensitive to remove granulation tissue. Socket preservation is done with Vanilla graft at #18 (Fig.8); there is ~3.5 mm bone between the bottom of the single socket and the Inferior Alveolar Canal (red dashed line). The socket at #18 seems to have healed 4 months post extraction (Fig.19), but the bone height appears to have been reduced (compare Fig.10,11). The buccolingual width is also decreased (Fig.12,13). A 4.5 or 5.0x10 mm implant is appropriate for the site (Fig.14). There is no bone loss at #19 (which may be associated with the bone expansion) 1.5 years post cementation (Fig.15). Therefore the osteotomy at #18 will be assisted with bone expanders after 2.2 mm drill.
Return to Lower Molar Immediate Implant #30 18
Xin Wei, DDS, PhD, MS 1st edition 03/17/2017, last revision 04/13/2019