

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hemisection and Immediate Implant
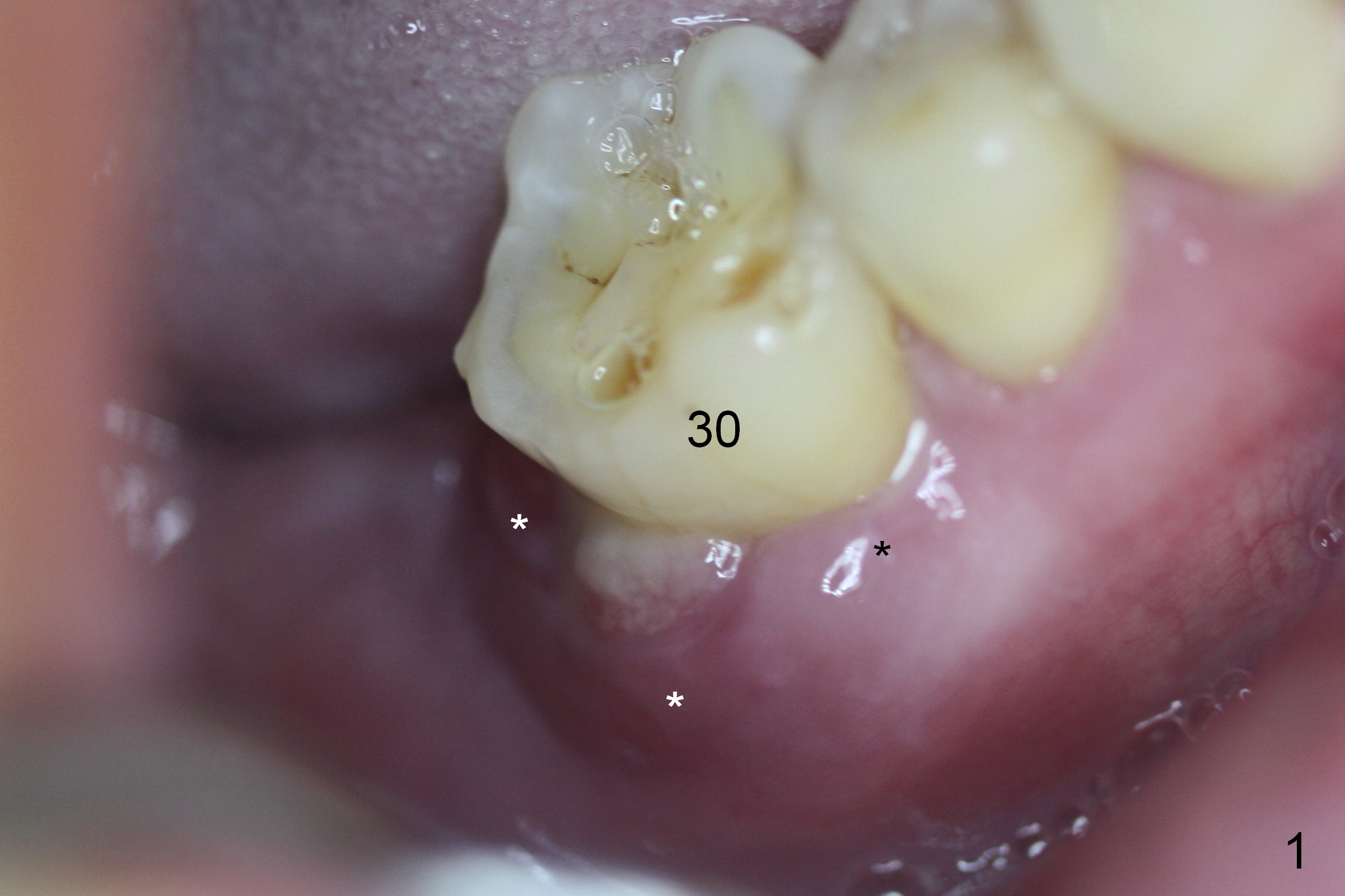
When the patient returns for #30 extraction and immediate implant and #31 delayed implant, there is severe distobuccal swelling and erythema at #30 (Fig.1 *). The buccal and distobuccal (DB) pockets are deep whereas the mesiobuccal one is within normal limit. The tooth has unnoticeable mobility.
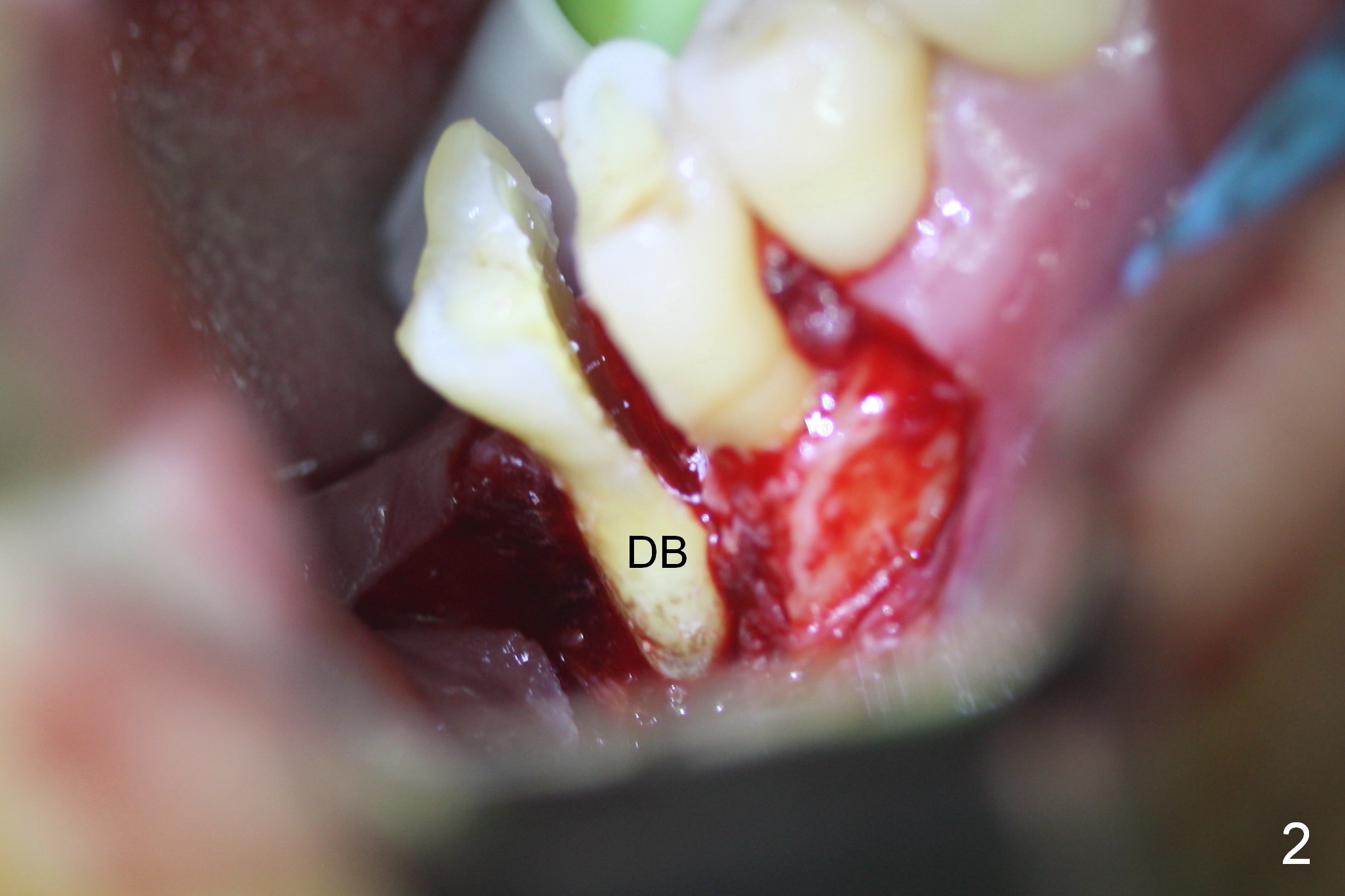
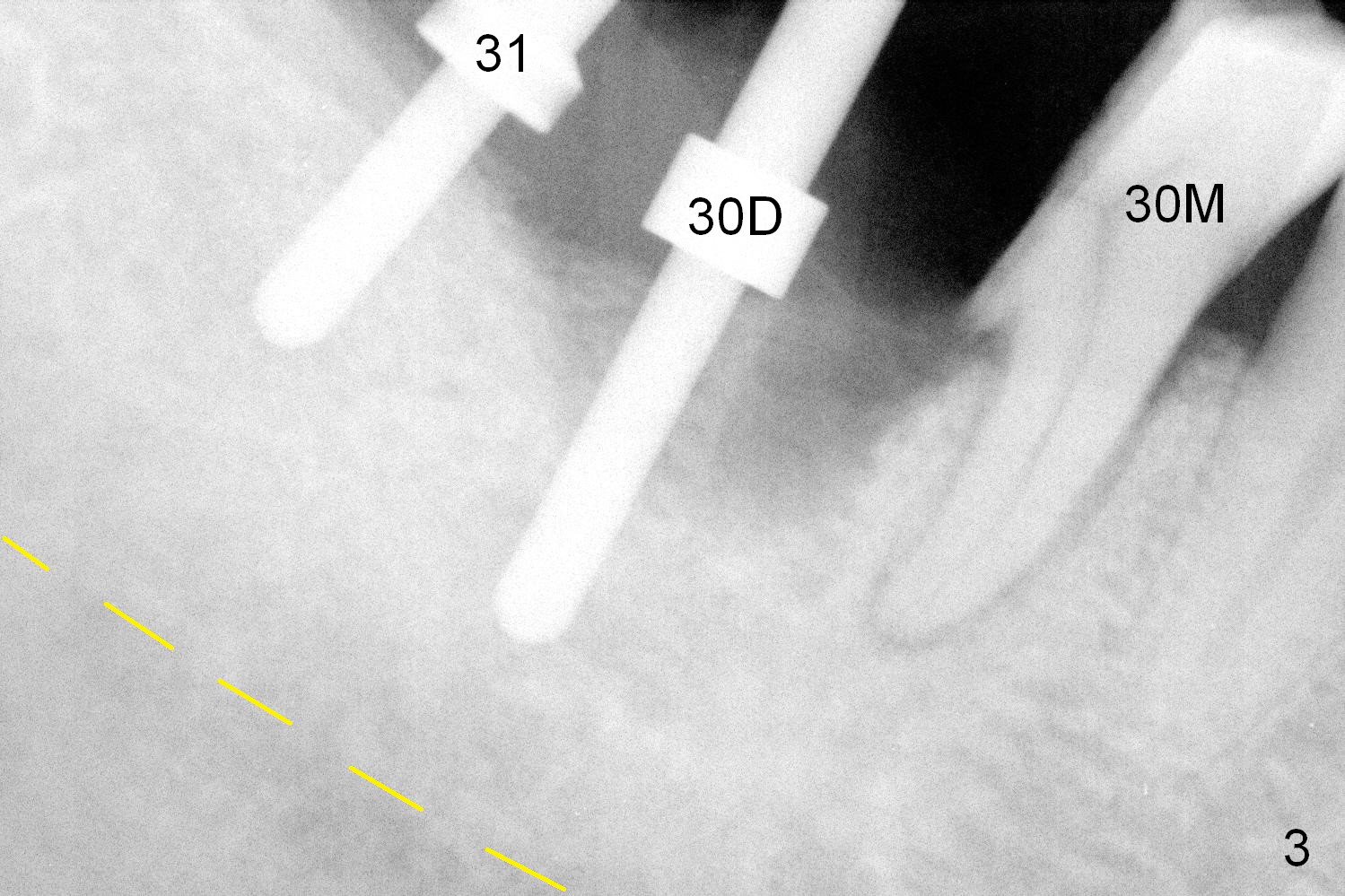
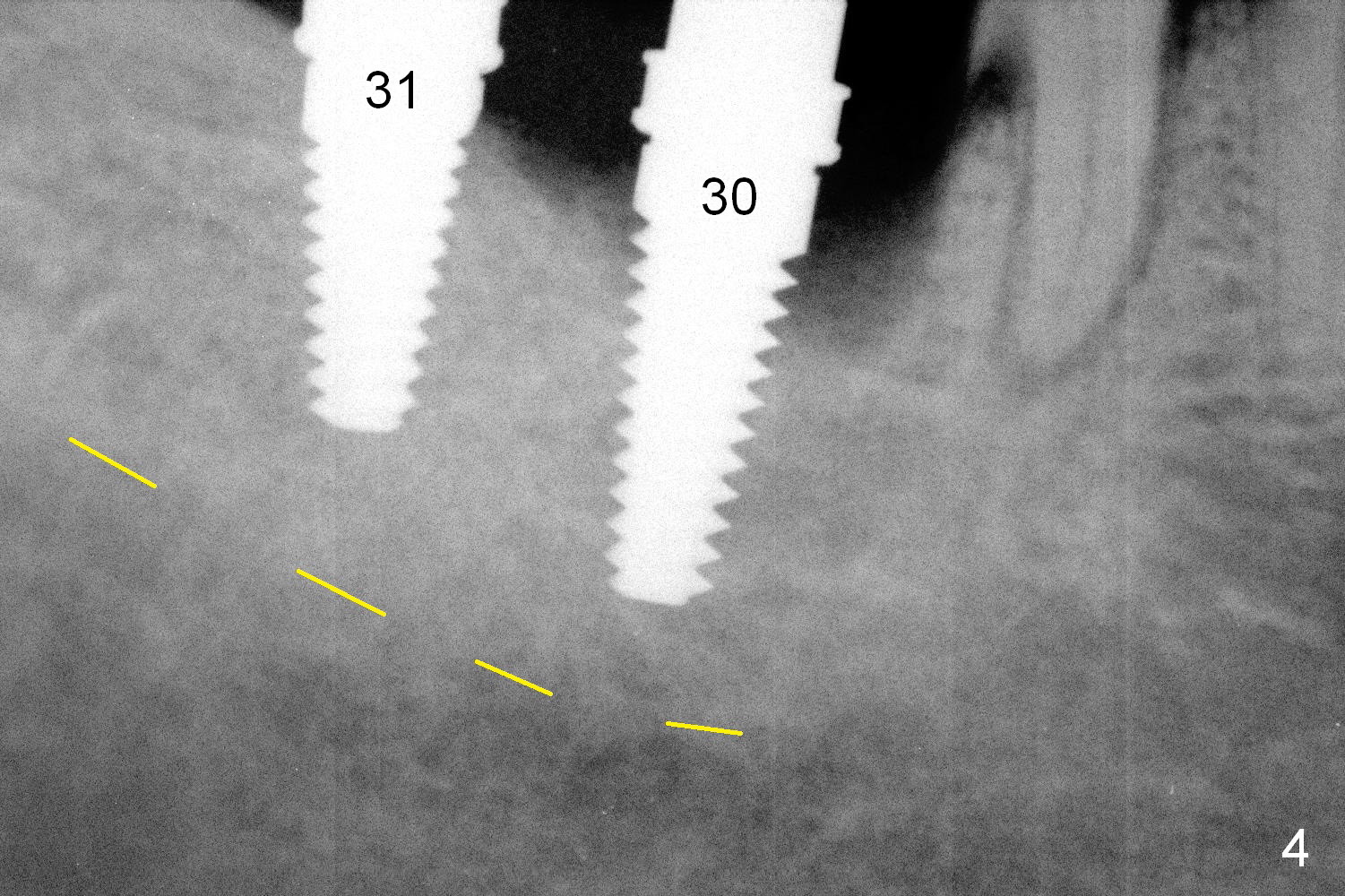
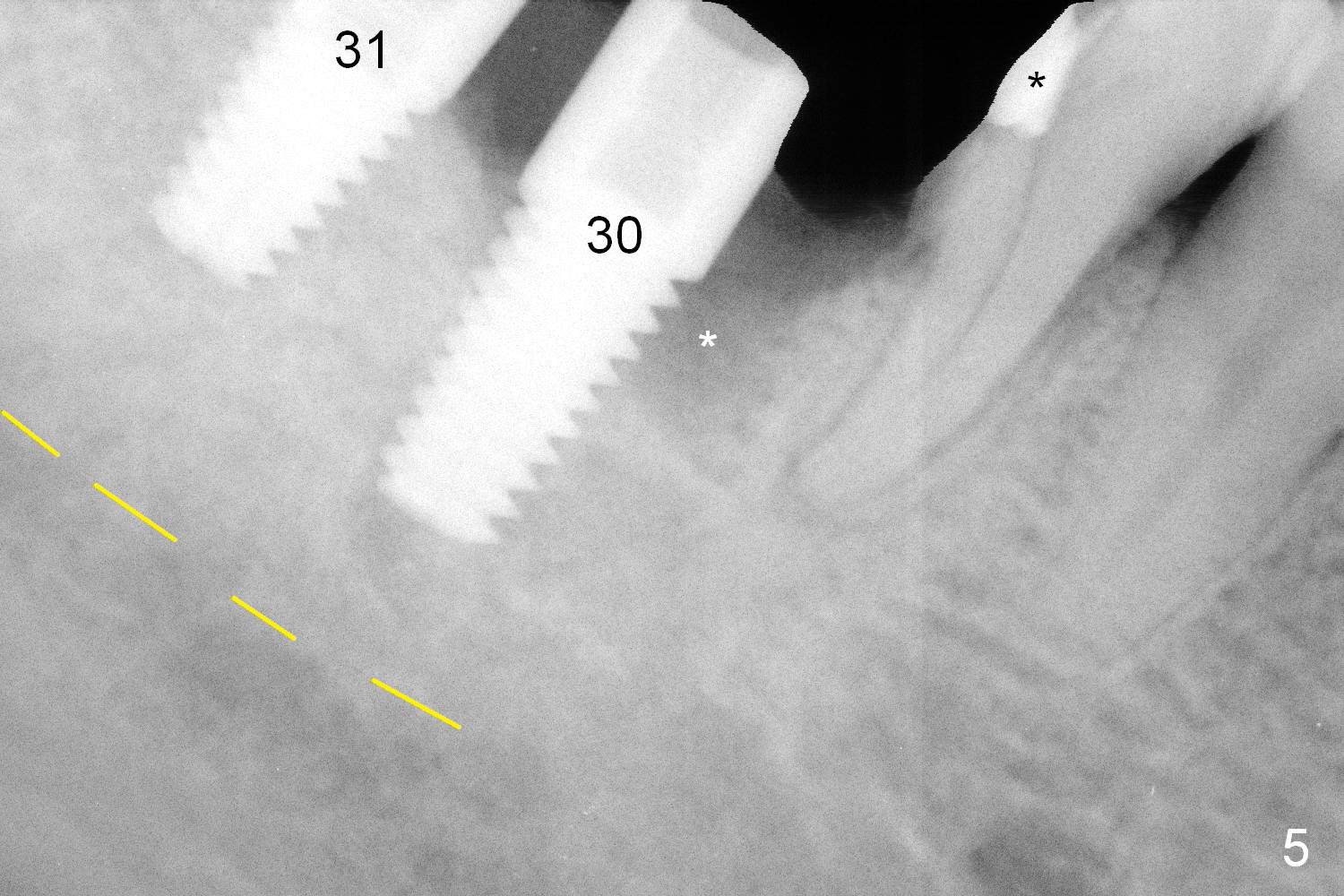
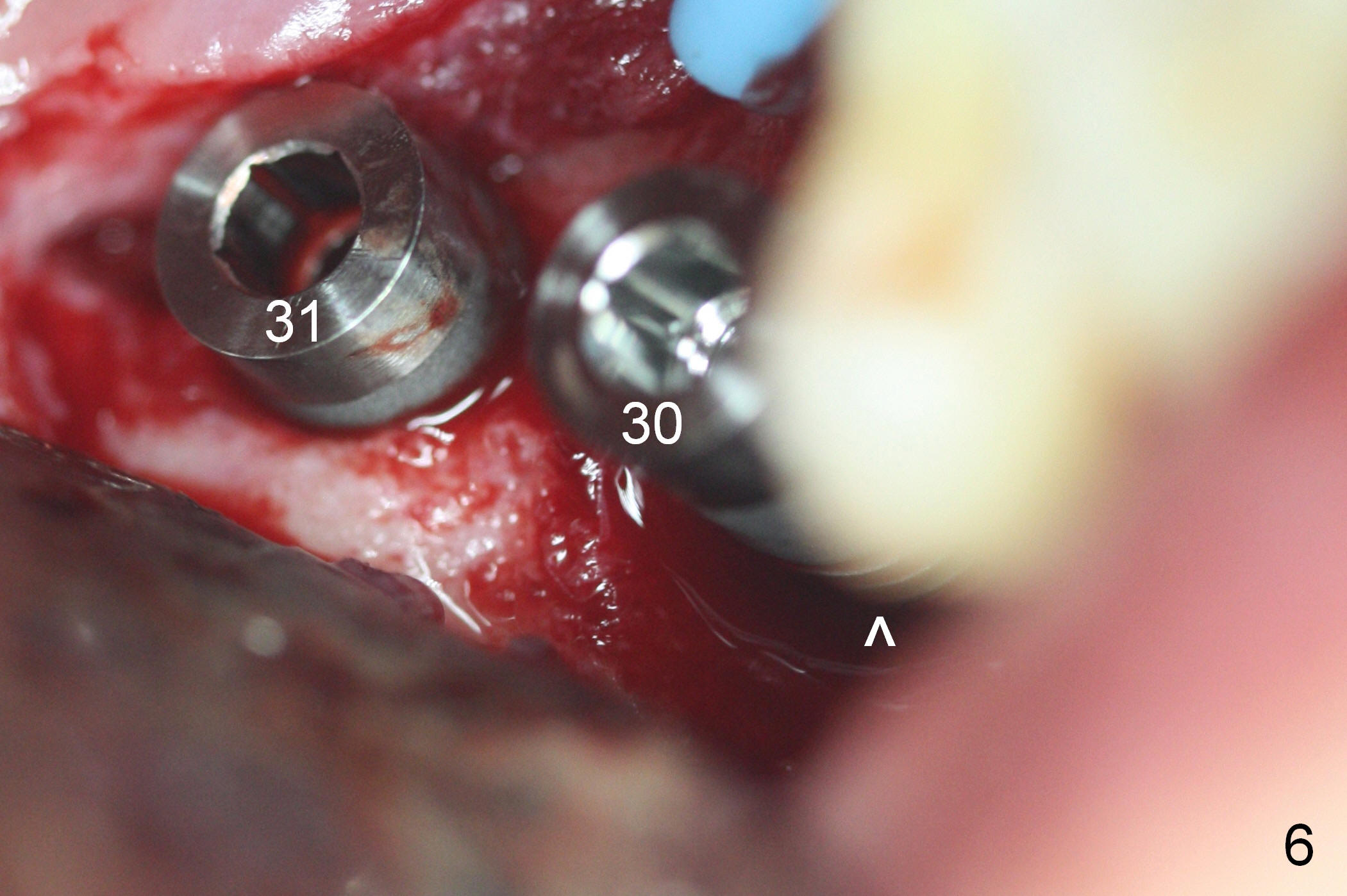
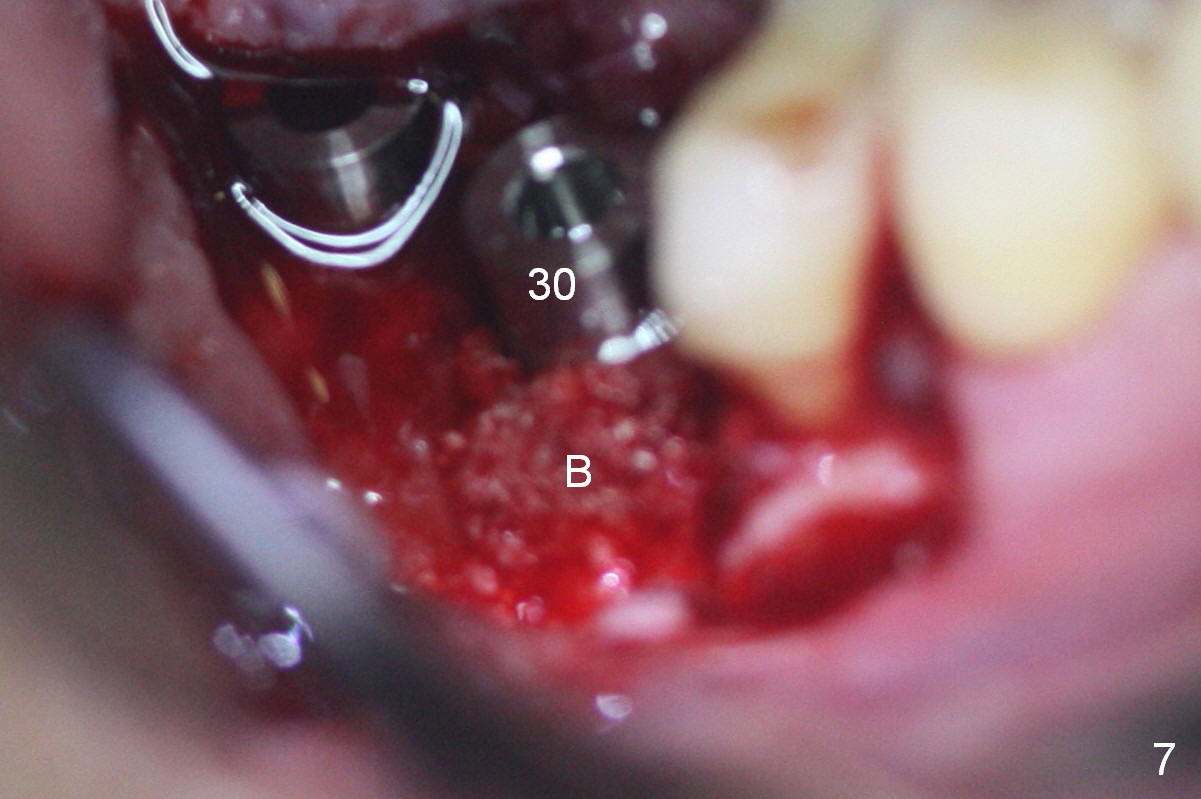
Buccal incision confirms severe bone loss around the DB root (Fig.2). The latter is easily removed after hemisection, whereas the distobuccal root is extracted with root tip picks. The mesial haft of the tooth is stable. Osteotomies are initiated in the enlarged DB socket of #30 and at the site of #31 (Fig.3). After placement of 4.5 mm taps (Fig.4), implants are placed with insertion torque >60 Ncm. The mesiobuccal defect at the site of #30 (Fig.5 *, 6 ^) is repaired with mixture of autogenous bone and Osteogen (Fig.7 B). The latter is covered by collagen dressing. The flaps are closed with suture. Perio dressing is applied after placing abutments.
In brief, an incision allows to identify lesion, place implants in precise position and cover exposed threads with bone graft securely.
The patient returns asymptomatic 6 days postop. The perio dressing is in place. There is no sign of infection.
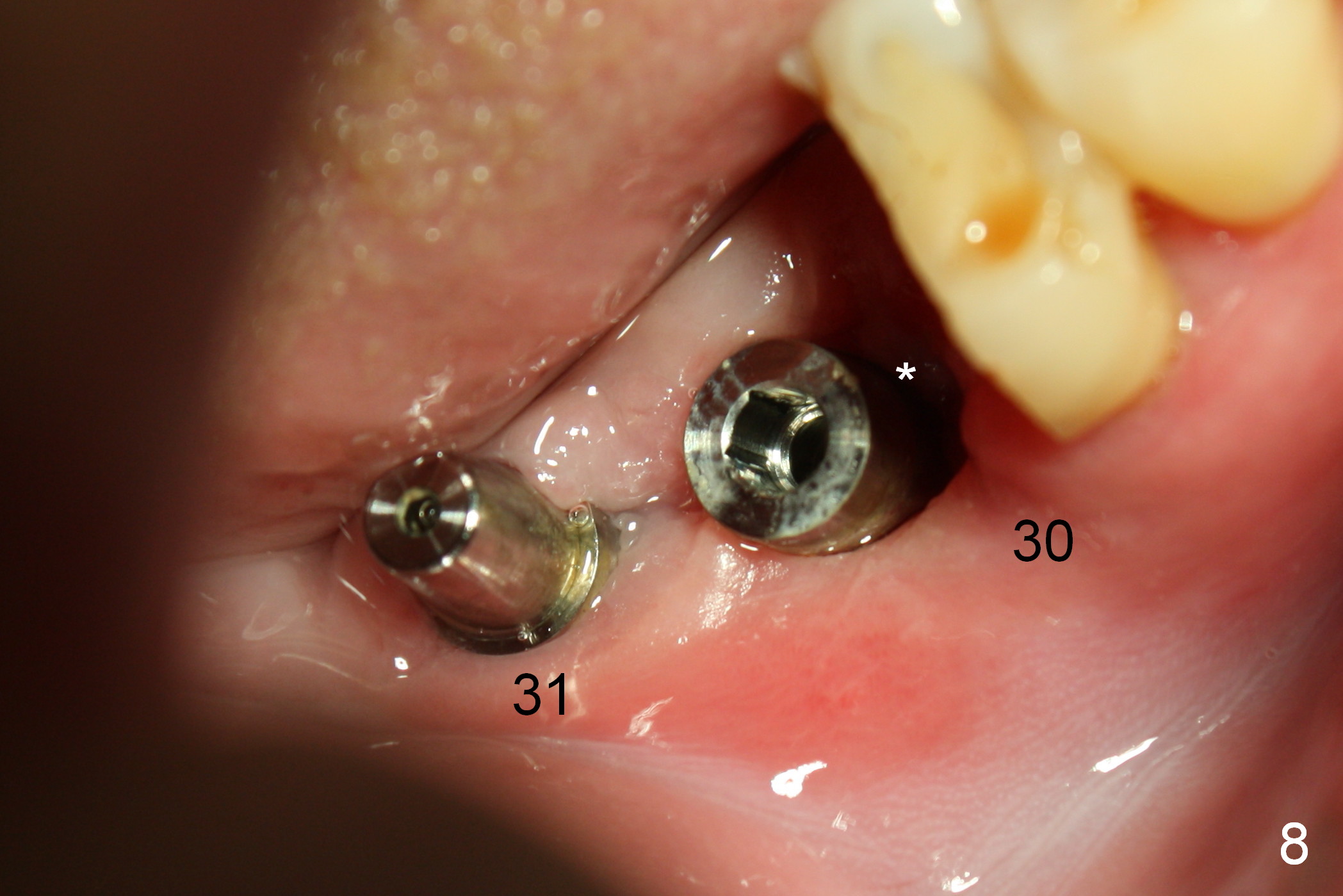
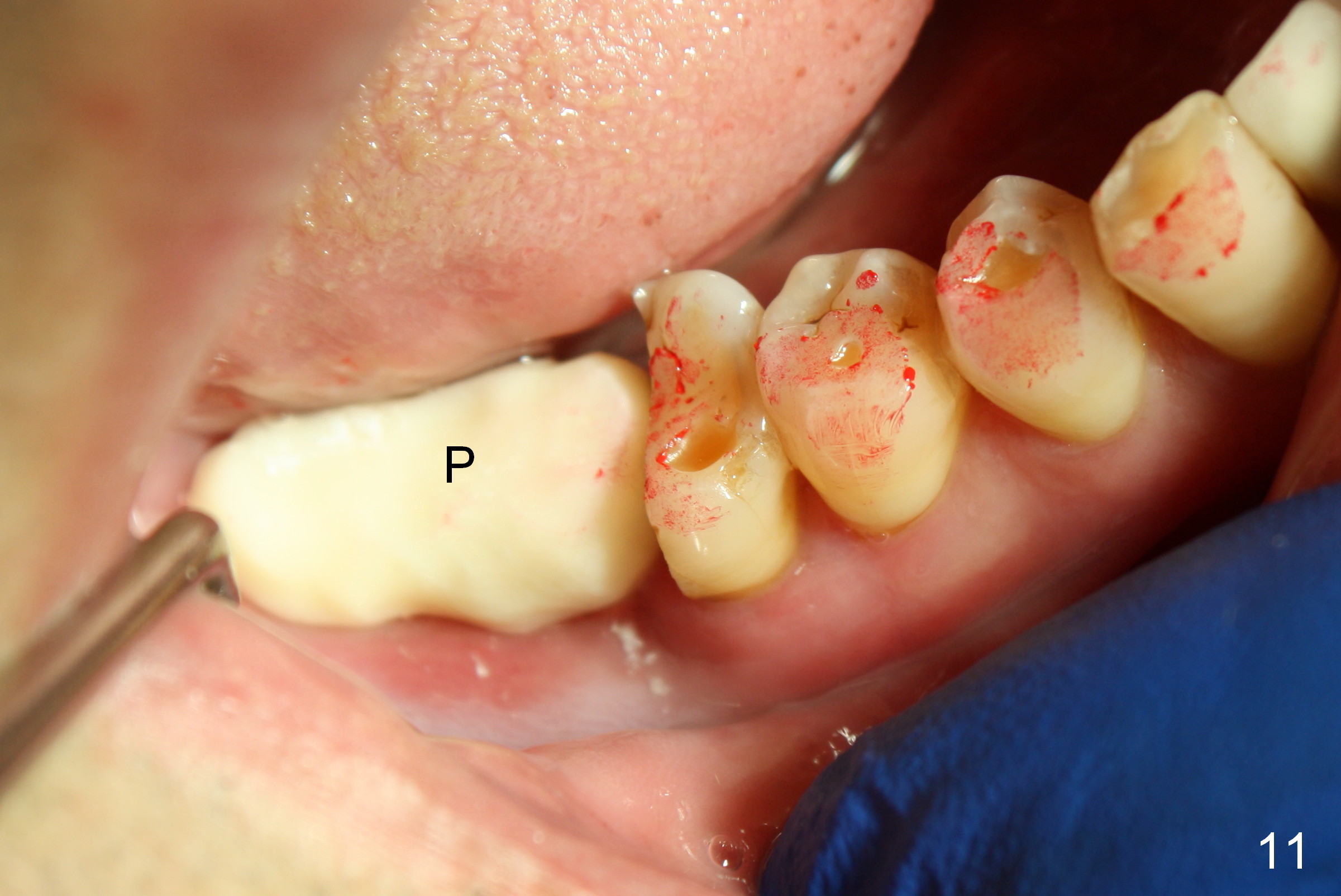
The perio dressing dislodges ~2 weeks postop. When the patient returns 19 days postop, the wound mesial to #30 implant is open (Fig.8 *) with loss of bone graft (Fig.9). After implant/abutment preparation and wound irrigation, bone graft is placed (Fig.10), followed by collagen dressing. Provisional restorations are seated to keep the bone graft and collagen membrane in place securely (Fig.11 P).
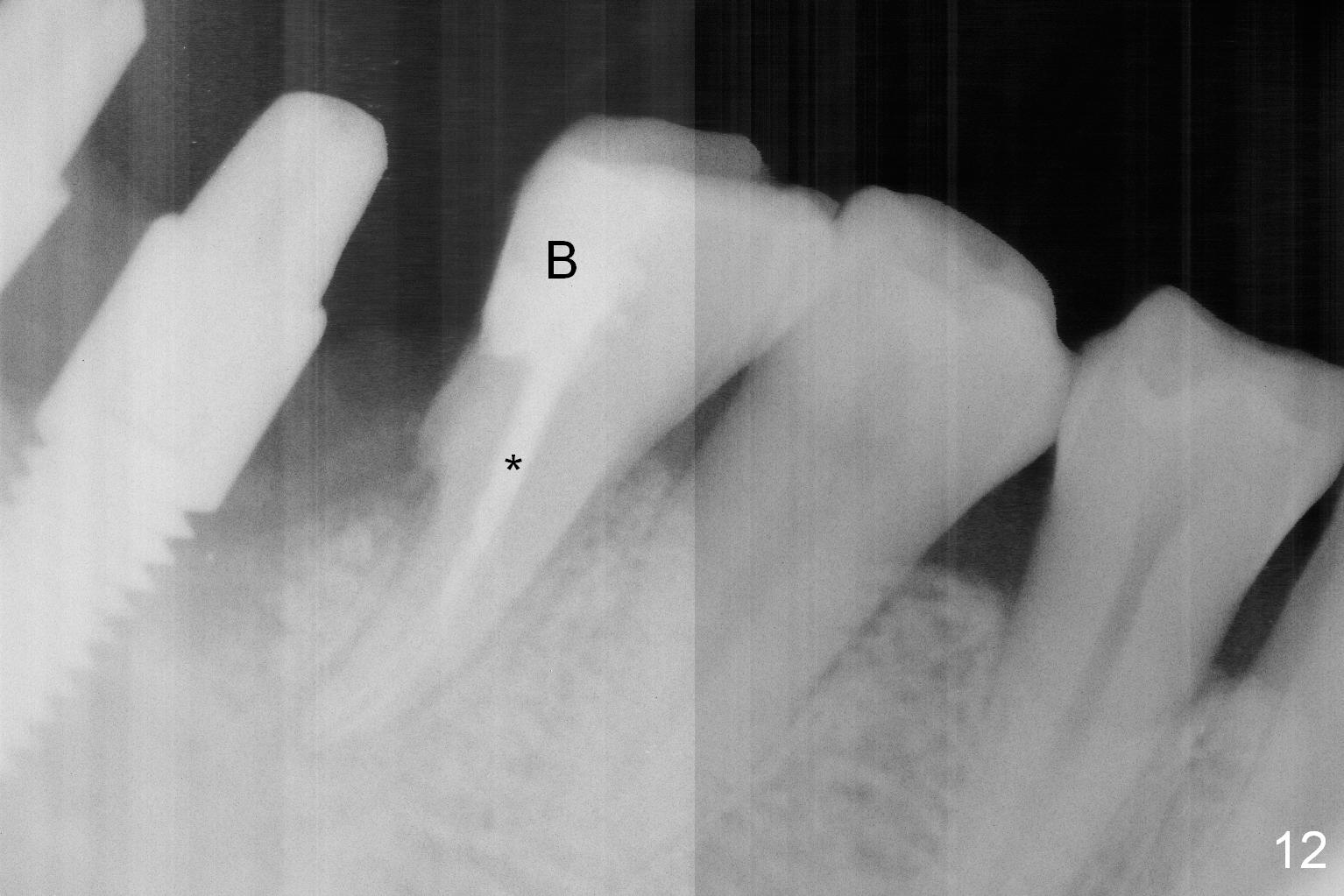
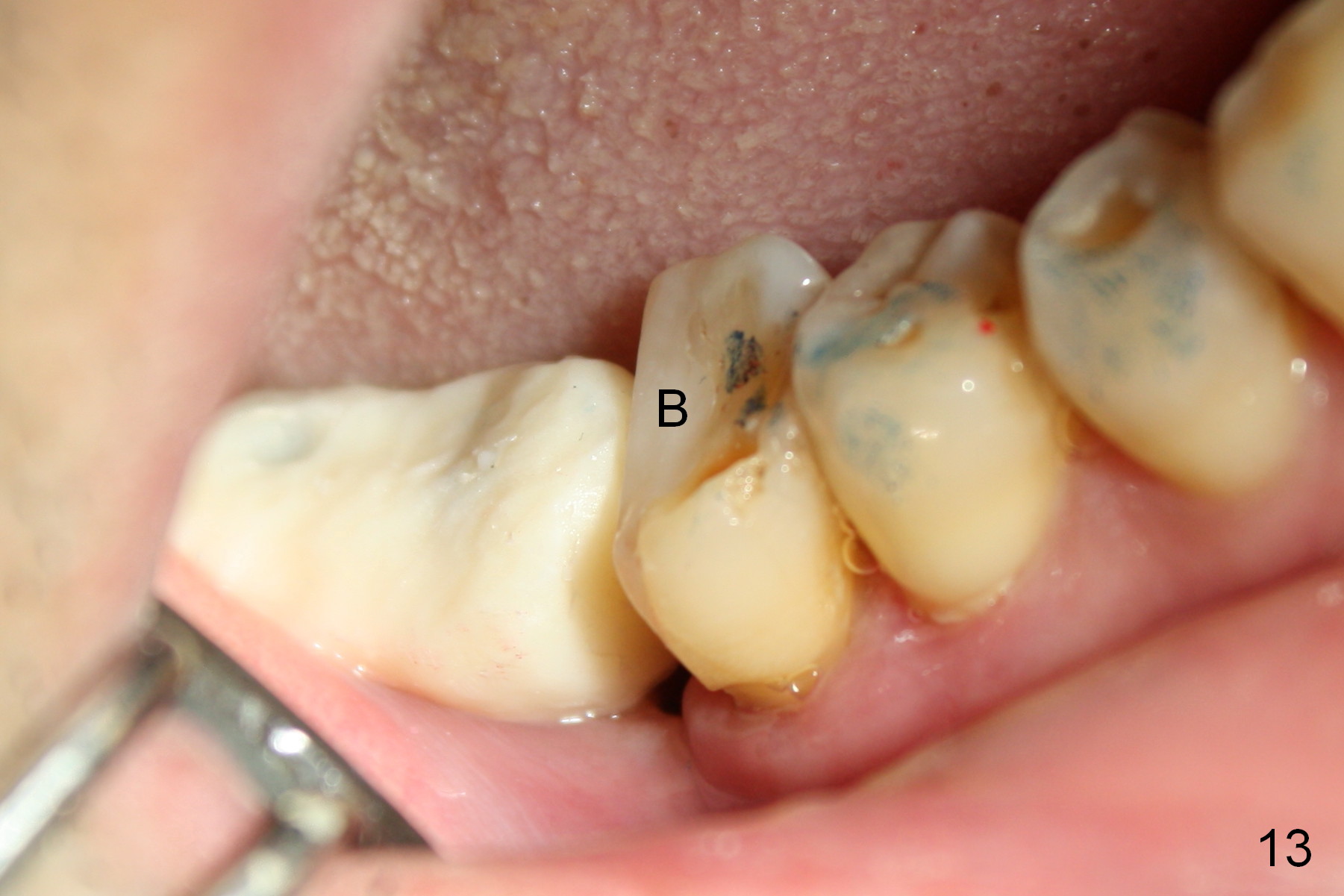
The patient returns for #30 mesial root canal therapy because of sensitivity 25 days postop (Fig.12 *). After build up (Fig.12,13 B), the provisional is relined and re-cemented. In fact the bone graft is not incorporated.
Return to Lower Molar Immediate Implant,
Dr. Wu
Xin Wei, DDS, PhD, MS 1st edition 03/26/2015, last revision 04/20/2015