



%20mm,%20.5-1%20mm%20Vanilla_1.jpg)

.jpg)

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1-Staged Ridge Split in the Mandible
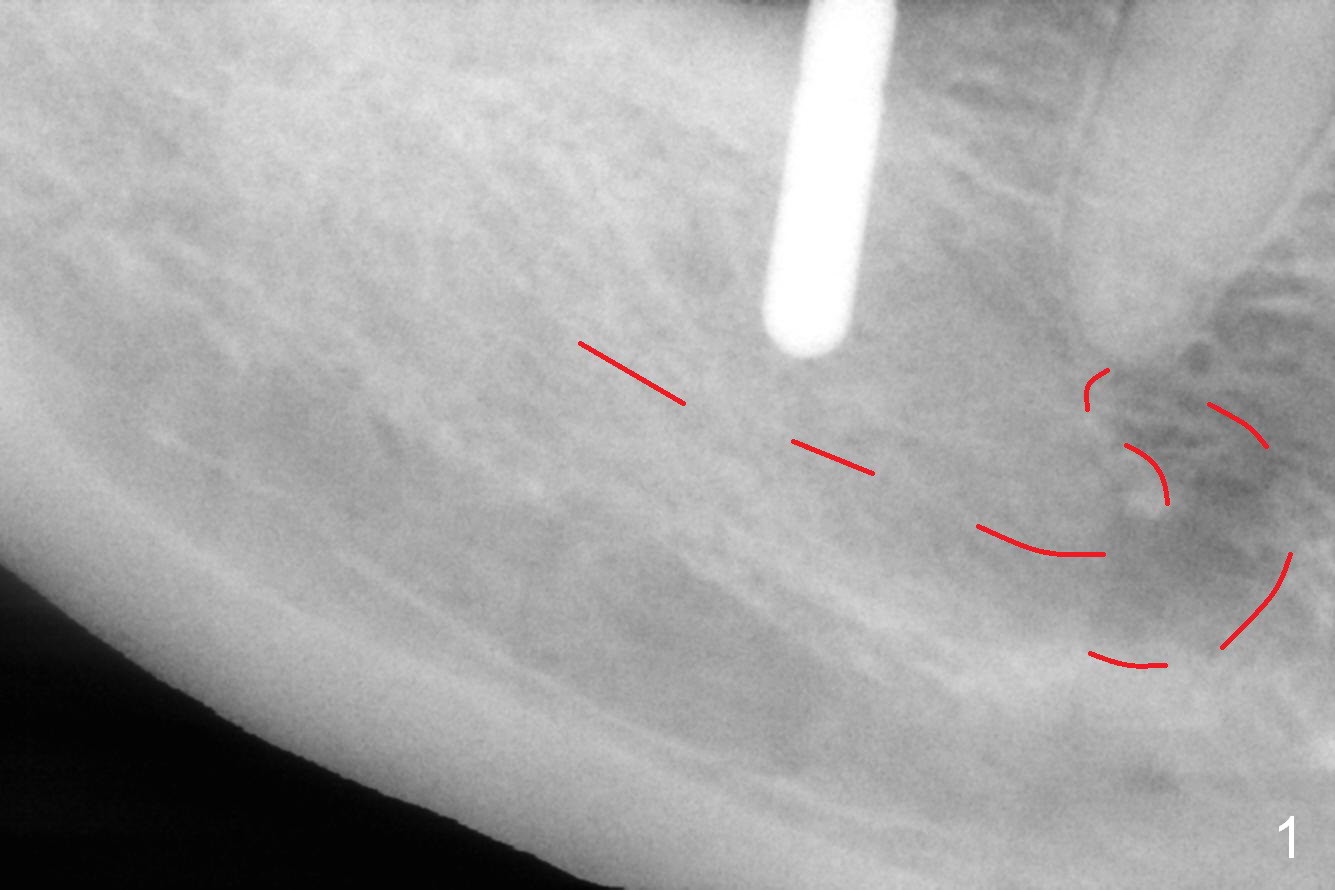
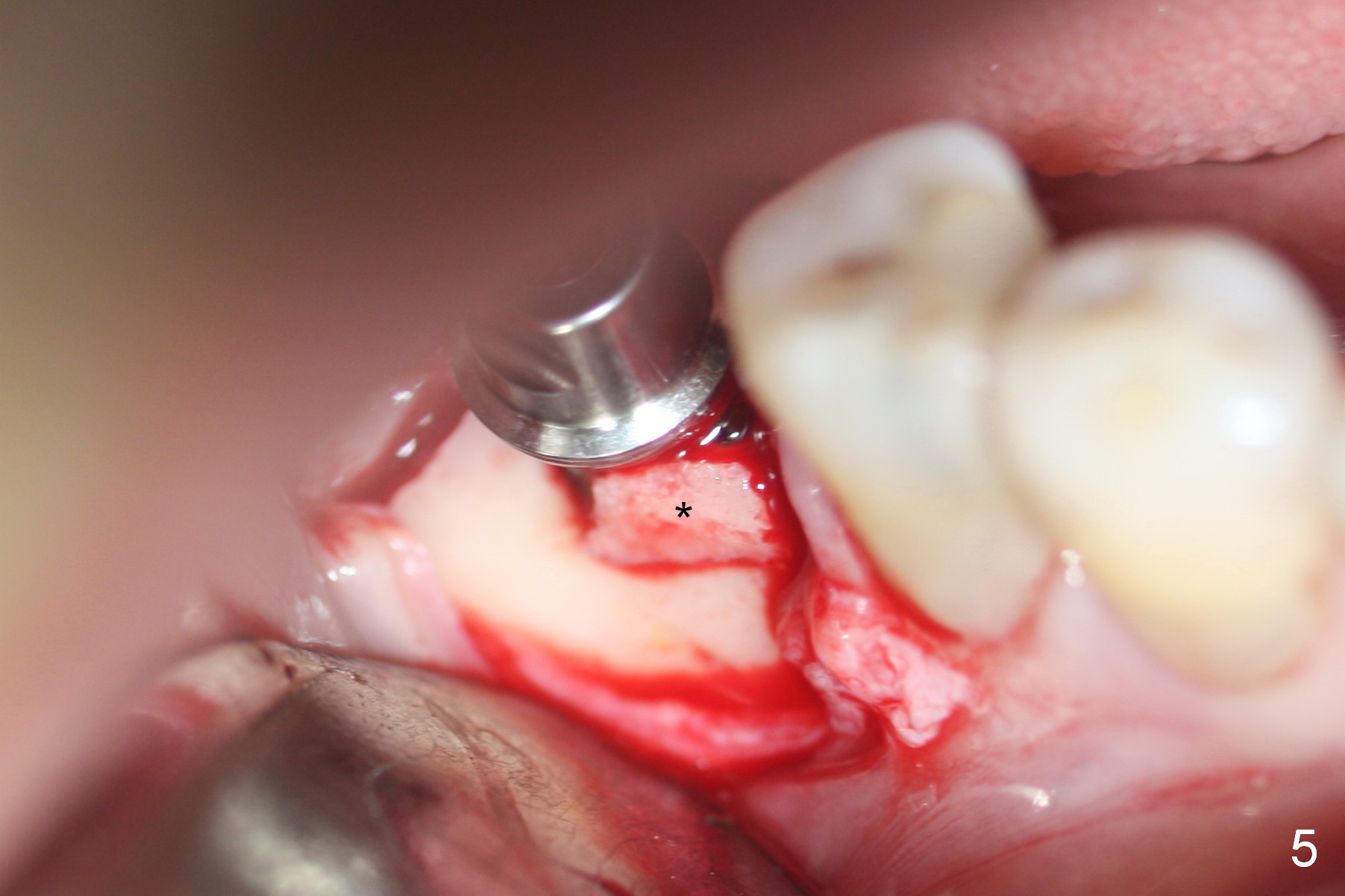
Incision reveals that the ridge is narrower than CT indicates. Considering that the patient is nervous, one-staged ridge split starts with ridge top split with surgical fissure bur, followed by a 2-mm pilot drill 8.5 mm deep. A calculated parallel pin is inserted for the 1st intraop PA (Fig.1 (red dashed line: the Inferior Alveolar Canal and Mental Foramen)). DIO 1.3/2.3 mm and 1.7/3.1 mm expanders are able to be inserted ~ 9 mm without obvious buccal plate deformity. When 2.4/3.7 mm expander is being used < 8 mm deep, the most coronal buccal plate starts to bulge (Fig.2,3 *). Two oblique accessory bony cuts (Fig.2,3 black arrow) are added without effect. A 3.2x8.5 mm drill is used mainly against the lingual wall (Fig.2,3 white arrow) prior to placement of a 4x8.5 mm implant (Fig.4). Due to incomplete seating with >50 Ncm and more buccal plate bulging, the implant is removed. A 3.2x10 mm drill is used for ~ 9 mm. The implant is re-inserted with deeper placement (Fig.7). When a 6.5x4(3) mm abutment is placed, the localized bulging plate fractures (Fig.5 *) with resultant mesiobuccal thread exposure (Fig.6). The fractured plate is repositioned with addition of mineralized cancellous/cortical allograft (.5-1 mm) with Osteogen (Fig.7 *). The latter is covered by collagen dressing. After suturing, setting acrylic dough is applied around the abutment, the wound and the distal undercut of the tooth #29 as an immediate provisional and secure dressing.
If the bone density at the crest were not so high, the buccal plate fracture would be less severe. #15 blade will be used to test the density of crest after incision for tomorrow case. Larger drill can be applied to the most coronal osteotomy, leaned against the lingual wall, to reduce stress in the crest. Primary stability will be mainly derived from the engagement to the cancellous bone.
When the immediate provisional is removed for revision 1 month postop, the gingiva around the abutment is healthy (Fig.8).
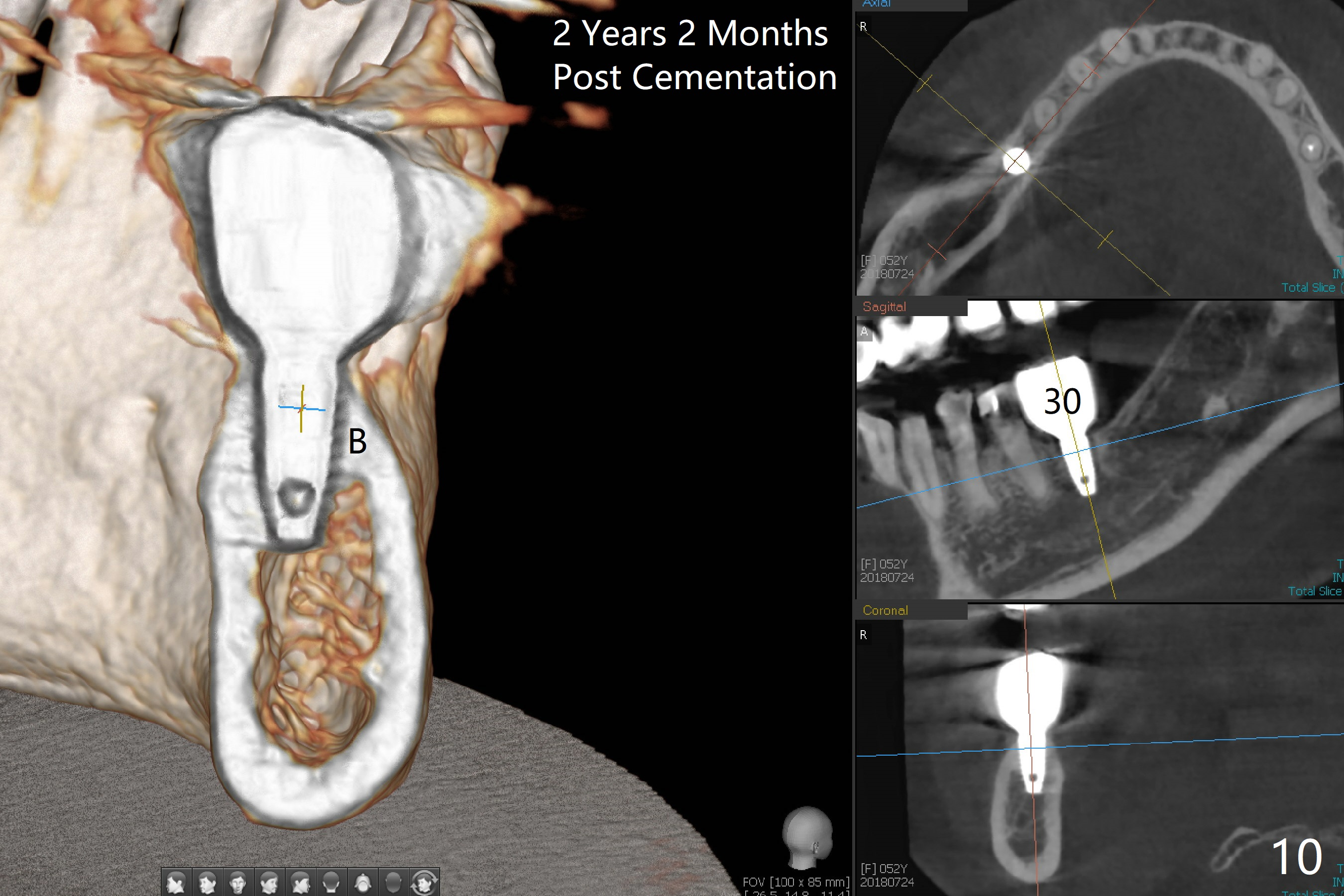
The provisional is lost 2 months postop. There is mild crestal bone resorption (Fig.9), but the gingiva remains healthy. A longer abutment with shorter cuff is used (6.5x5.5(2) mm) for impression. It appears that 1-staged ridge split is associated with more bone resorption than 2-staged one. There appears no bone resorption 2 years 2 months post cementation (Fig.10). There is no gingival recession 4 years 10 months post cementation (Fig.11).
Return to
Lower Molar Immediate Implant,
Berkeley,
Posterior Immediate Provisional, #13
14
14/19 Guide
劈开术
Xin Wei, DDS, PhD, MS 1st edition 01/27/2016, last revision 04/01/2021