|
|
|
|
|
|
|
|
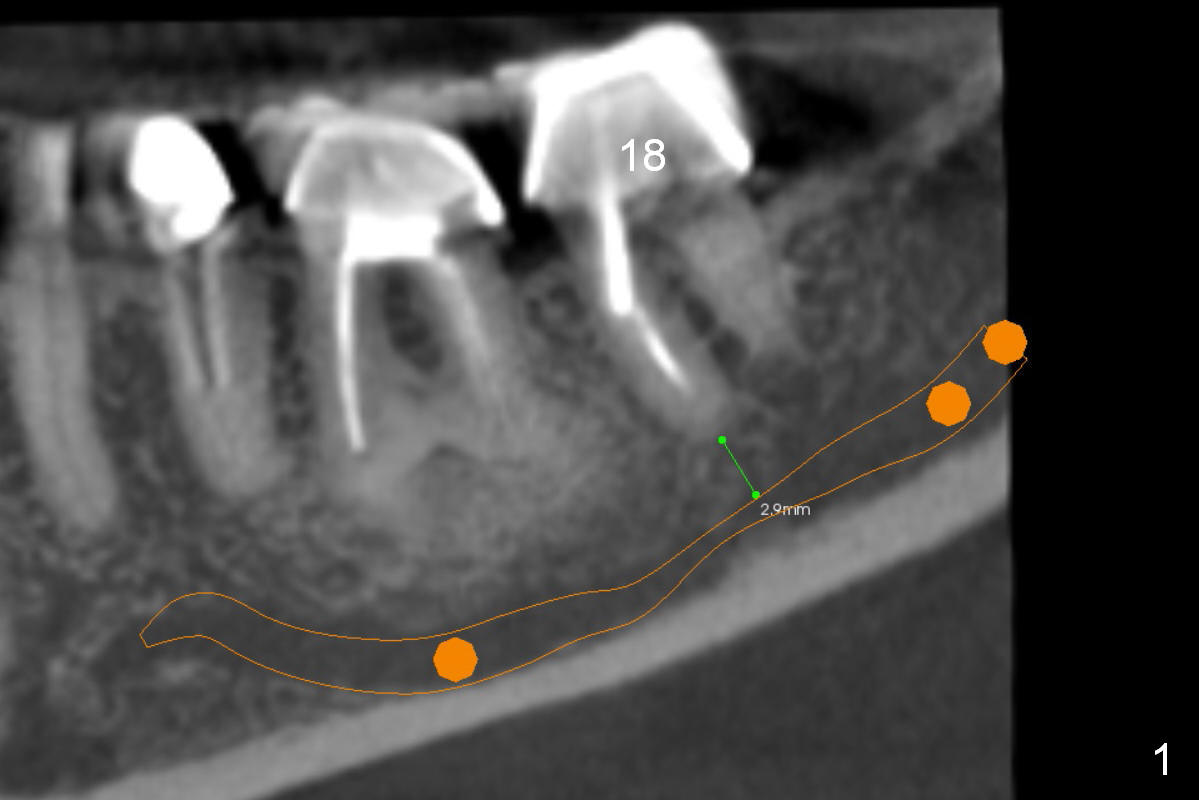
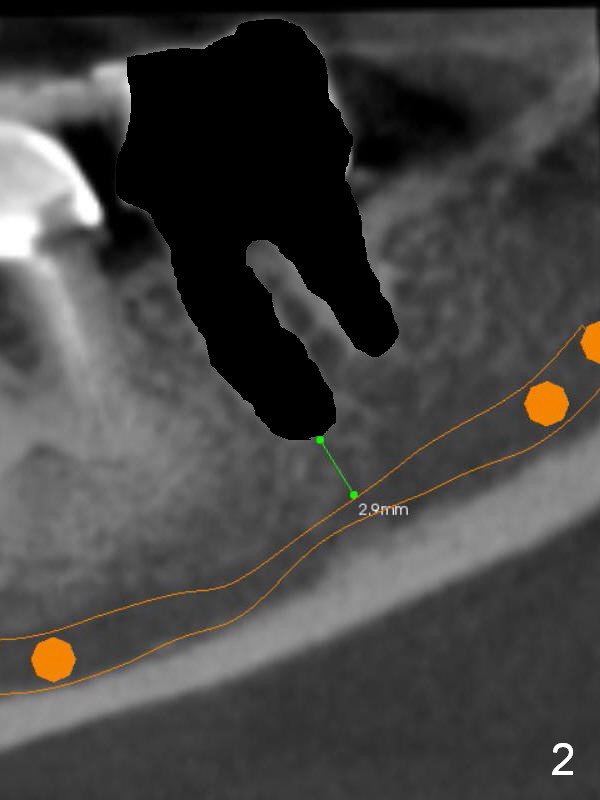
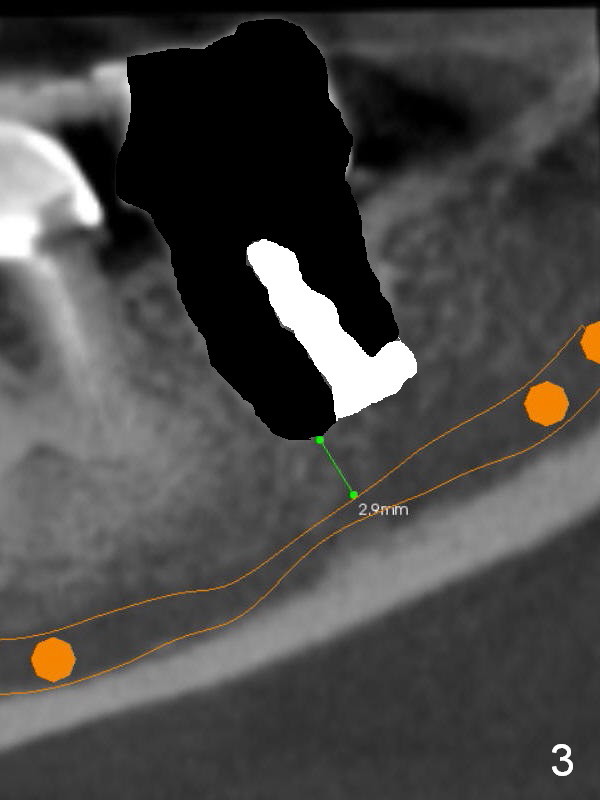
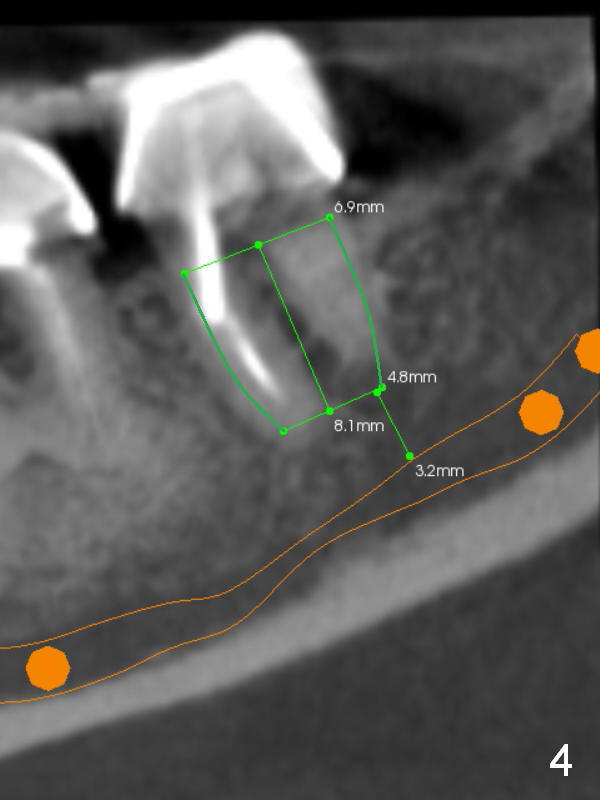
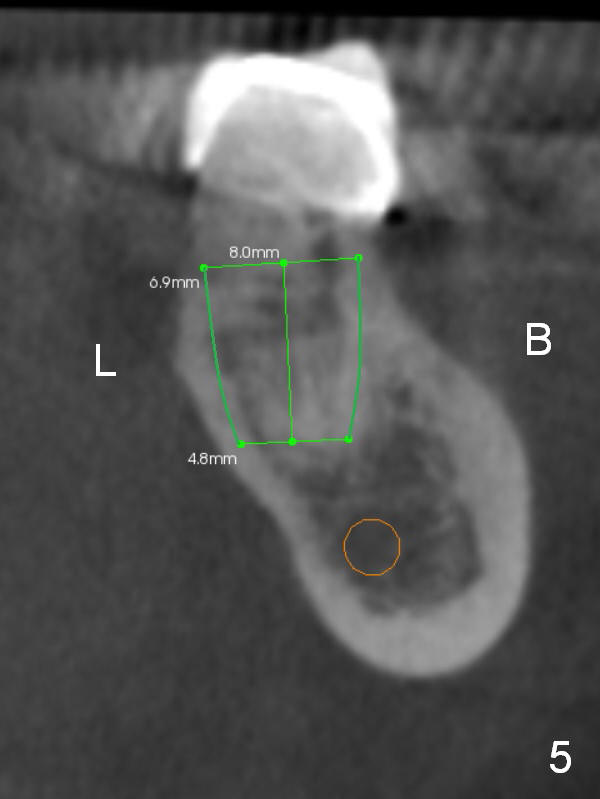
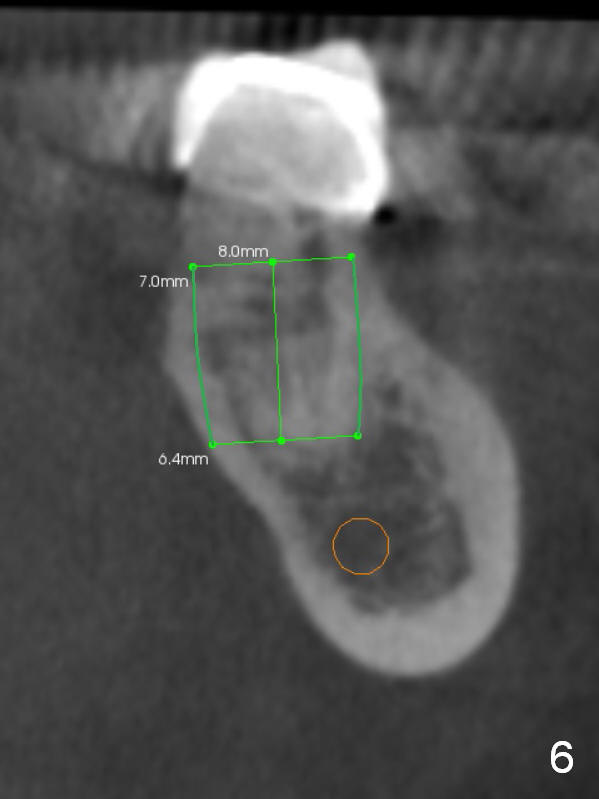
Osteotomy Confined to Socket
When the apex of the lower 2nd molar is 2-3 mm from the Inferior Alveolar Canal (Fig.1 (CBCT sagittal section), it is safe to place a large bone-level implant within the socket. After extraction (Fig.2 black area), check whether there is buccal and/or lingual plate defect. If the defect is severe (periodontitis), immediate implant should be considered being aborted. If the defect is minimal (tooth fracture), remove the septum (not beyond the apex of the socket (Fig.3 white area)). Use large taps until stability is achieved, i.e., when the tap contacts the buccal and lingual plates. Taper of SM implant (Fig.4,5 (coronal section)) matches the shape of the socket (B: buccal; L: lingual). If primary stability of SM tap is not high, try UF one (more or less cylindrical) and place the corresponding implant (Fig.6).
Return to Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 10/31/2015, last revision 10/31/2015