




|
|
|
|
|
|
|
|
|
|
|
|
Socket Preservation Due to Insurance
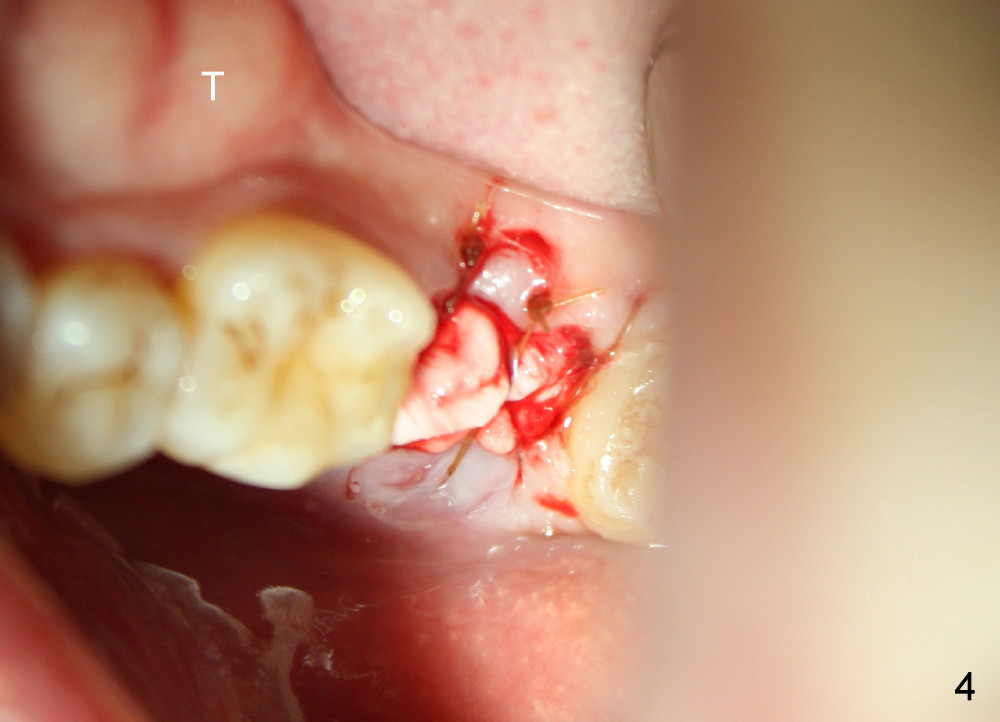
A 46-year-old man presents with toothache in the lower left 2nd molar (Fig.1). Exam shows a disto-occlusal crack line (Fig.2 ^). An explorer makes the crack larger (Fig.3). The crack line extends to the distal root surface (Fig.6 <). The patient wants to buy dental insurance before placing an implant. The tooth is extracted and socket preservation is performed (Fig.4). The mandibular torus (T) suggests bruxism. In fact, he fails to get an insurance eventually. He does not want to return for implant eagerly. Immediate implant should have been done in the first place.
Fig.1 shows that the roots are converged with a thin septum in between (< in Fig.5 buccal view of the extracted tooth). The socket is basically single and large. A 7x14 mm tapered implant seems to be appropriate for the site. Fig.2-4 show the wide ridge. Two months post extraction, the ridge should not be atrophic too much.
Osteotomes will be used to initiate osteotomy, followed by tap insertion. Depth of the osteotomy should not extend 3 mm beyond the apex of the socket (Fig.7). PA is to be taken prior to implant placement for depth confirmation.
Return to Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 12/22/2014, last revision 12/22/2014