|
|
|
|
|
|
|
|
|
|
Drawback of No Preop PA for Lower 2nd Molar
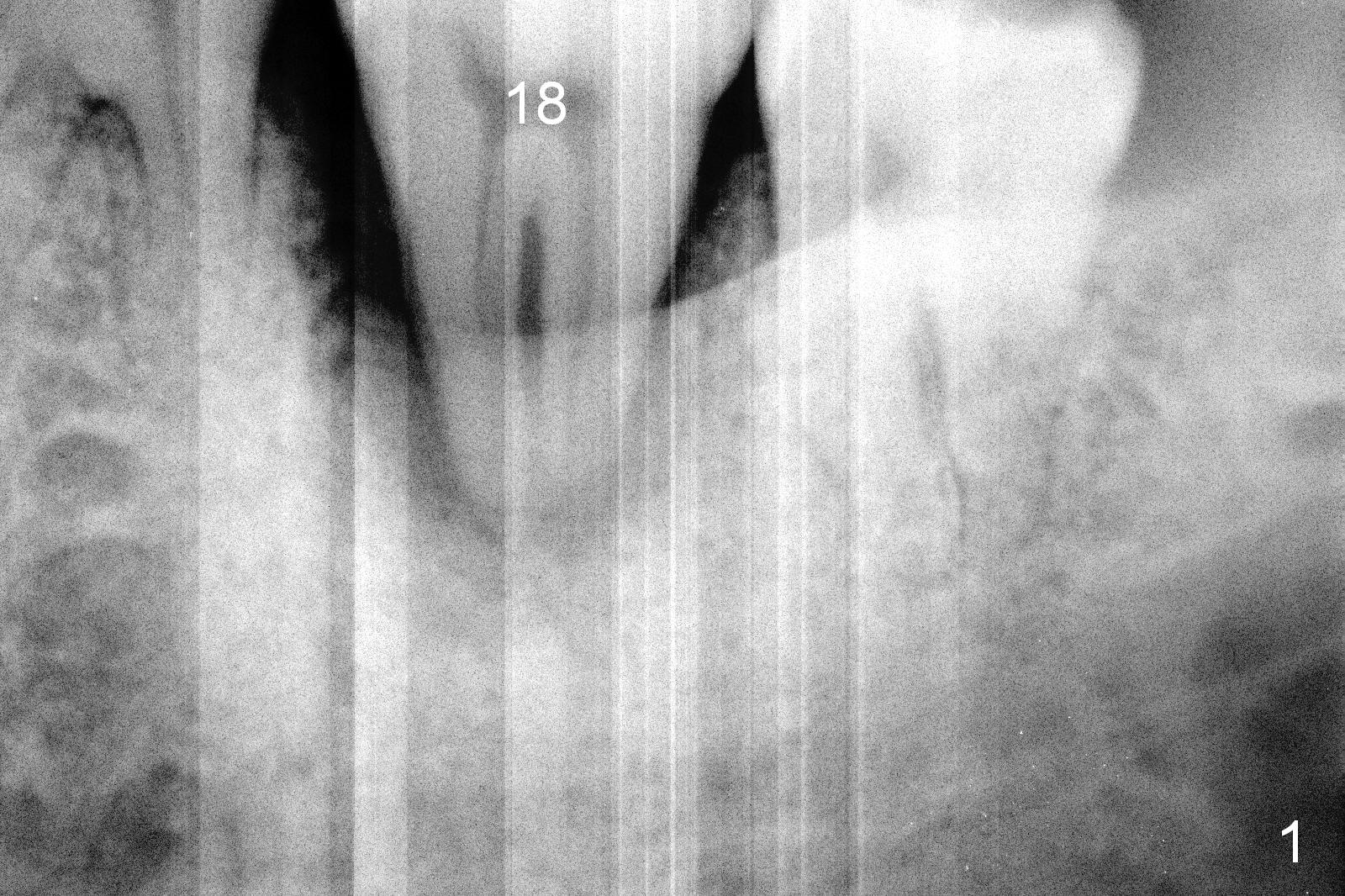
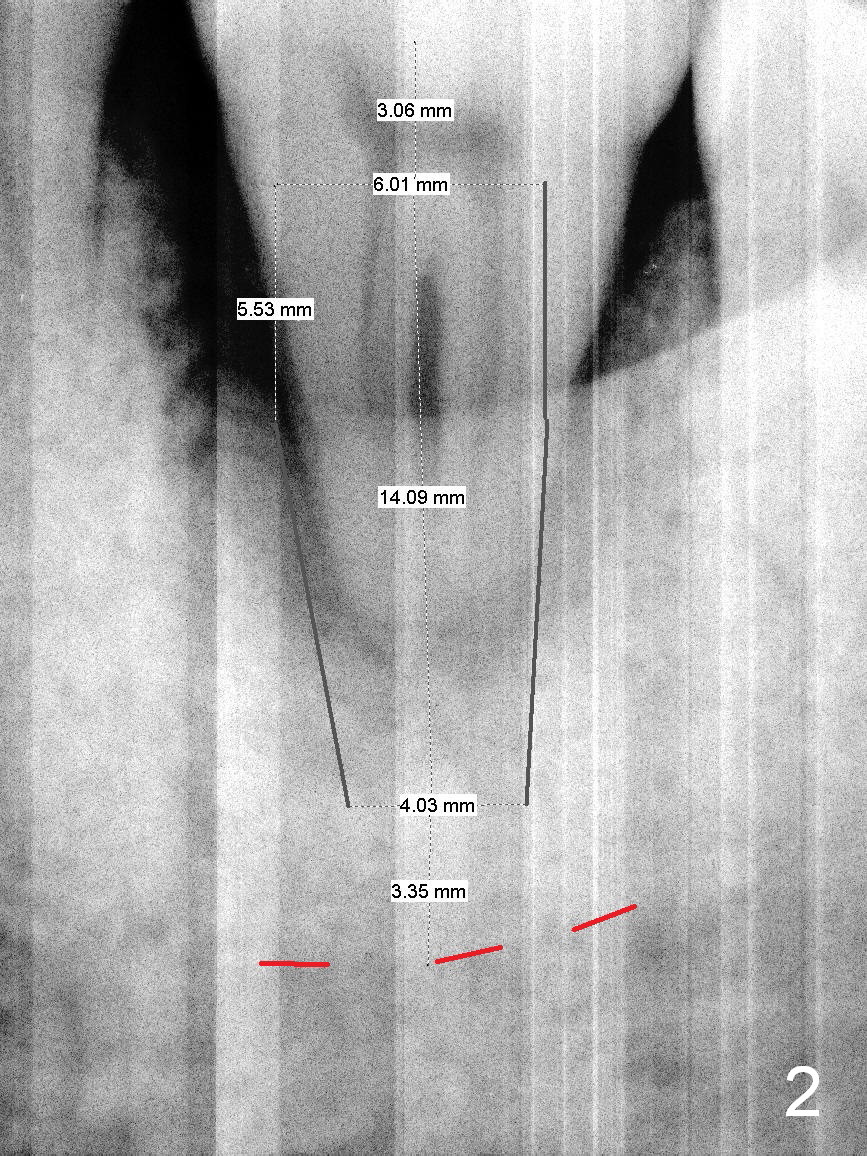
When the patient returns for #18 immediate implant, a PA is taken (Fig.1). She is nervous. Time is spent on explanation of necessity of extraction and implant. Little time is used for design of the implant (Fig.2: 6x14 mm) and appreciation of safety margin (3.35 mm from the superior border of the Inferior Alveolar Canal (IAC) (red dashed line)). Preop palpation reveals no submandibular fossa.
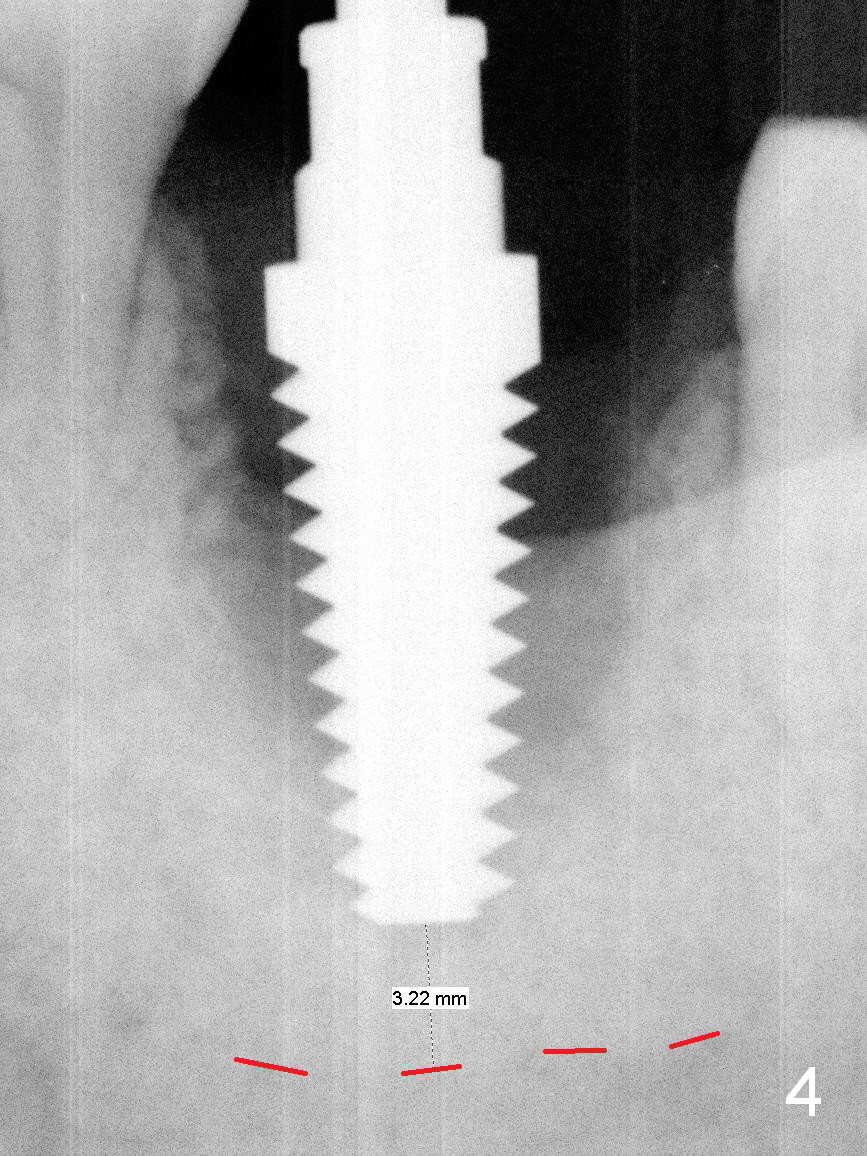
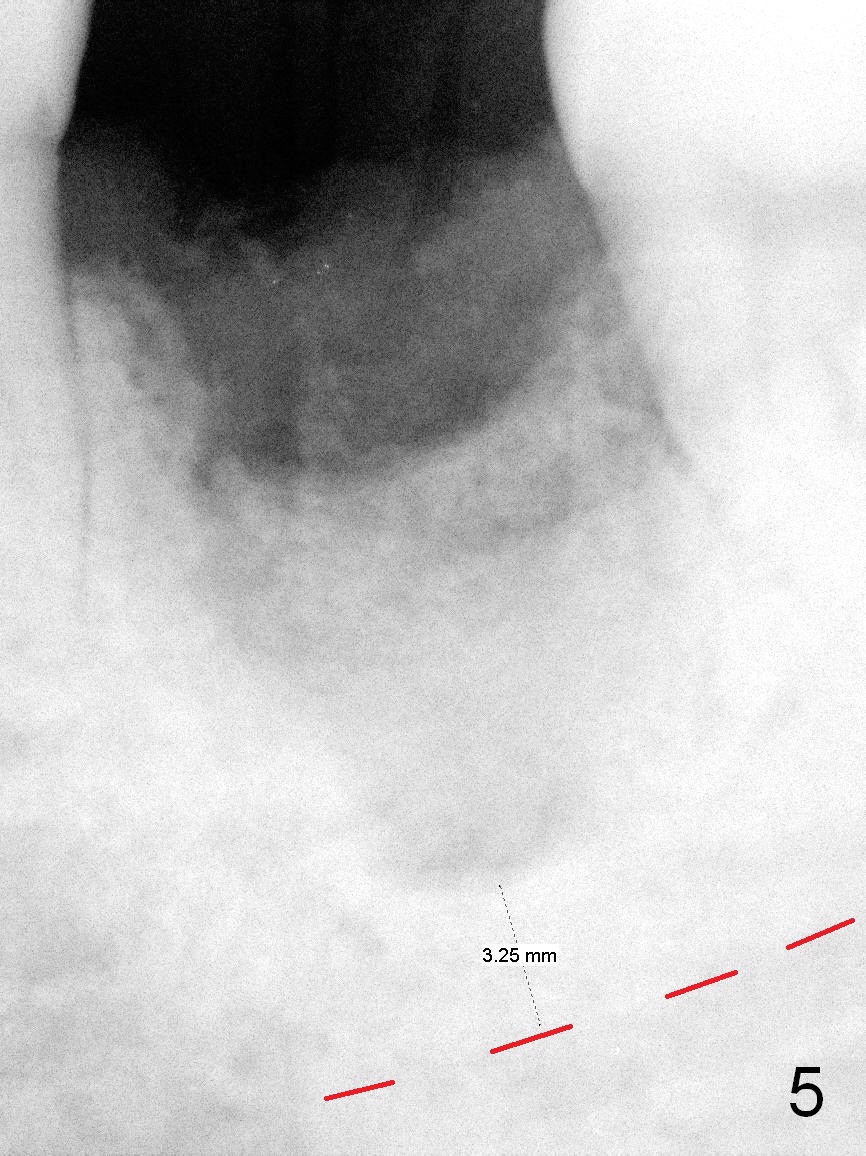
The buccal and lingual plates are found to be low after extraction. To achieve primary stability, apical new bone should be obtained. Initial osteotomy appears to be overachieved (Fig.3 (yellow dashed line: the inferior border of IAC), while later osteotomy is underachiever (Fig.4: 6x17 mm tap). A 7x14 mm implant cannot achieve stability. Socket preservation is done (Fig.5). There is no postop paresthesia. If the osteotomy were done 2 mm more (Fig.4,5), primary stability might be obtained with increased probability of nerve damage. Bone density in fact is high.
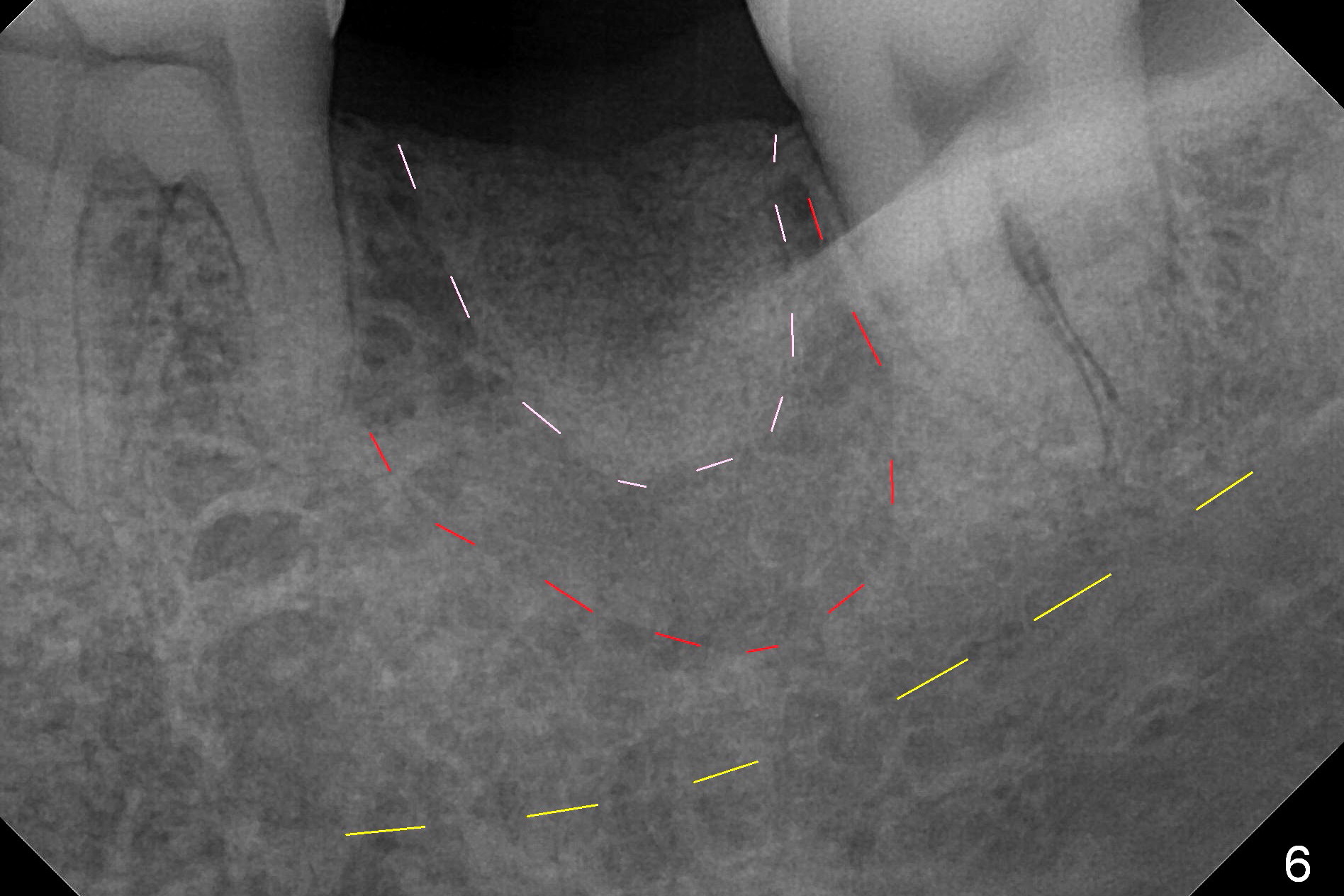
She does not return for treatment until 15 months later. The socket outline is preserved (Fig.6 pink dashed line). The buccal or lingual plate is most likely concave (red dashed line). If this is the case, the ridge top will be trimmed. The bone height before trimming is 14 mm. For safety, a 11 mm long implant will be placed. If the trimming is necessary, use a 7 or 9 mm one. Magicore will be used if the ridge is narrow. Use a healing cap for provisional or perio dressing. It is a piece implant or tissue-level one. Magicore solid abutment is similar to unipost.
Return to Lower Molar Immediate Implant,
IBS
Xin Wei, DDS, PhD, MS 1st edition 10/15/2015, last revision 02/13/2017