
,%20no%20graft.jpg)
|
|
|
|
|
||
|
|
|
|
|||
|
|
|
|
|
|
|
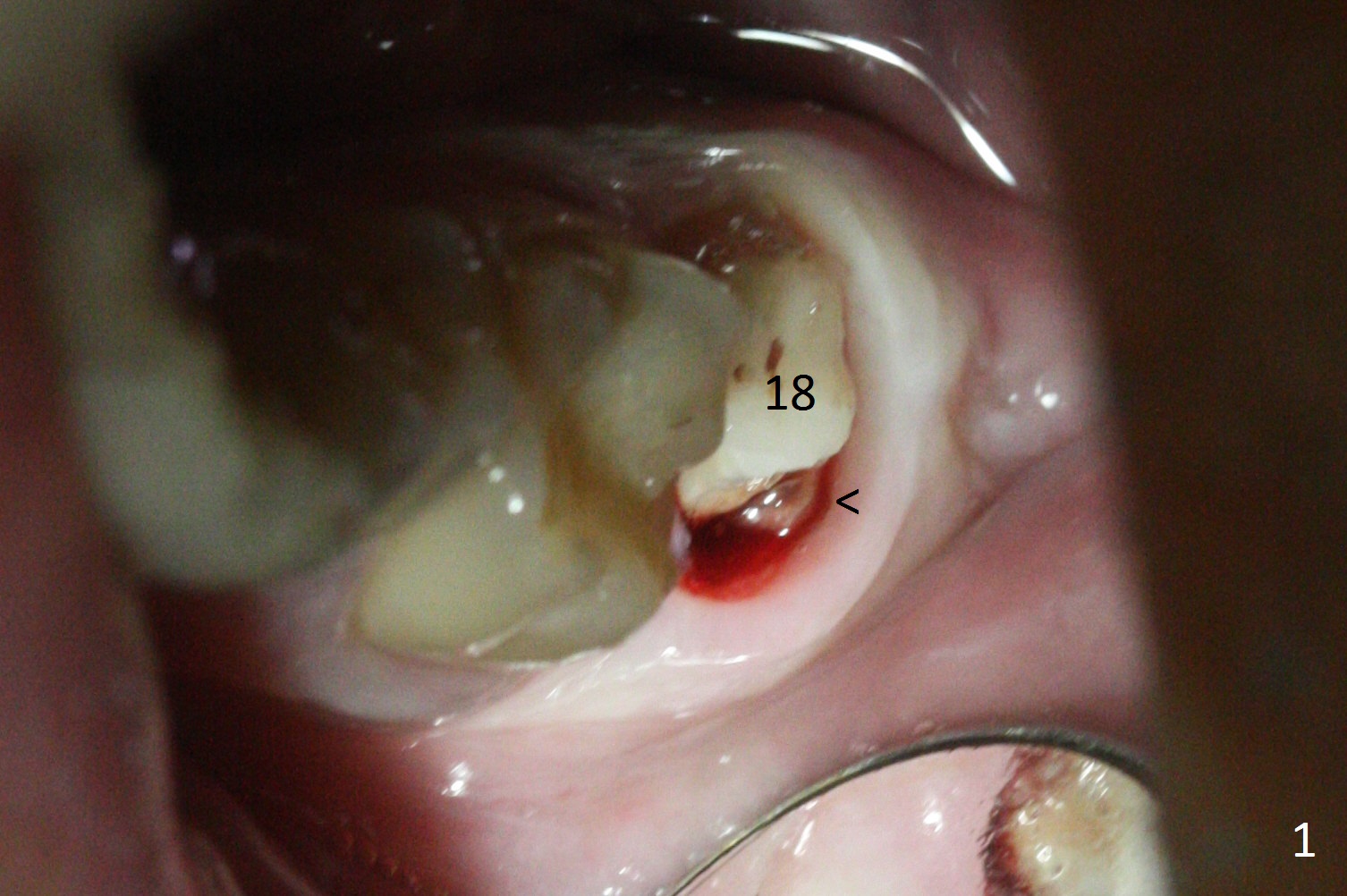
Limited Vertical Height for Crown
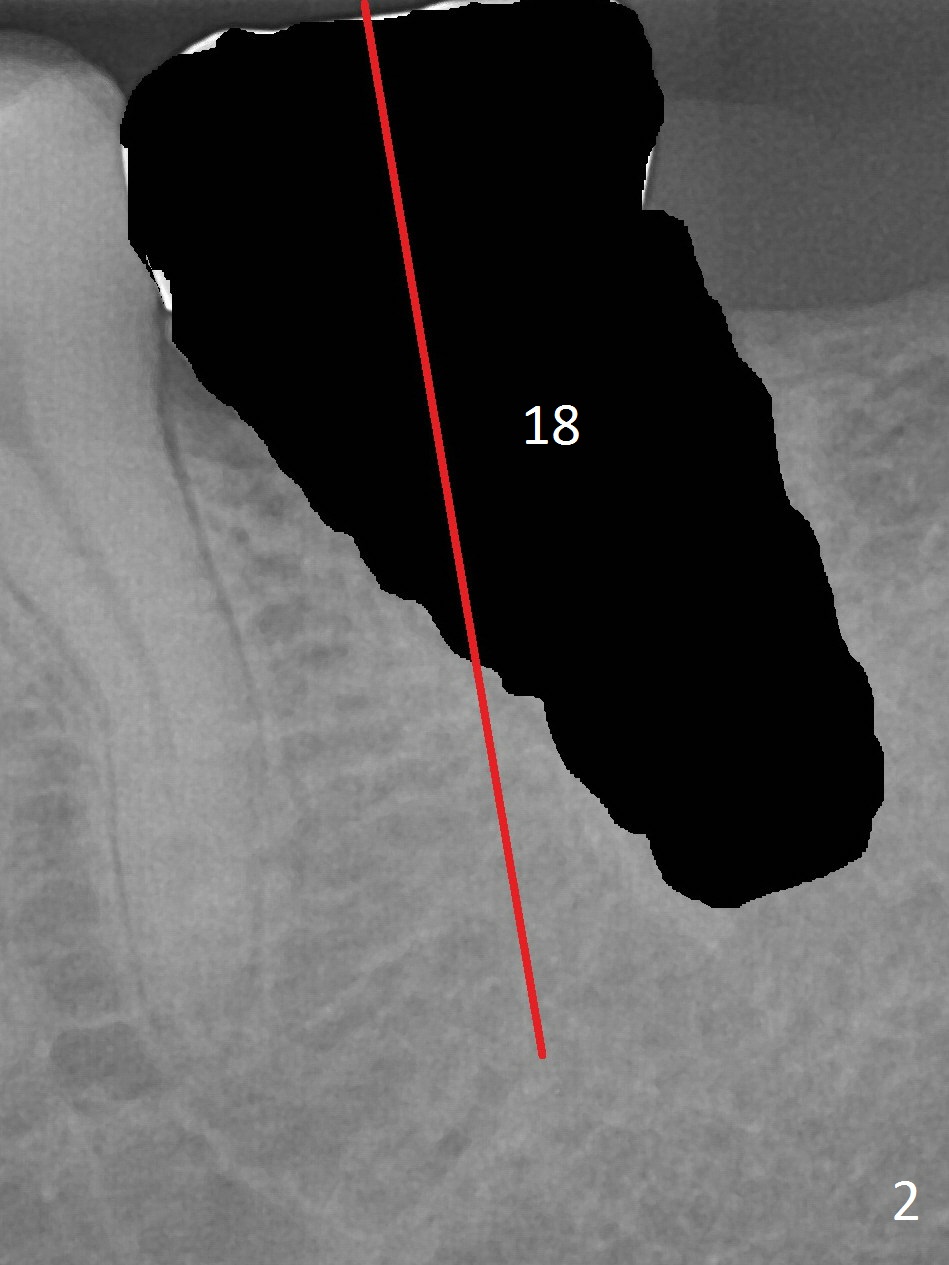
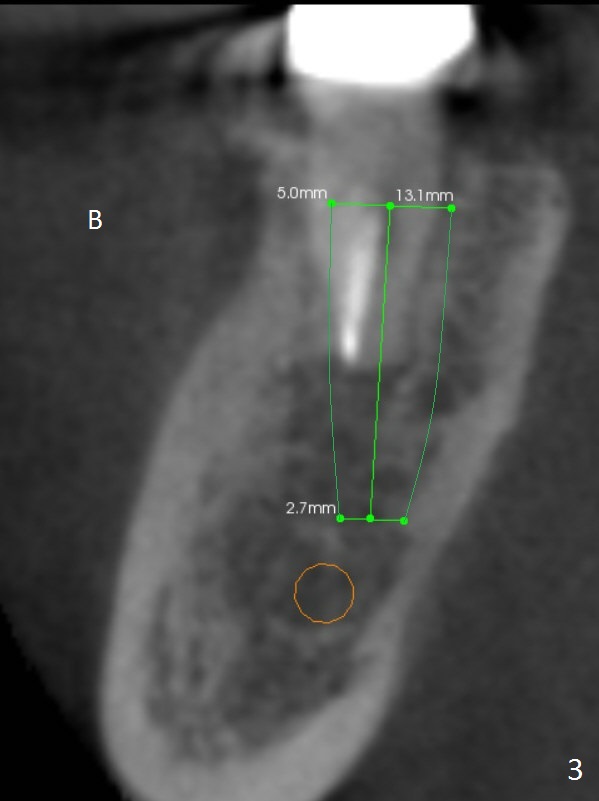
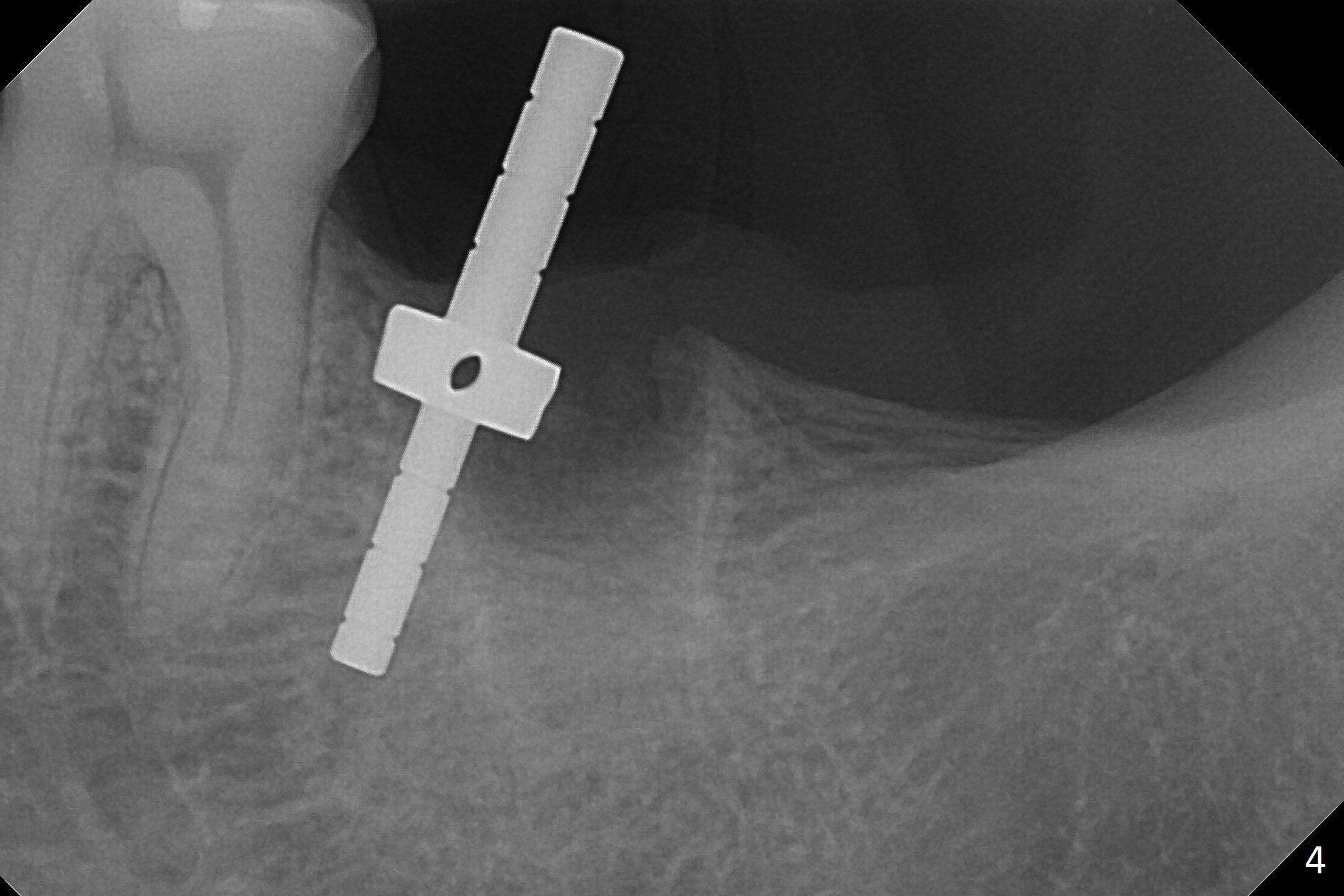
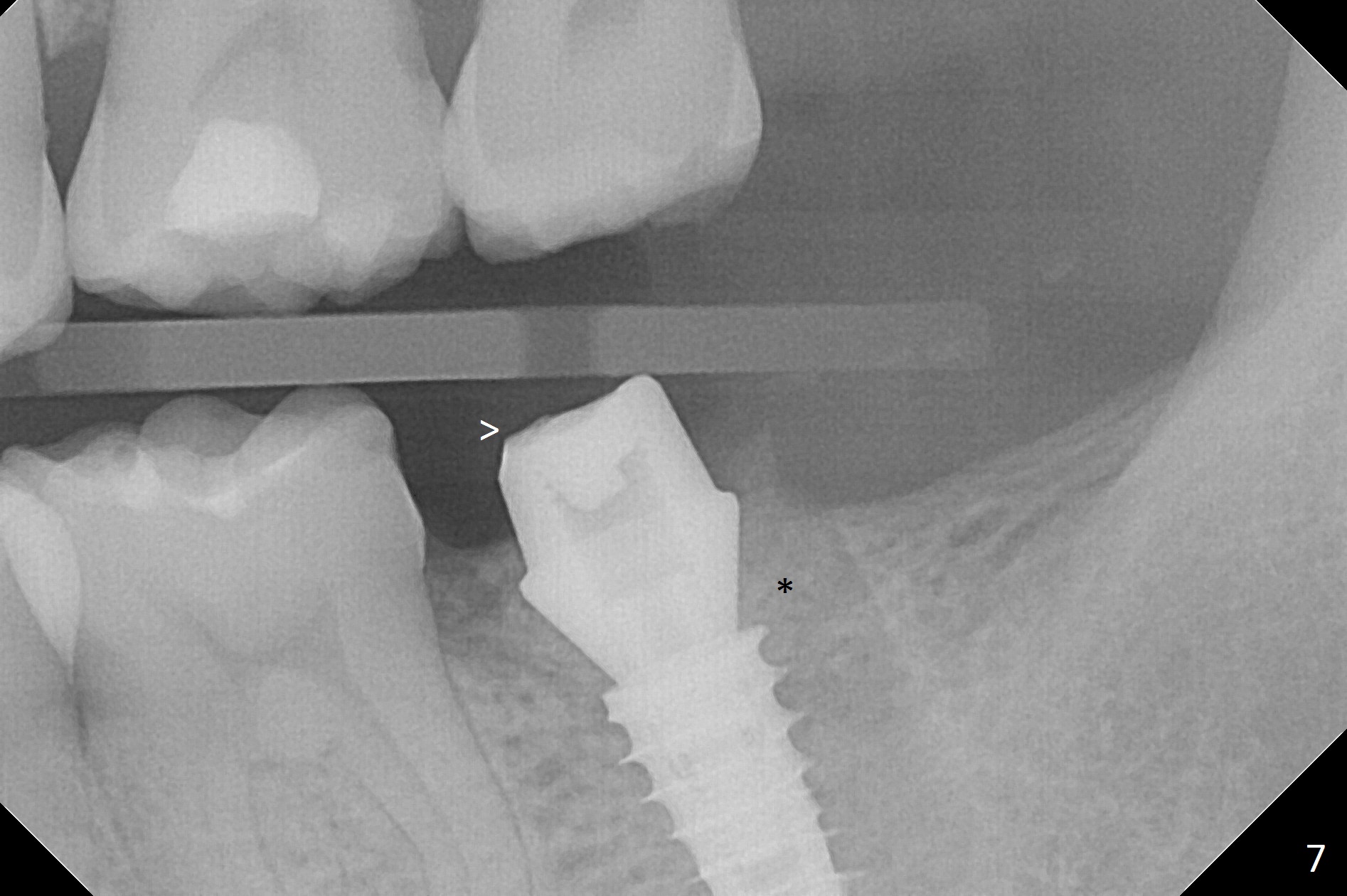
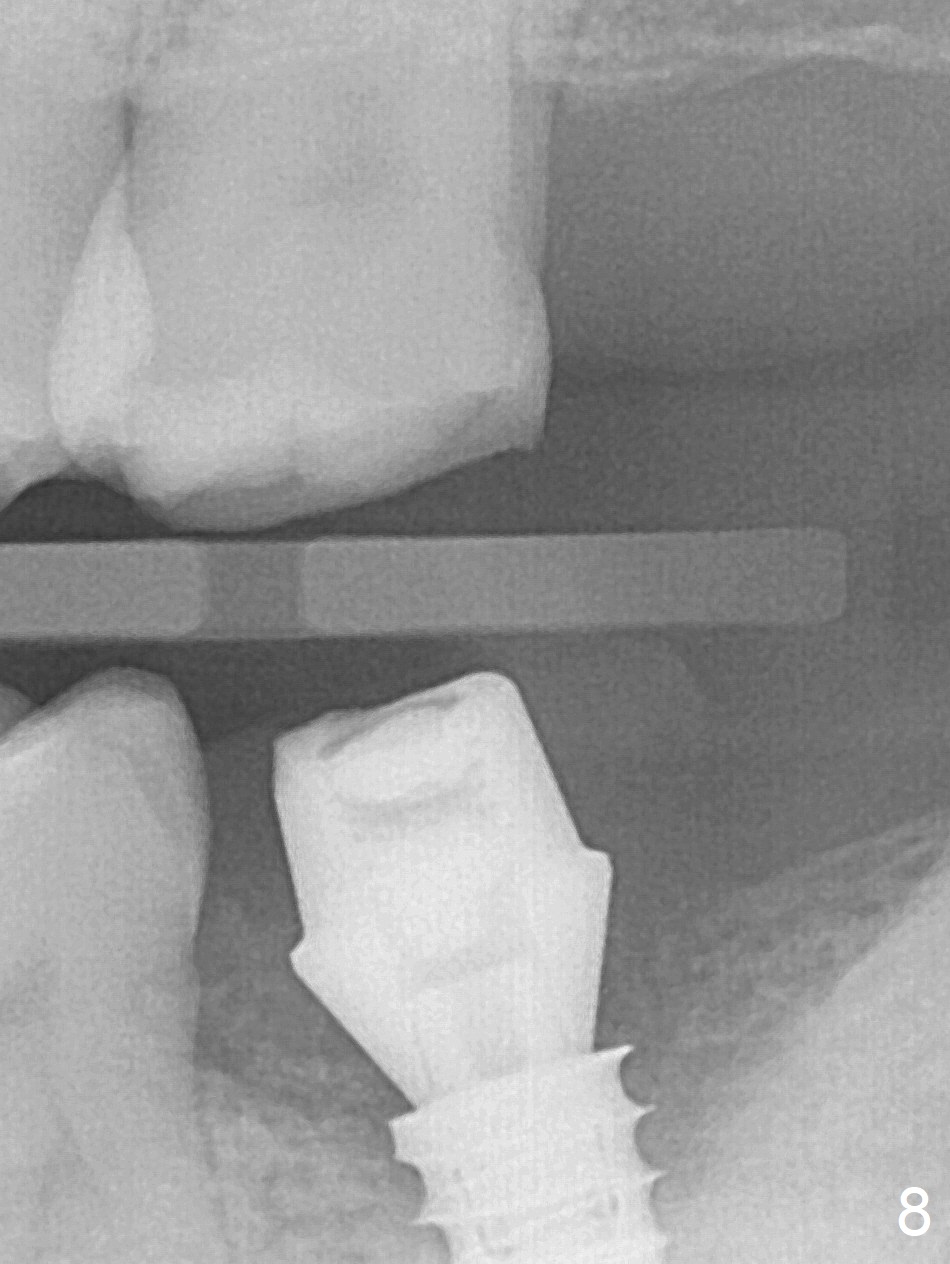
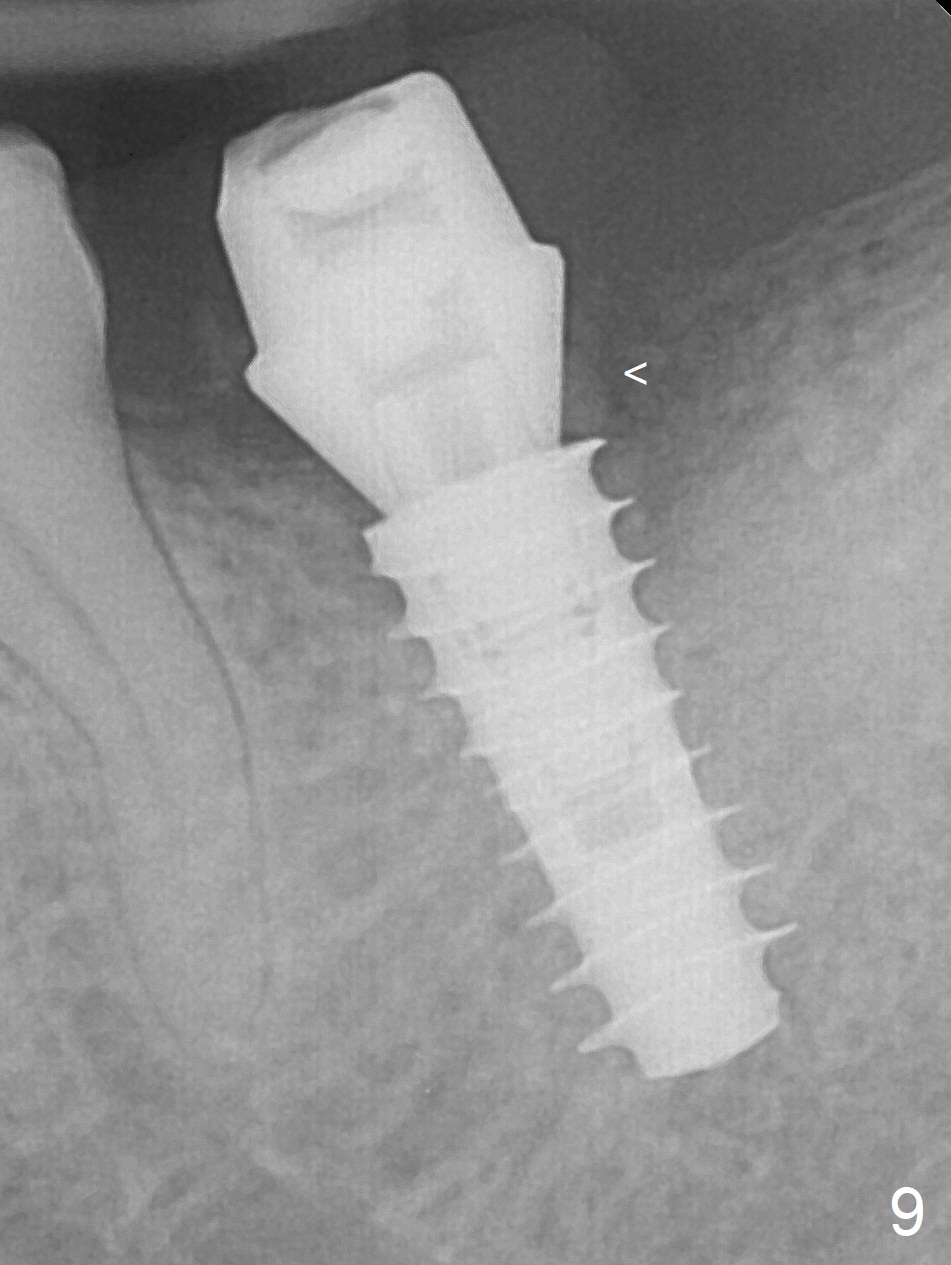
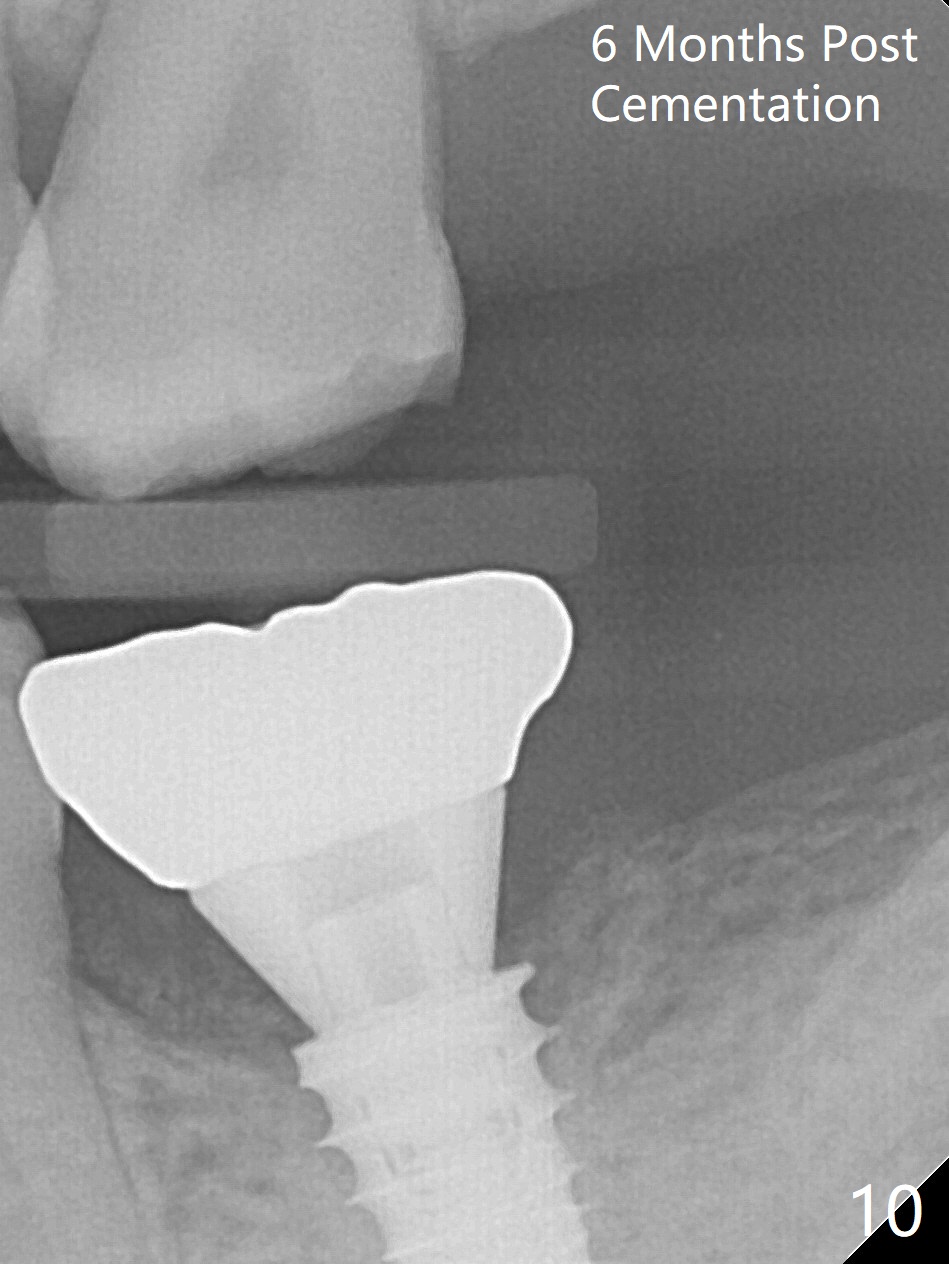
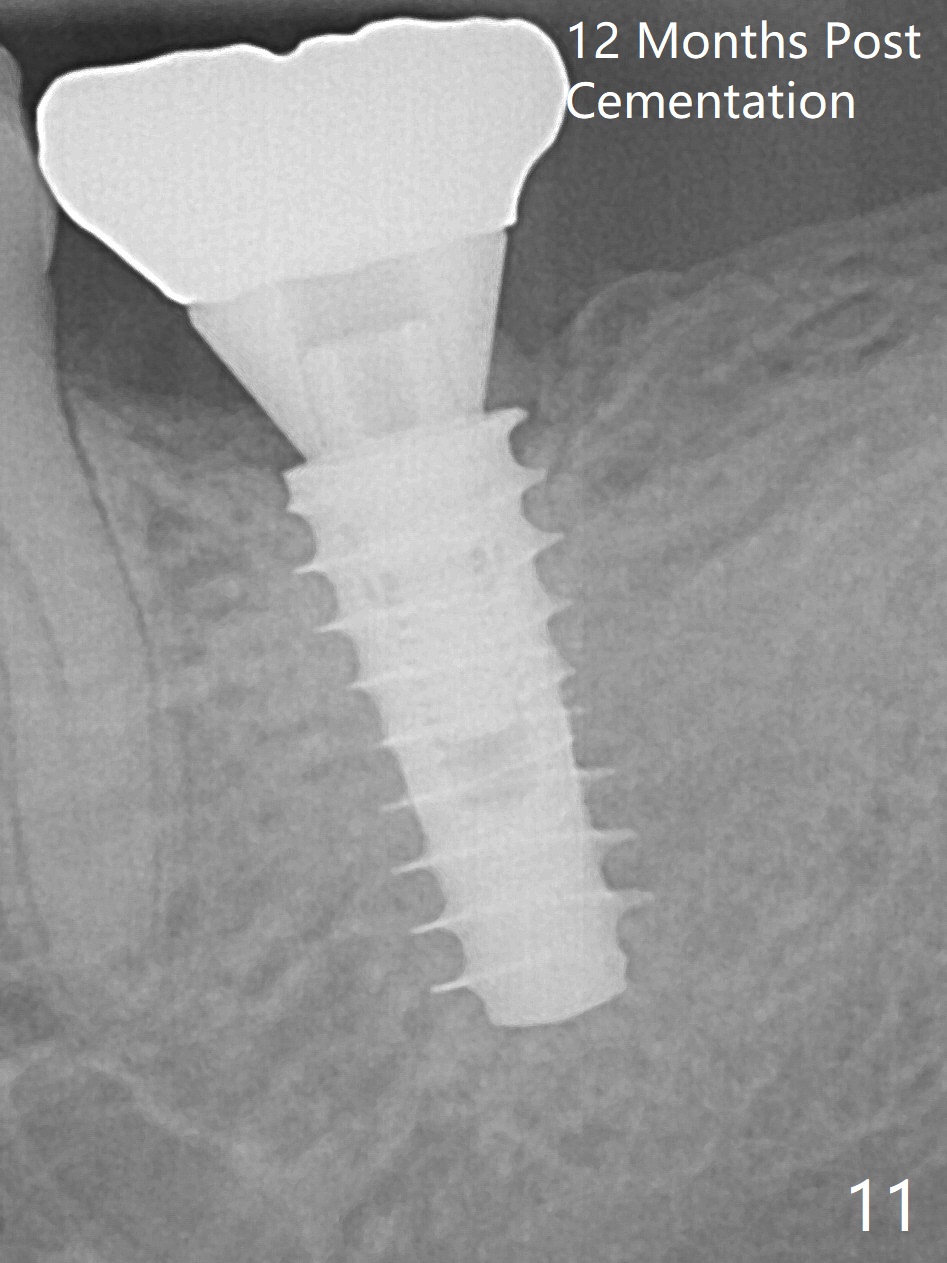
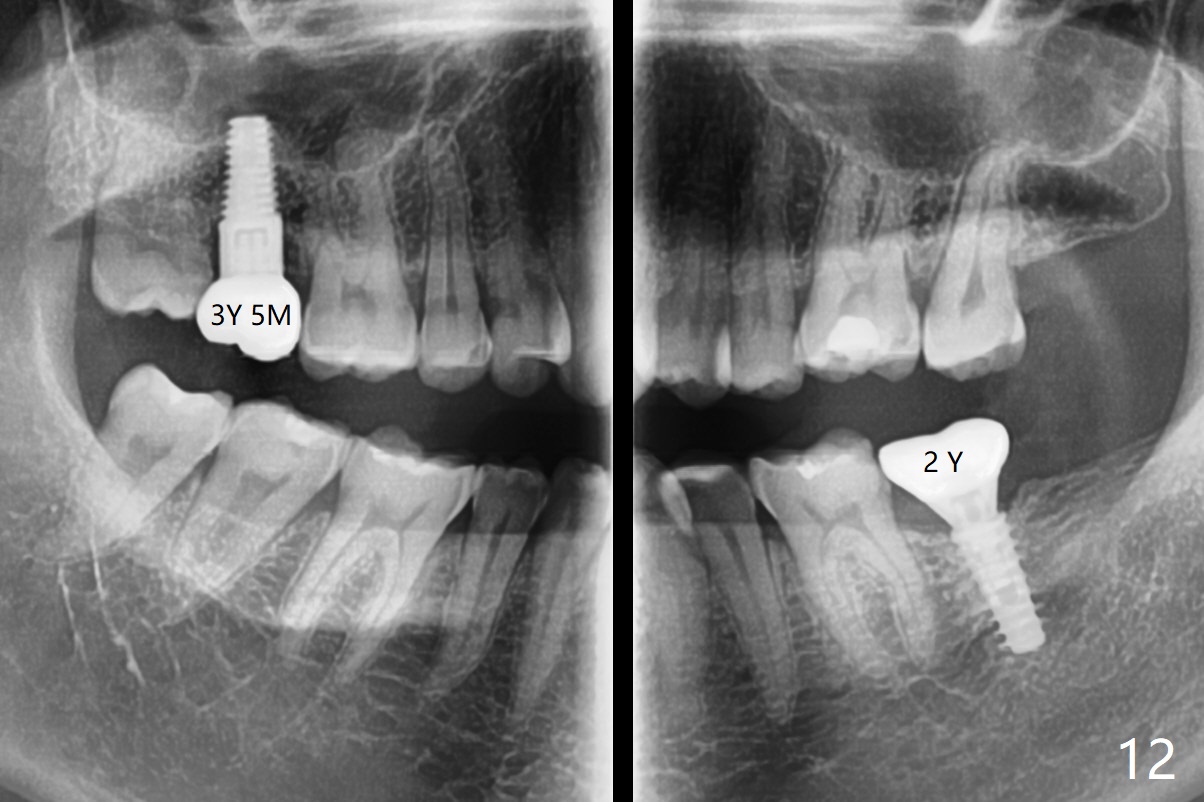
The crown at #18 dislodges; there is buccal subgingival caries (Fig.1 <). The gingiva is blanched after intraligamental injection. In fact intraop hemorrhage is substantially reduced. After extraction, the mesial slope of the socket seems to be an ideal osteotomy site (Fig.2 red line) with depth of 15 mm, as suggested by CBCT coronal section (Fig.3). The initial osteotomy with 1.6 mm drill (Fig.4 with parallel pin) needs to be moved distally with Lindamann bur. After use of 3.8 mm Magic Drill (MD), a 4x11 mm dummy implant is placed with 25 Ncm (insertion torque, Fig.5). Following 4.8 mm MD, a 5x11 mm IBS implant is placed subcrestal circumferentially (Fig.6 with 50 Ncm). A 6x4(3) mm abutment is placed. Since the vertical height is limited, the coronal end of the abutment is trimmed (Fig.7 <) for an immediate nonfunctional provisional. Three months postop, there is no bone resorption, while the bone graft seemingly remains in place (Fig.8,9 <). Bony trabecule has grown into the distal socket 6 months post cementation (10 months postop, Fig.10). Trabeculae mature in the used-to-be distal socket 12 months post cementation (17 months postop, Fig.11). In spite of this, the patient complains of mastication pain. The latter persists 2 years post cementation (Fig.12). Occlusion is adjusted.
Return to
Lower
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table)
2
Xin Wei, DDS, PhD, MS 1st edition 05/25/2017, last revision 01/07/2020