.jpg)



|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Keep 3rd Molar for Immediate Provisional Retention M
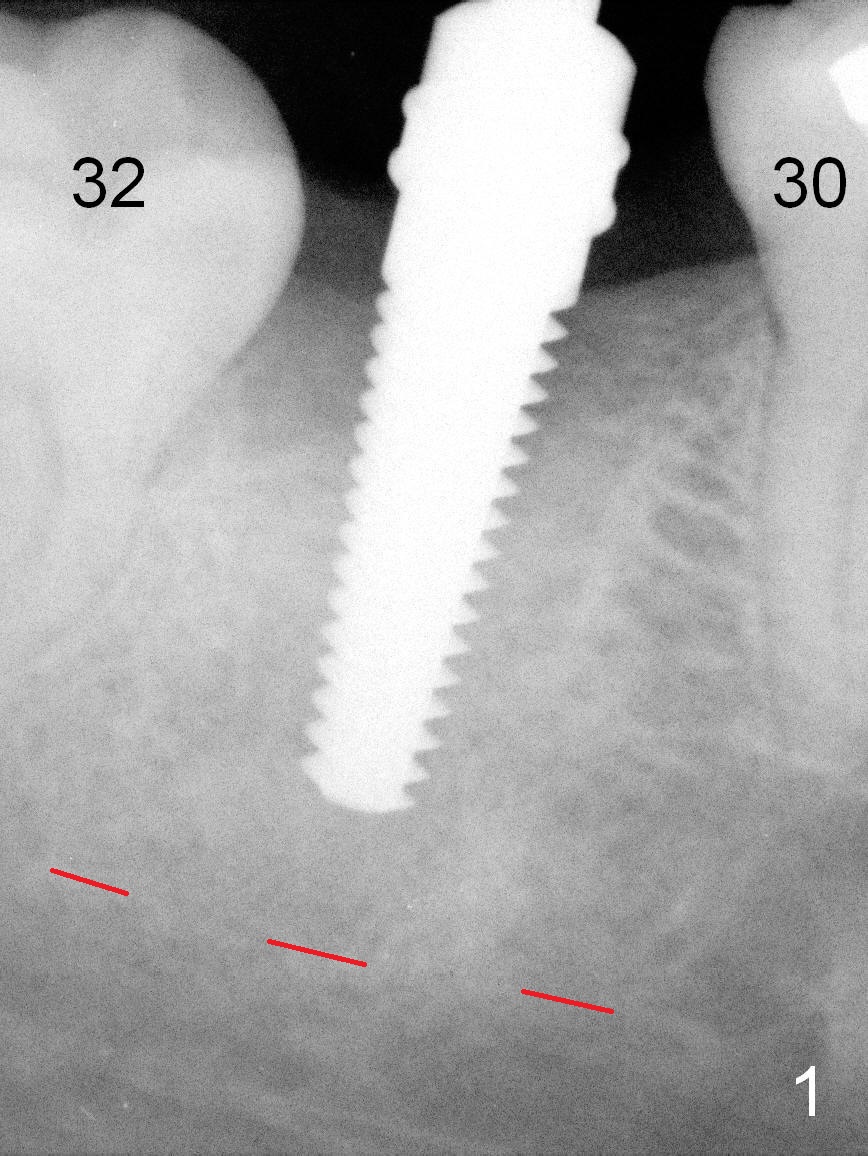
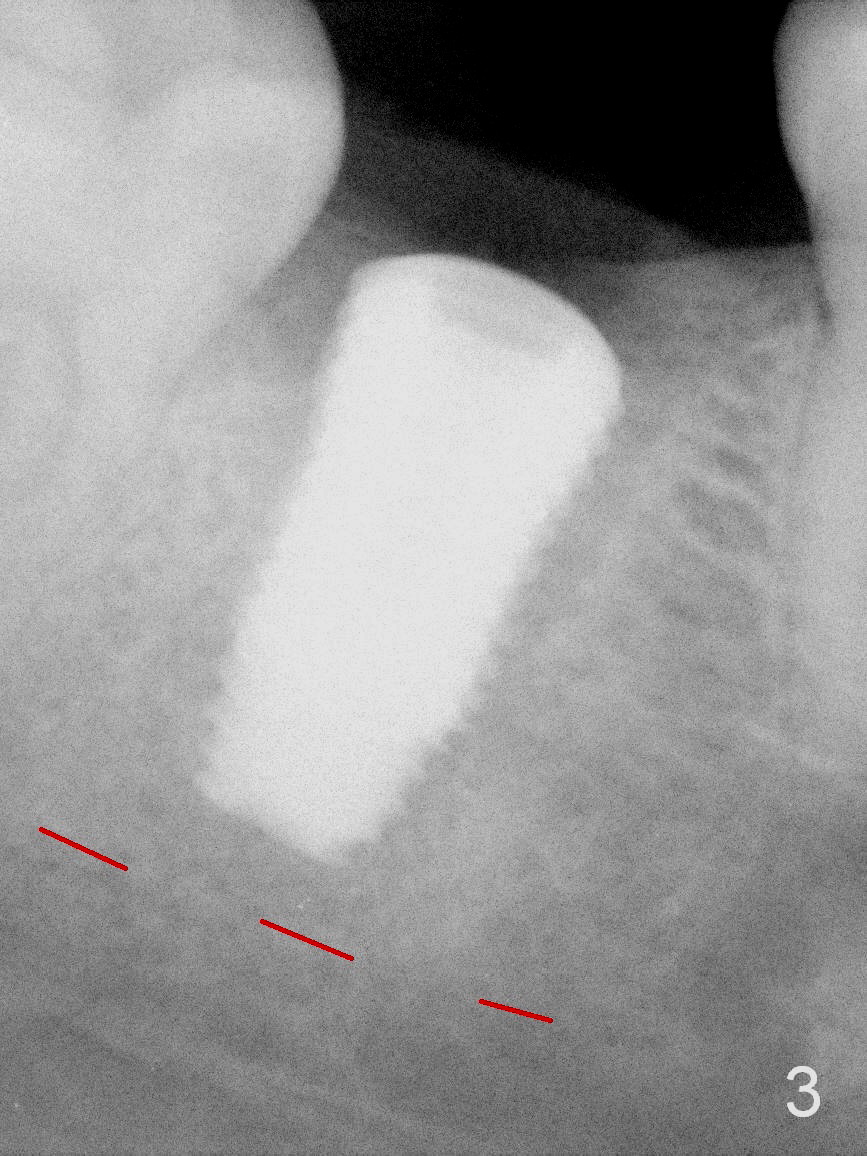
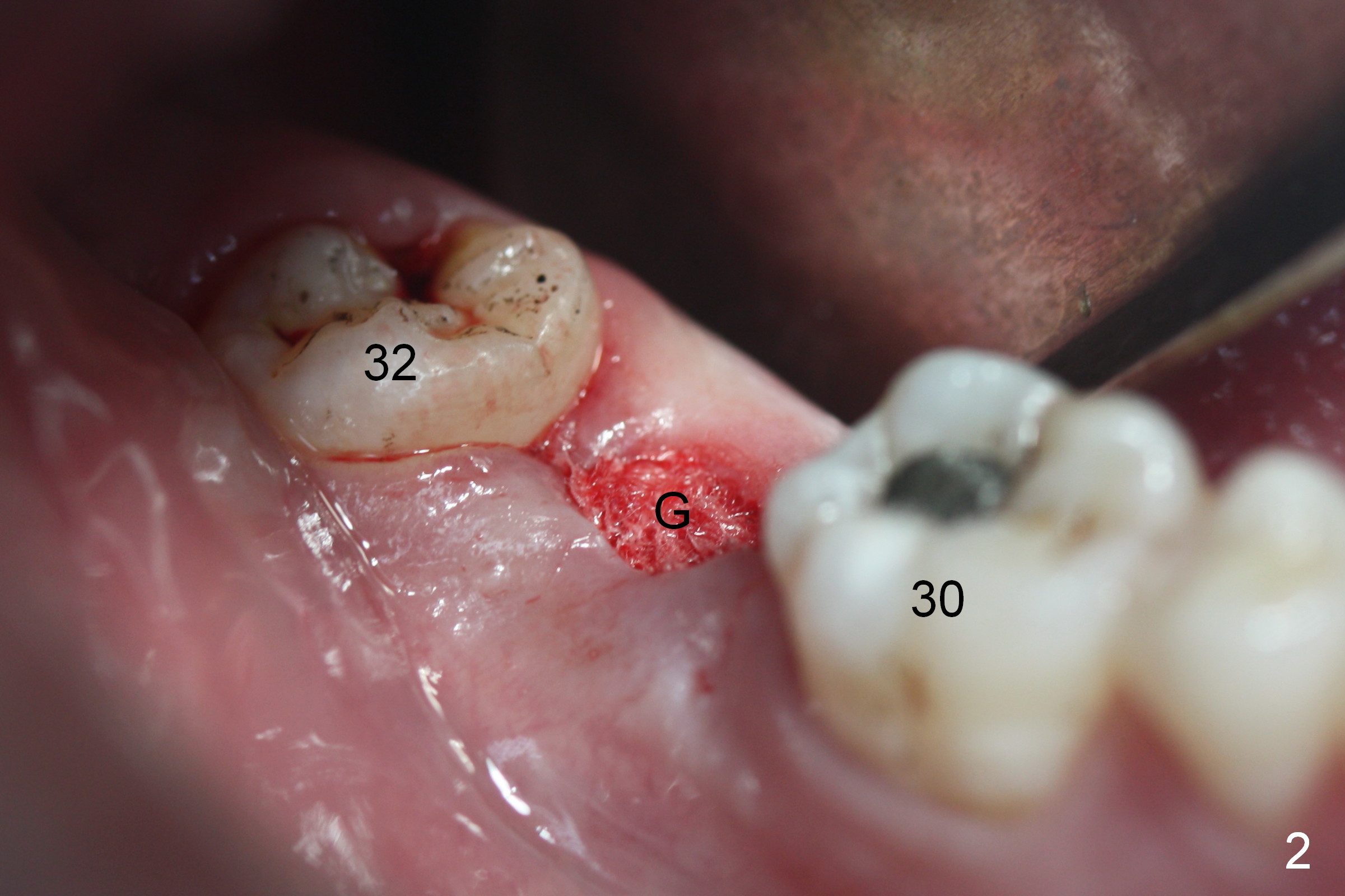
After infiltration anesthesia, the gingiva over the healing socket of #31 looks transparent and tender, 2 months post extraction. The buccal and lingual plates are intact and wide. Osteotomy is initiated by using a series of osteotomes. First, bone scalpels (4,5,6 mm) are inserted into the socket (no incision by traditional scalpel), followed by bone blades (4, 5.5 mm) and rounded tapered osteotomes (2,3 mm). The depth is 14 mm from the gingival margin. The bone expansion and condensation continues with insertion of 4.5 mm (not stable) and 5 mm (barely stable, Fig.1) taps. When a 6 mm tap is inserted, stability is acceptable. Placement of a 7 mm tap would produce satisfactory stability, but it may be too large for the mesiodistal space. A 6.5x12 mm bone-level implant is placed with insertion torque ~ 55 Ncm (Fig.3). Prior to implantation, the osteotomy site is packed with Metronidazole gauze for 3 times (Fig.2 G). No drills are used.
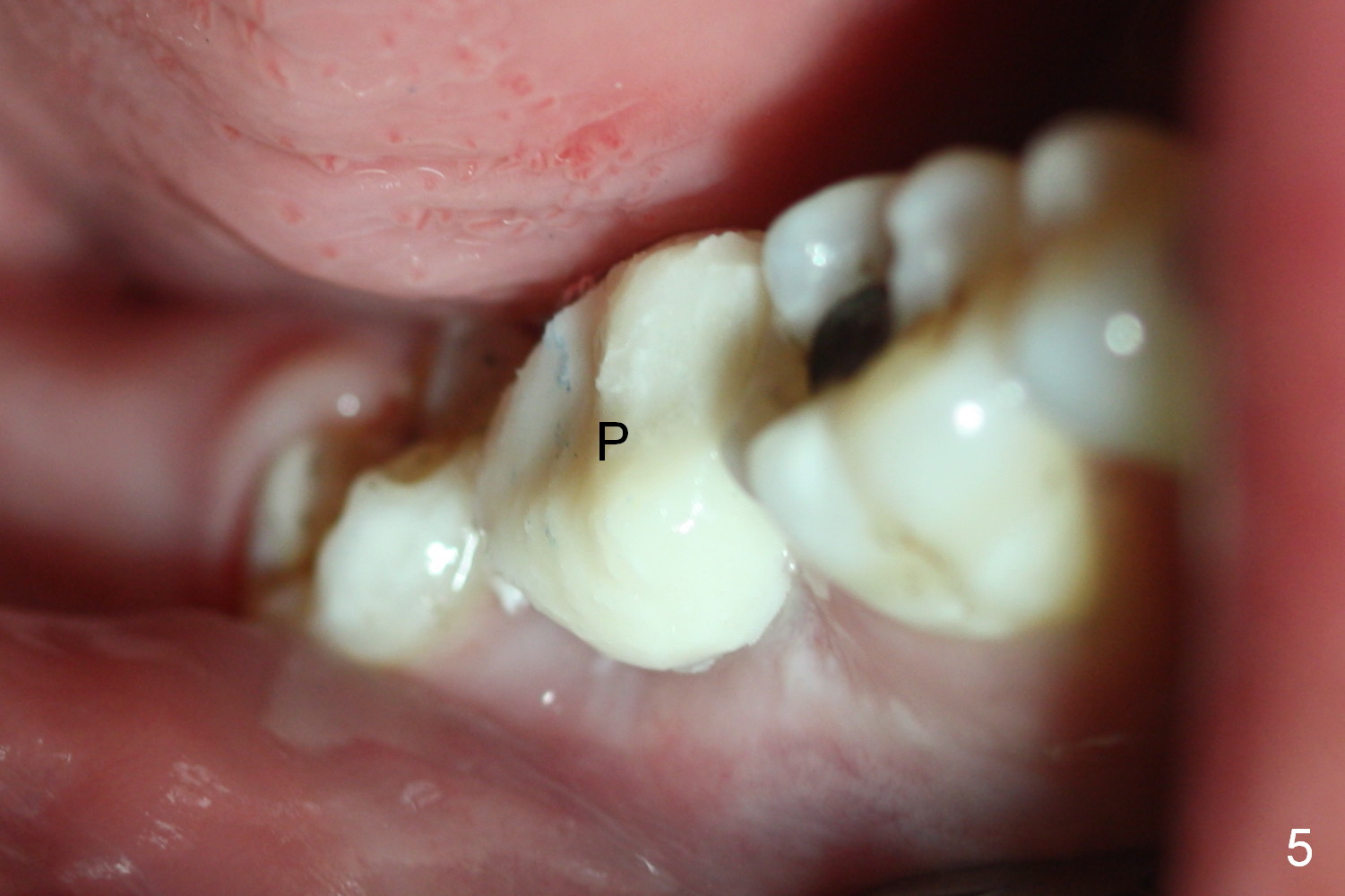
A 7.5x4(2) mm cemented abutment is immediately placed and trimmed for restorative height (Fig.4 A). Access to the osteotomy is completely closed and further protected by an immediate provisional (Fig.5 P). In fact, the presence of the 3rd molar may help retention of the provisional. The tooth may be extracted prior to and at the time of impression for the implant crown.
The patient returns for follow up asymptomatic 8 days postop. The provisional is in place without gingival inflammation (Fig.6). It is removed for lingual contour adjustment and recemented.
When the patient returns for final restoration 3 months postop (Fig.7), the provisional is lost, because of the loose abutment. The margin of the abutment is subgingival, as compared to equigingival immediately postop (Fig.4). It takes long time to expose the margin with Diode Laser. A better way may be to use a smaller diameter abutment. Expose the abutment margin with gingival retraction cords prior to abutment torque. If the margin issue is too big, change abutment.
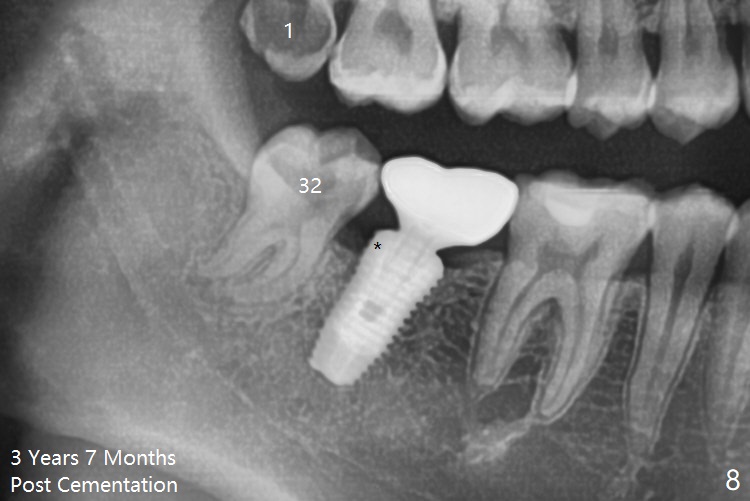
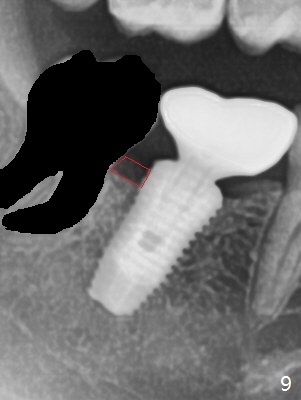
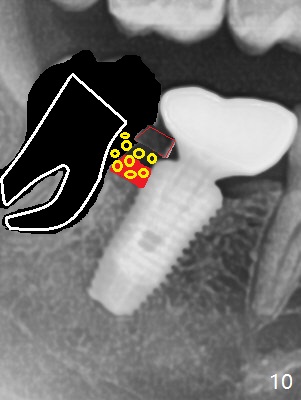
The patient also reports TMD, which may be related to malpositioned third molars. Two of them (#1,32) will be extracted when the crown at #31 is cemented. In fact the patient returns for #1 and 16 extraction 3 years 7 months post cementation (Fig.8). The distal threads seem to be exposed (*). When the tooth #32 is extracted, make envelop incision and raise the interdental papilla (Fig.9 red line) and place bone graft (Fig.10 yellow circles, Fig.11 *) after placement of Osteogen plug in #32 socket (Fig.10 white outline, Fig.11 O). In fact hockey stick incision starts in the mesial of #31 for easy access to the implant.
Return to
Lower Molar Immediate Implant,
Posterior Immediate Provisional
Plug
Allograft
Xin Wei, DDS, PhD, MS 1st edition 08/20/2015, last revision 12/25/2019