
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
It Does not Look Too Large
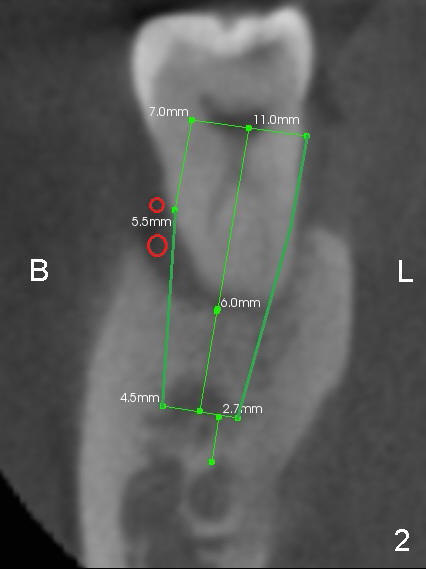
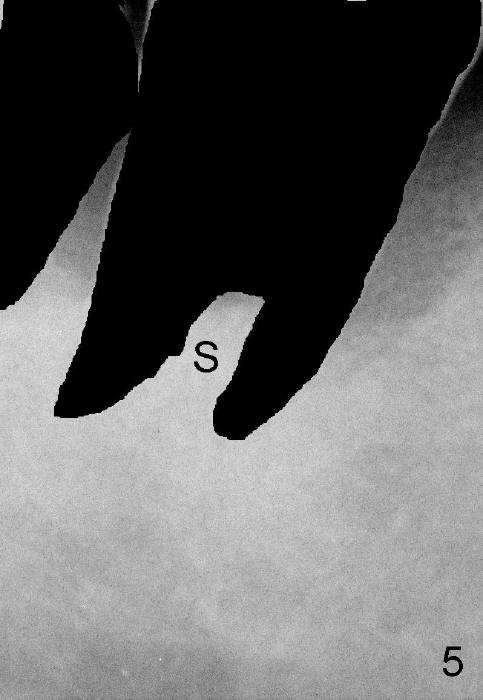
The tooth #31 of a 41-year-old man appears to have combined periodontitis and occlusal trauma: severe mesial bone resorption (Fig.1 (CT sagittal section),Fig.4 (PA)). In fact, the tooth #32 was extracted when a 5x17 mm implant was placed at the site of #30 (Fig.4).
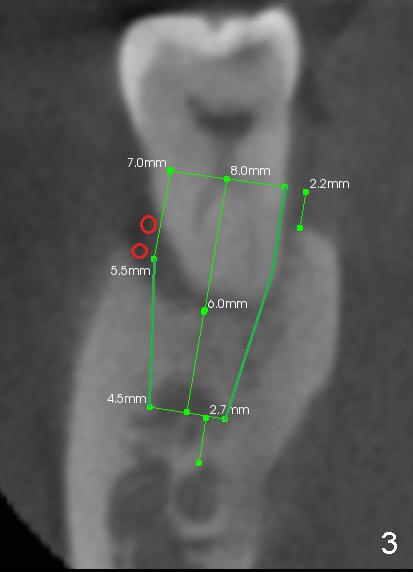
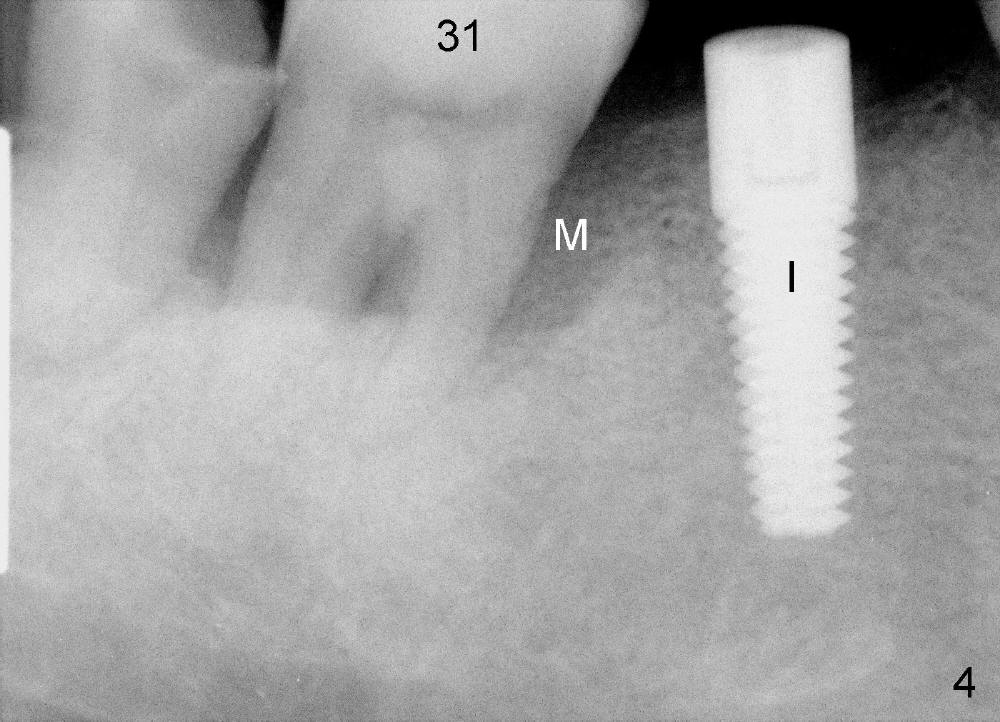
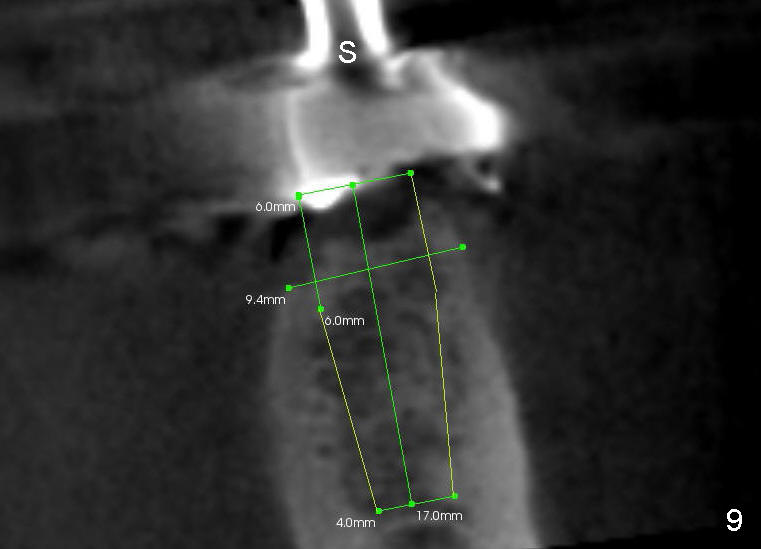
CT coronal sections at the mesial root of #31 show that a 7x17 (Fig.2) or 7x14 mm (Fig.3) implant does not look too large for the alveolar bone buccolingually. The large implant is able to help close the large socket (mesial (Fig.1,4) and buccal (Fig.2,3) aspects), reducing the amount of bone graft (red circles) placed. In contrast, the buccolingual width of #30 is narrower (Fig.9 CT coronal section), allowing a smaller implant (6x17 mm by design (Fig.9), 5x17 mm clinically (Fig.4)).
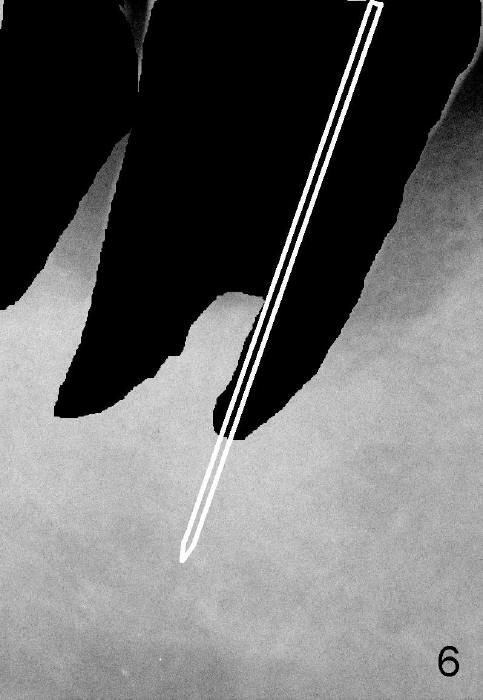
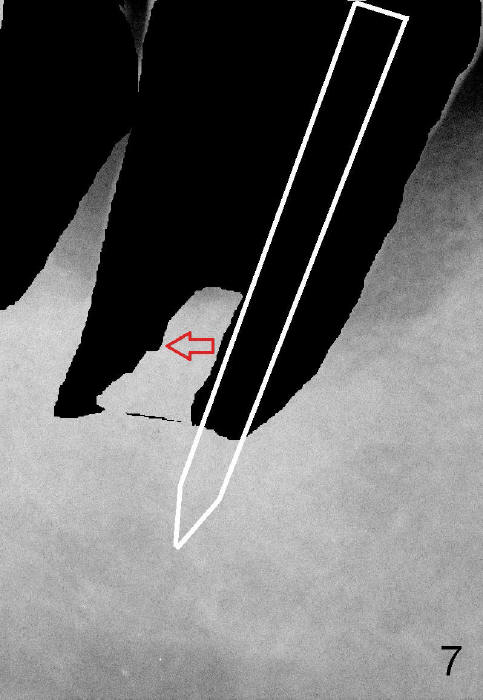
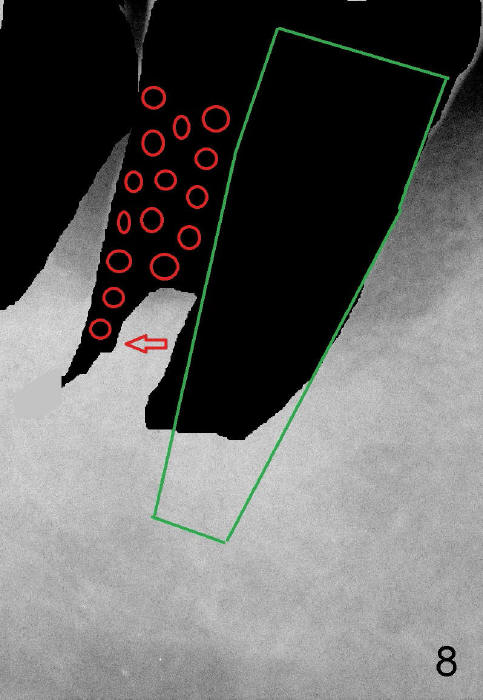
In brief, a large implant is to be placed in the mesial socket of #31. In order to increase primary stability and save autogenous bone (septal bone (Fig.5 S, drawing from Fig.4 after extraction), a pilot drill is used to start osteotomy in the mesial socket (Fig.6 white lines), followed by insertion of osteotomes (Fig.7 white lines, combined with drills). The latter are mainly used to push the septum distally (red arrow). By the time a large implant is placed (Fig.8 green lines), the septum is further pushed distally (red arrow). The remaining distal socket is then filled with bone graft (red circles). How does the surgery end up with?
Return to
Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 10/11/2014, last revision 02/17/2015