












|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Severe Supraeruption
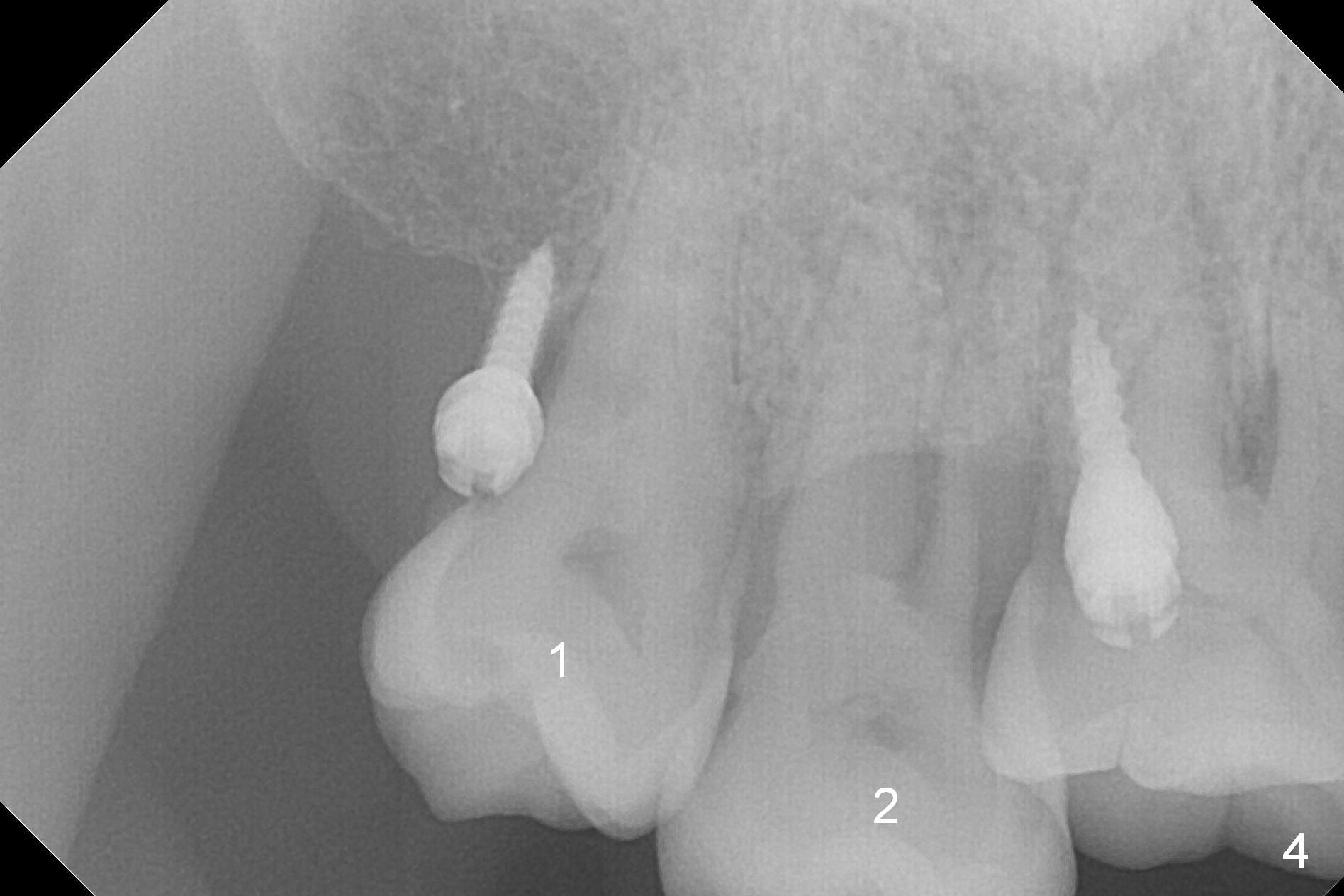
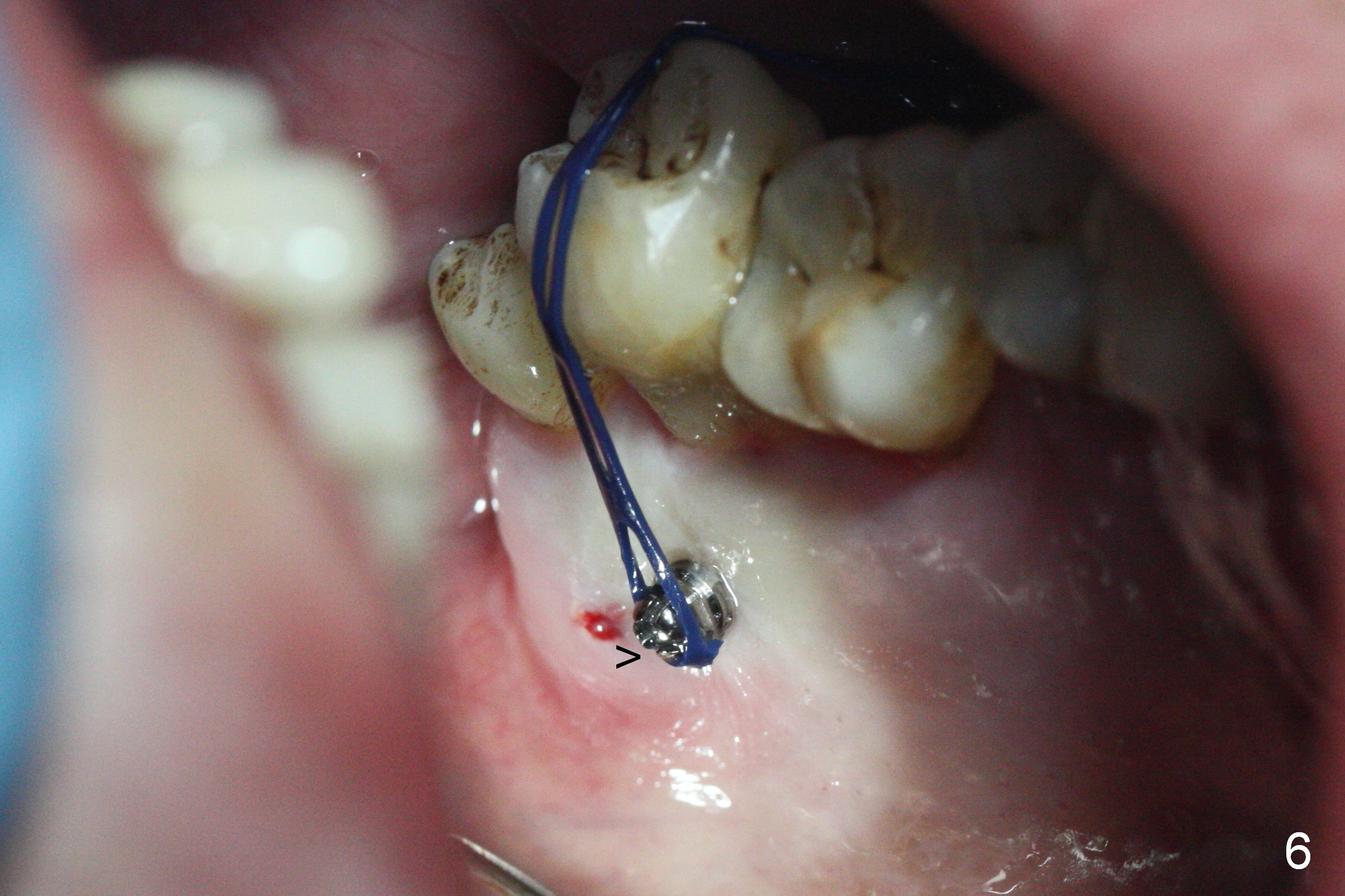
Two days post #31 implant placement, the patient returns for orthodontic intrusion of the tooth #2 with mini-implants (Fig.1). The palatal cusps have been trimmed (Fig.2 ^), since they almost contact a healing abutment at #31(*, Fig.3). Two mini-implants are to be placed mesiobuccal and distopalatal to the affected tooth. After minimal injection of Lidocaine, a 1.6x6 mm Tomas implant is placed in full length mesially (Fig.4), while the other (1.6x8 mm) half way (Fig.4). Following change in implant site mesially (Fig.6 >), the implant is half inserted (Fig.5). It appears that the tip of the distal implant is toward the tooth #1 (Fig.5). After withdrawing the implant partially, it is re-directed to apparently ideal trajectory (Fig.7). Ideally the mesial implant (Fig.8) should have been placed partially initially (Fig.4,5,7) so that the trajectory could have been able to be changed.
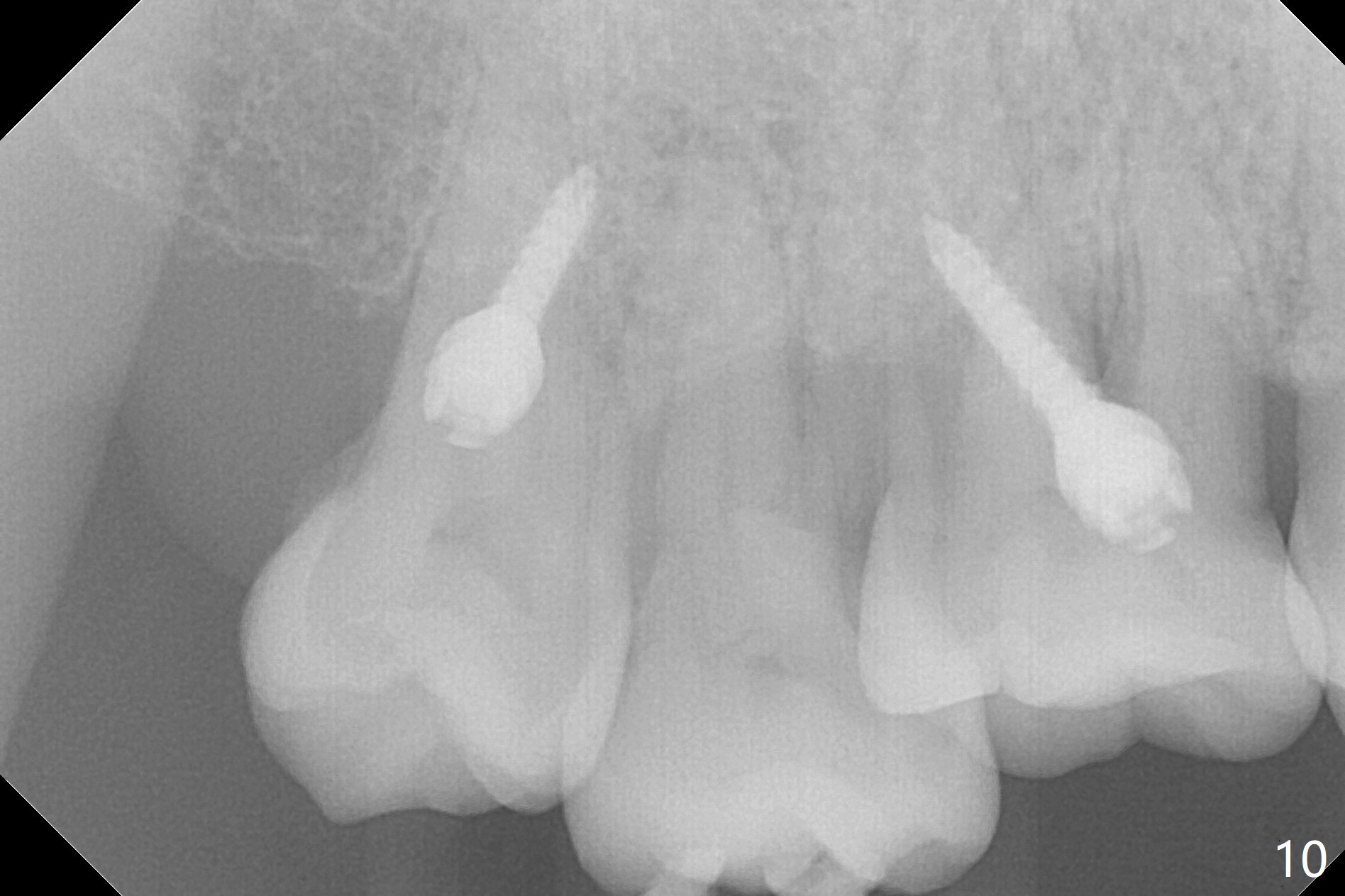
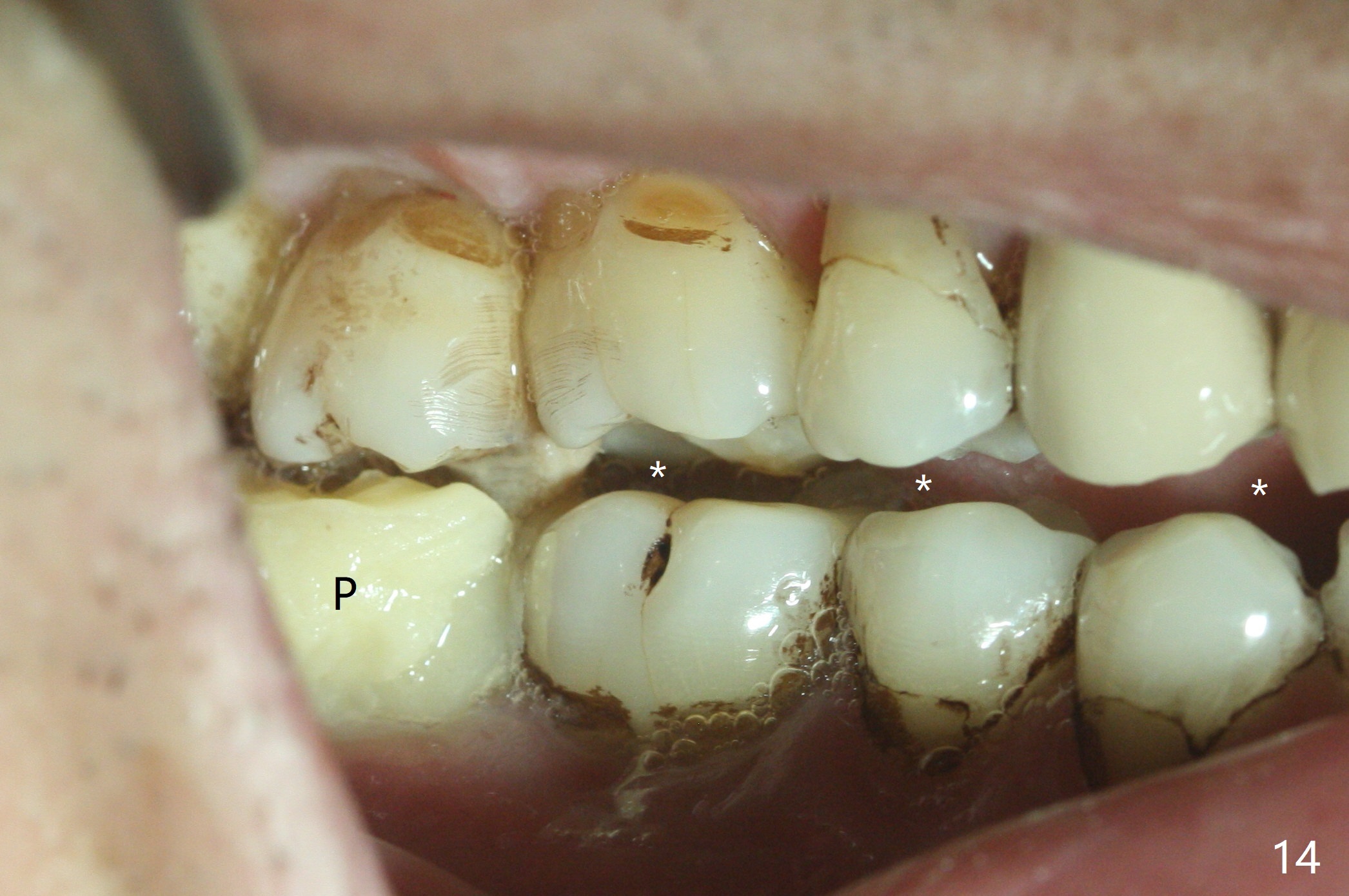
The buccal implant becomes loose in 2-3 months. When the wound heals (Fig.9 <), a 1.6x`10 mm implant is placed with the help of PAs for trajectory (Fig.10,11) and in the nonkeratinized gingiva (higher, the crestal bone may have been traumatized by previous implant placement, Fig.12). Two months later, the tooth #2 is partially intruded (Fig.13). A provisional (Fig.14 P) is fabricated in the osteointegrated implant at #31 with supraocclusion so that the remaining dentition has no occlusal contact (*). The periodontally compromised tooth #2 becomes in buccoversion in 2 months. The provisional is removed, while a lingual button is placed in the buccal surface of the tooth #2 (Fig.15). With power chain attached to the lingual mini-implant, the tooth #2 is lingualized in 2 months. The provisional and the implants are reused for final intrusion (Fig.16). The treatment is nearly 11 months. The buccal implant, although placed in the movable mucosa, remains stable and healthy (Fig.17). The tooth #1, as a guiding plane (to prevent #2 from distalization during intrusion), is not extracted after intrusion is completed.
Return to
Implant & Ortho
2 IBS
Xin Wei, DDS, PhD, MS 1st edition 03/17/2017, last revision 04/29/2018