,%205.8x5.5(4.5)%20abutments,%20bone%20graft.jpg)



|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Thick Gingiva, Long Abutment Cuff
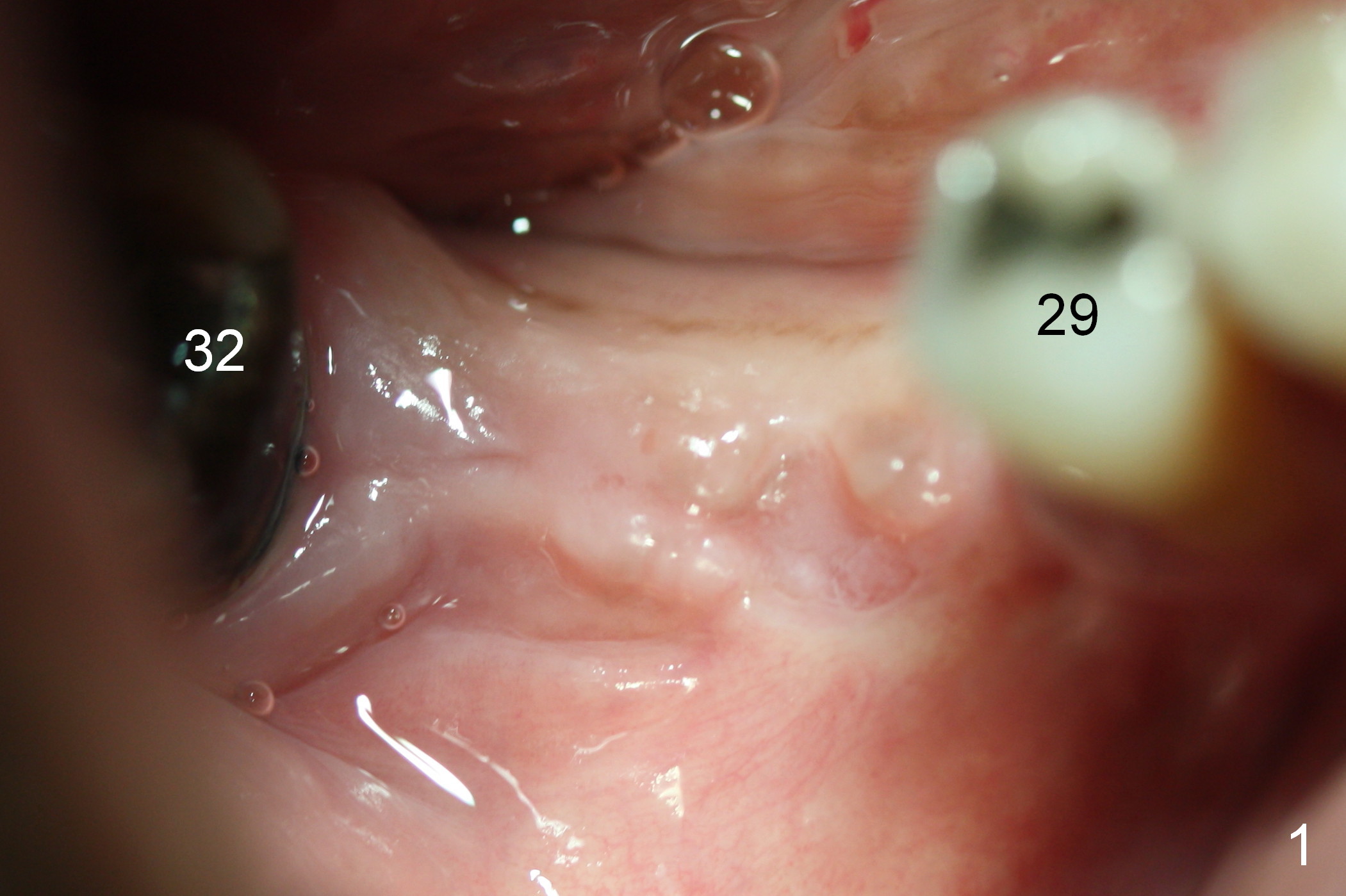
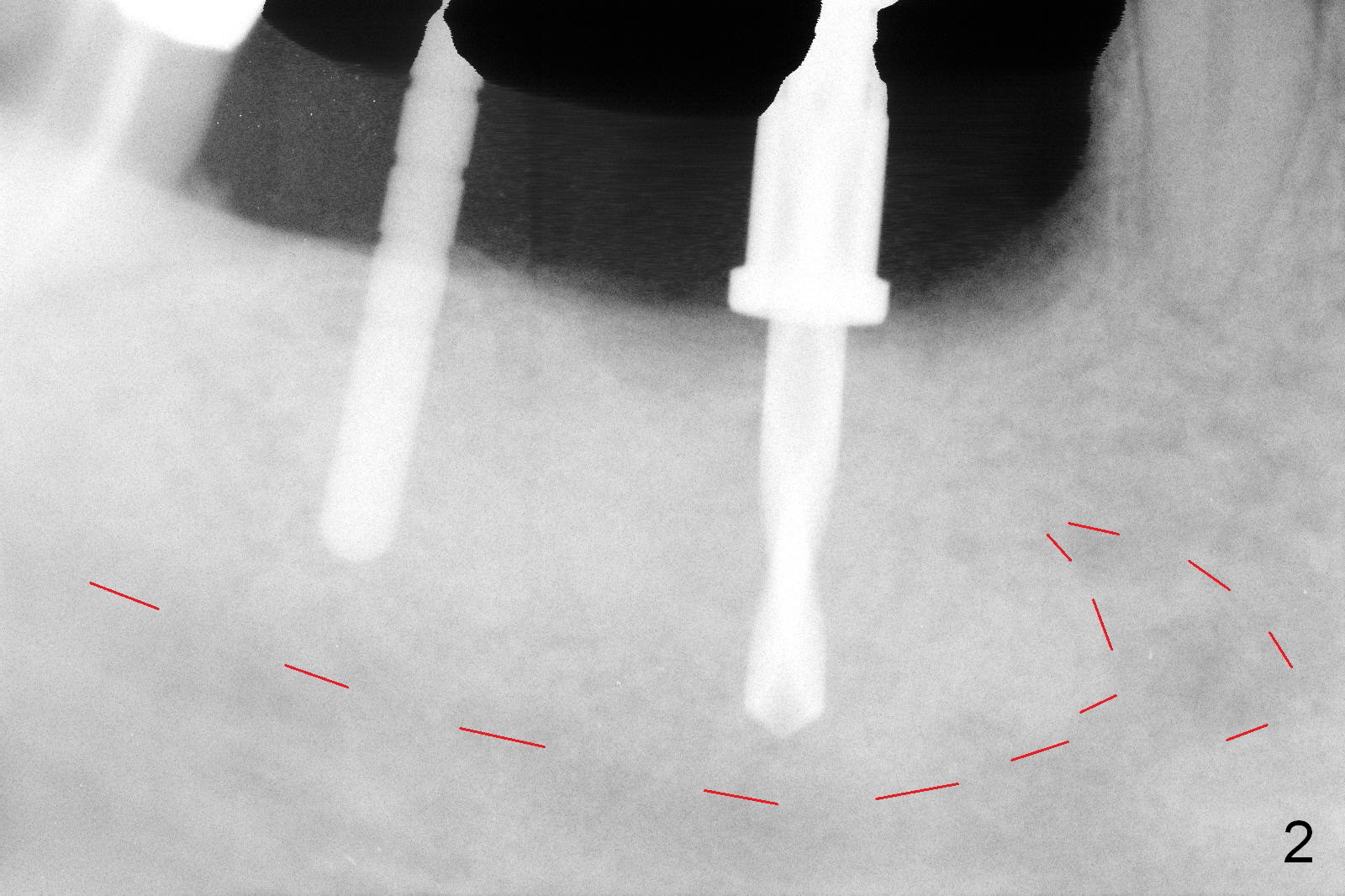
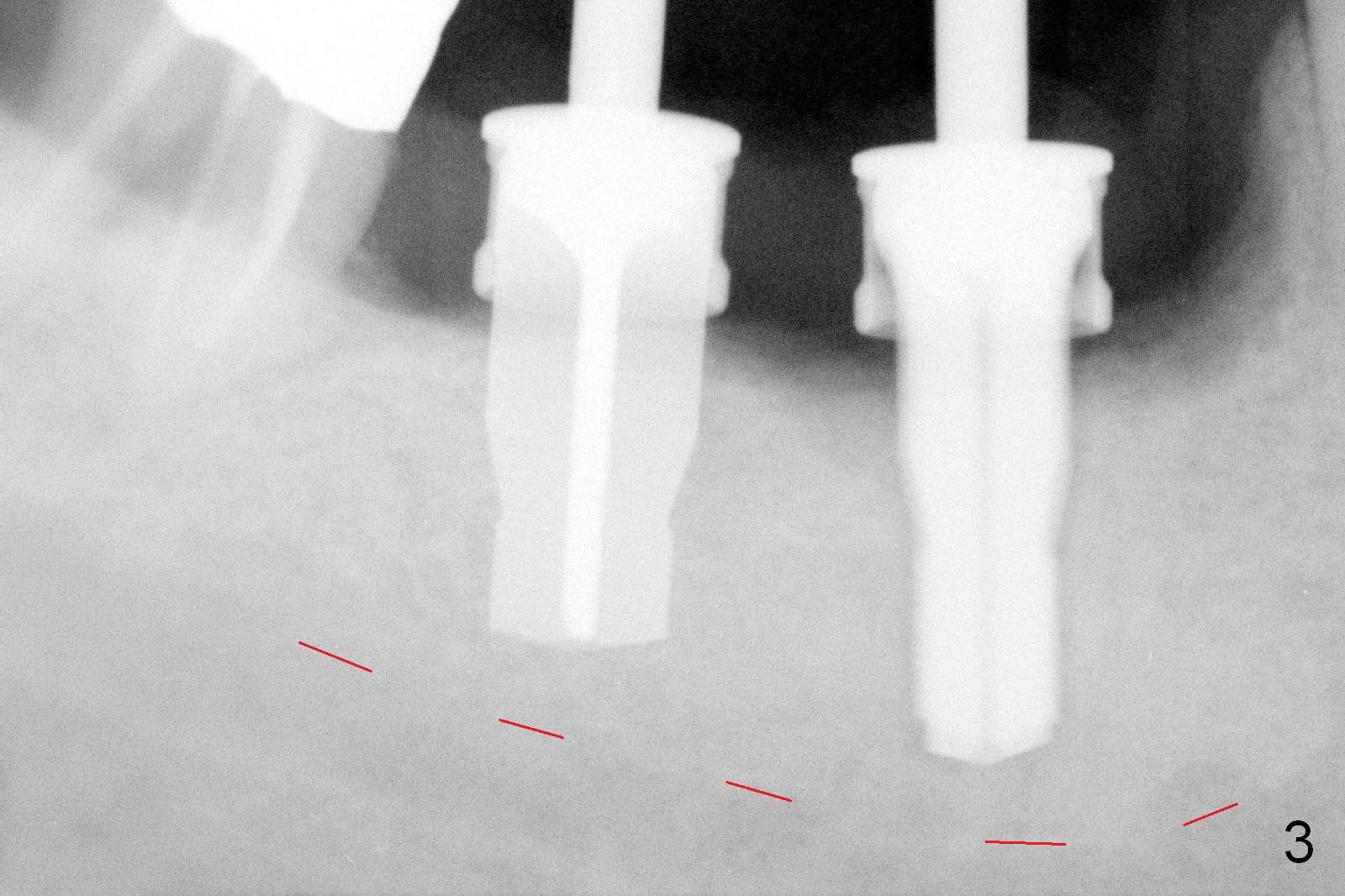
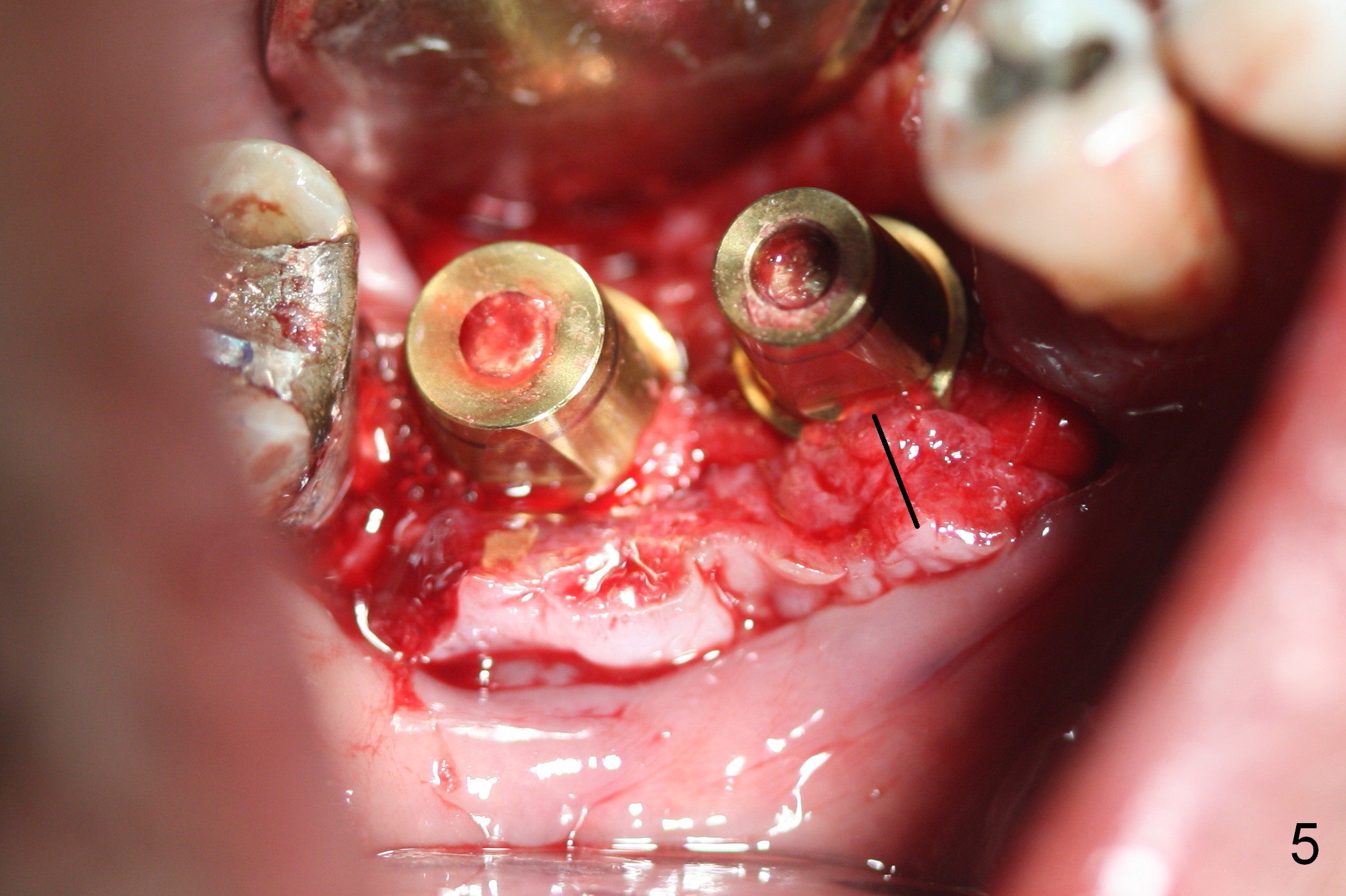
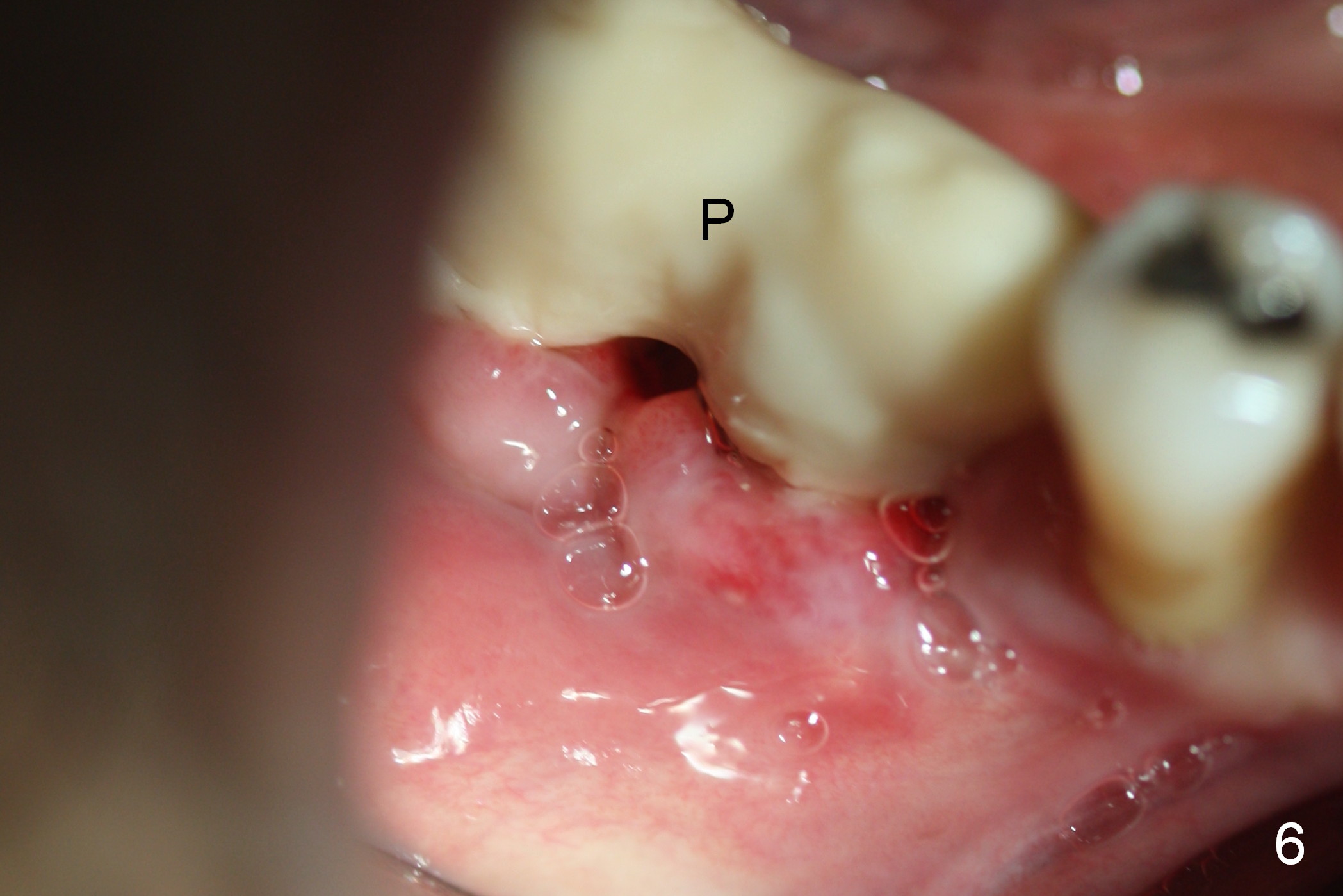
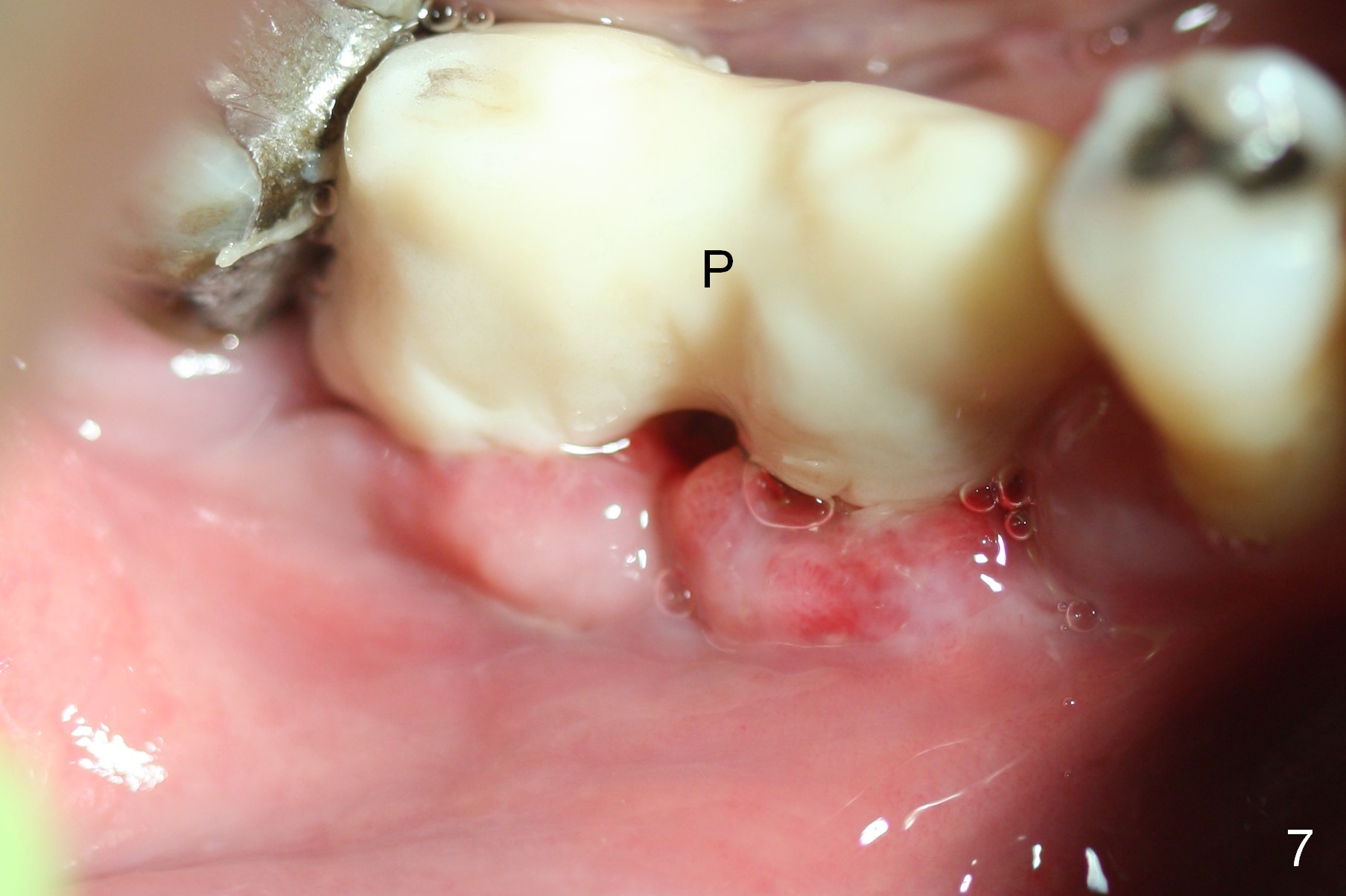
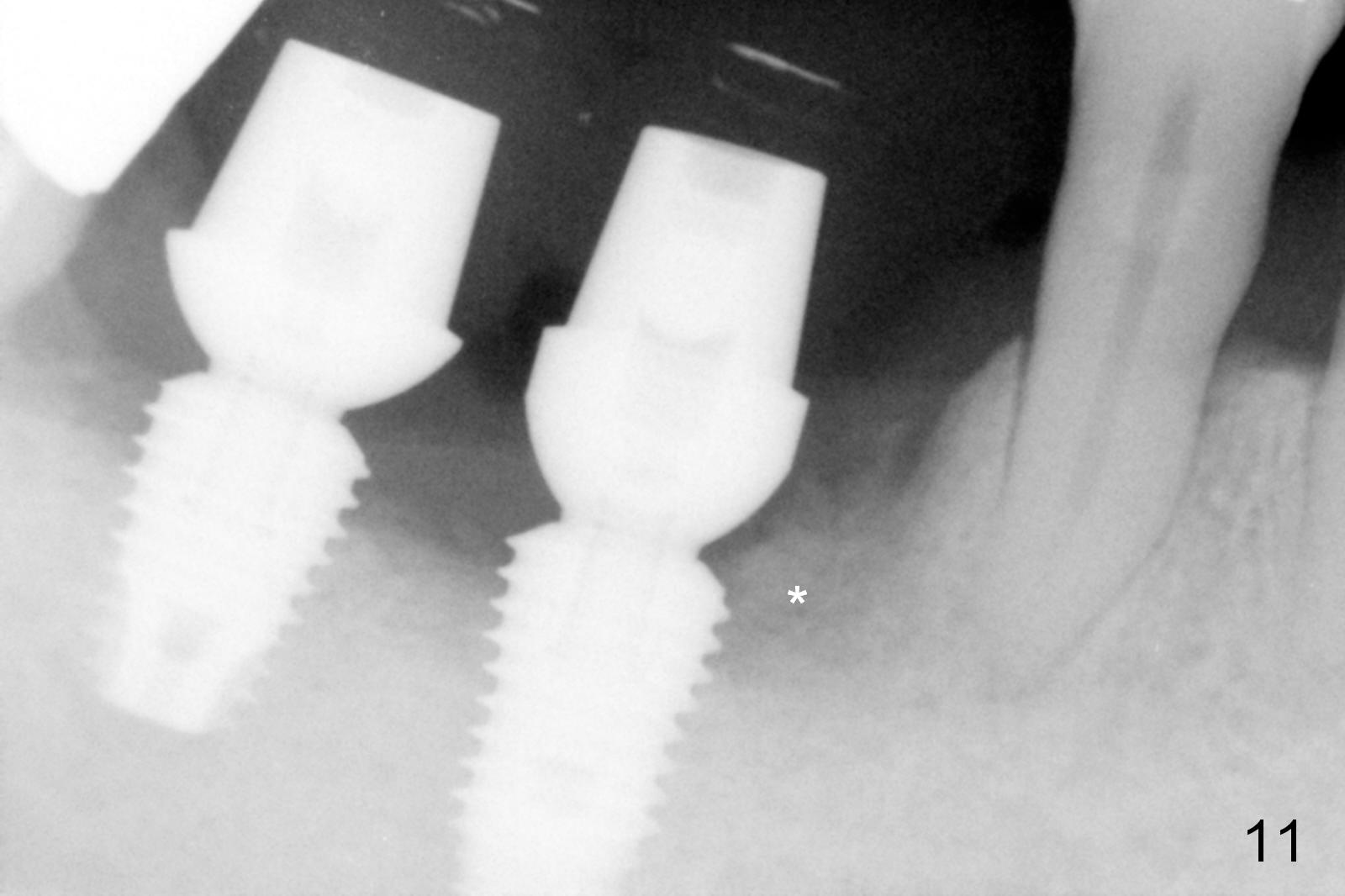
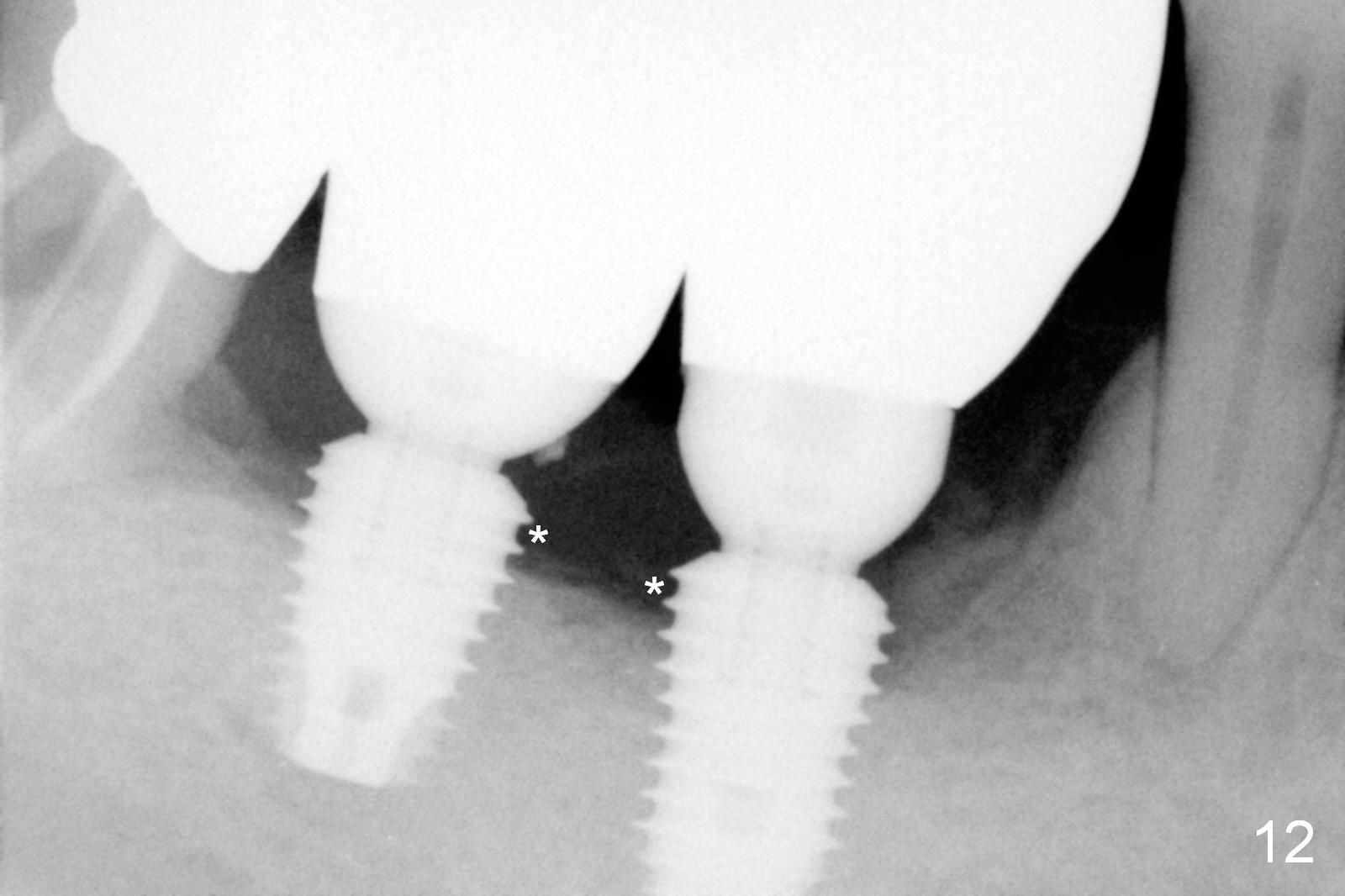
The patient cuts down smoking preop (~1.5 ppd). Clinically, the edentulous ridge at #30 and 31 looks wide (Fig.1). The depth of initial (Fig.2) and final (Fig.3) osteotomies is controlled at 10 and 8 mm, respectively (red dashed line: the superior border of the Inferior Alveolar Canal). Two implants (Fig.4: 5.9x10, 5.9x8 mm) are not seated completely due to high bone density. Bone graft (*) is placed to cover the denuded threads. Long abutment cuffs (4.5 and 3 mm) have to be used (Fig.4) because of thick gingiva (Fig.5 black line). An immediate splinted provisional is cemented before suturing and perio dressing. The patient reports swelling the first few days postop. When he returns 8 days postop, there is mild pain, accompanied by buccal gingival erythema and edema (Fig.6,7,8 (P: provisional)). He has not smoked postop. Probably 2 stage technique should have been adopted for the heavy smoker. Thick gingiva appears to be a feature of patients with chronic periodontitis. The gingiva heals well around the implants/abutments/splinted crowns well 2 months postop. He is ready for #14,15 implant placement (Fig.9,10: 2.5 months postop). There appears to have bone growth mesial to #30 implant 5 months postop (Fig.11 *). The final restorations are delivered 9 months postop (Fig.12, temp bond). It appears that the most coronal threads of the implants are uncovered by the bone. These two implants should have been placed deeper (all of the threads buried) to reduce possibility of periimplantitis. Shorter implants should have been chosen.
Return to Lower Molar Immediate Implant,
Posterior Immediate Provisional,
Systemic Diseases
Xin Wei, DDS, PhD, MS 1st edition 08/23/2015, last revision 05/18/2016