,%206.8x4(3).jpg)

|
|
|
|
|
|
|
|
|
|
New Sensor and Its Holder
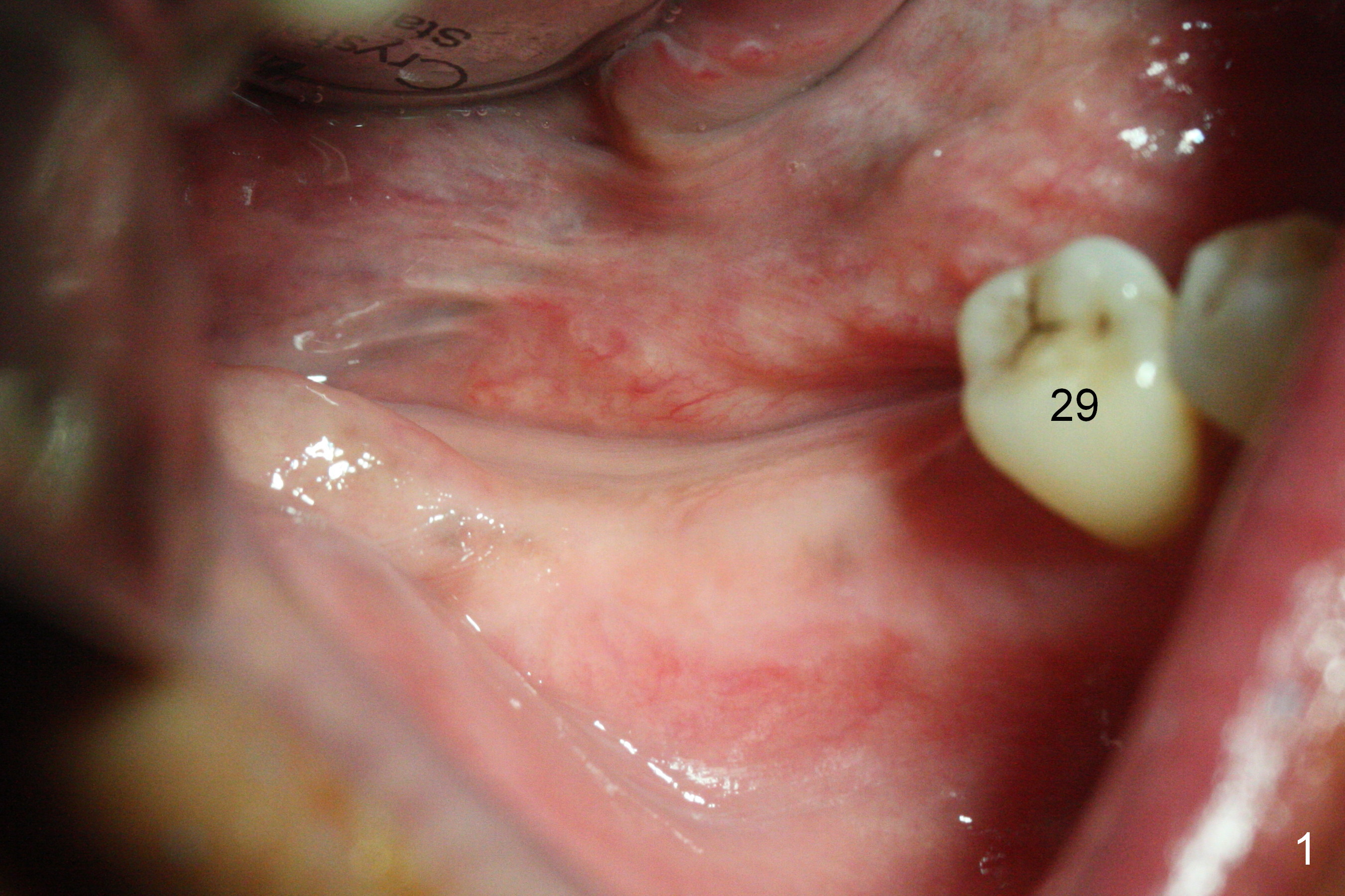
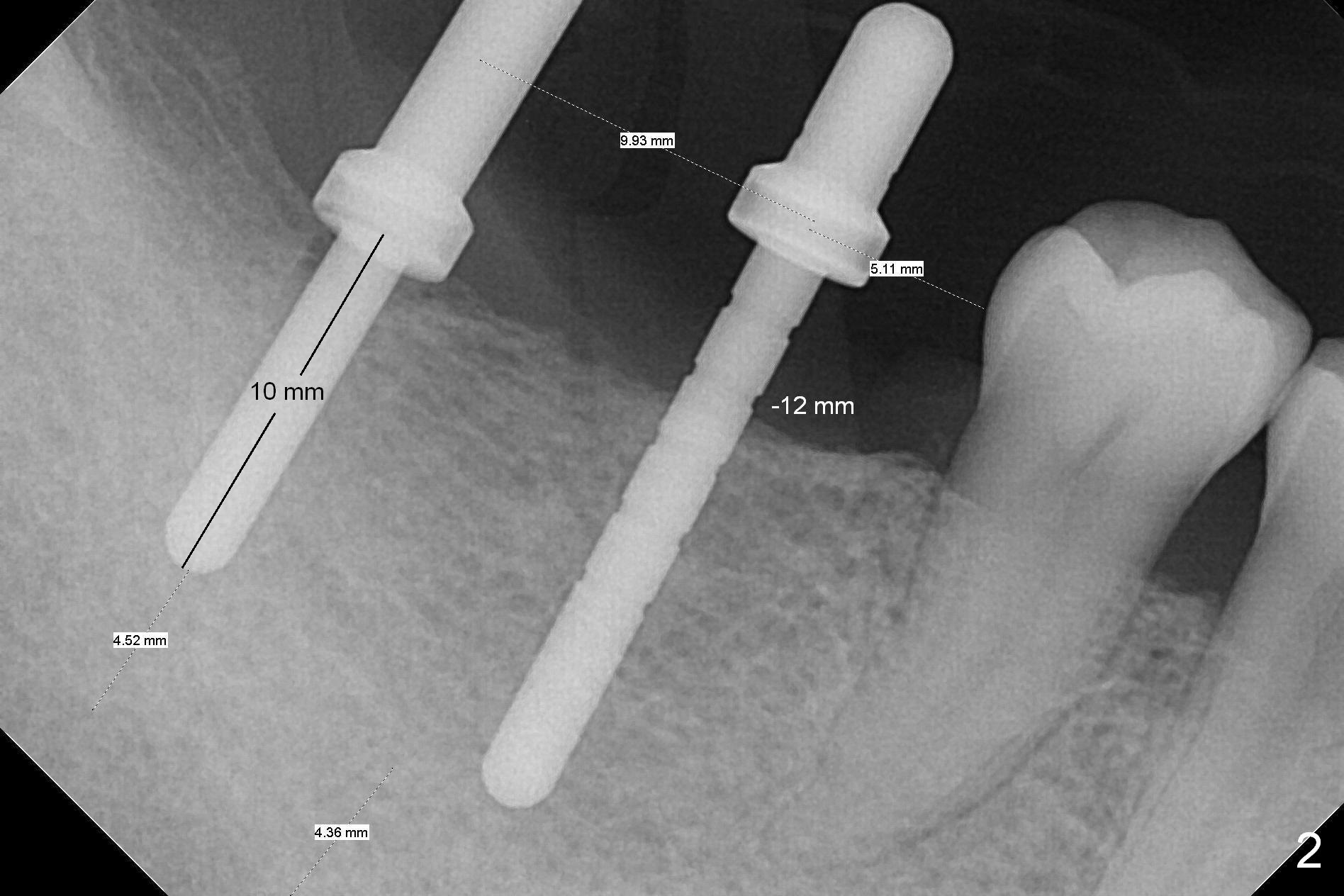
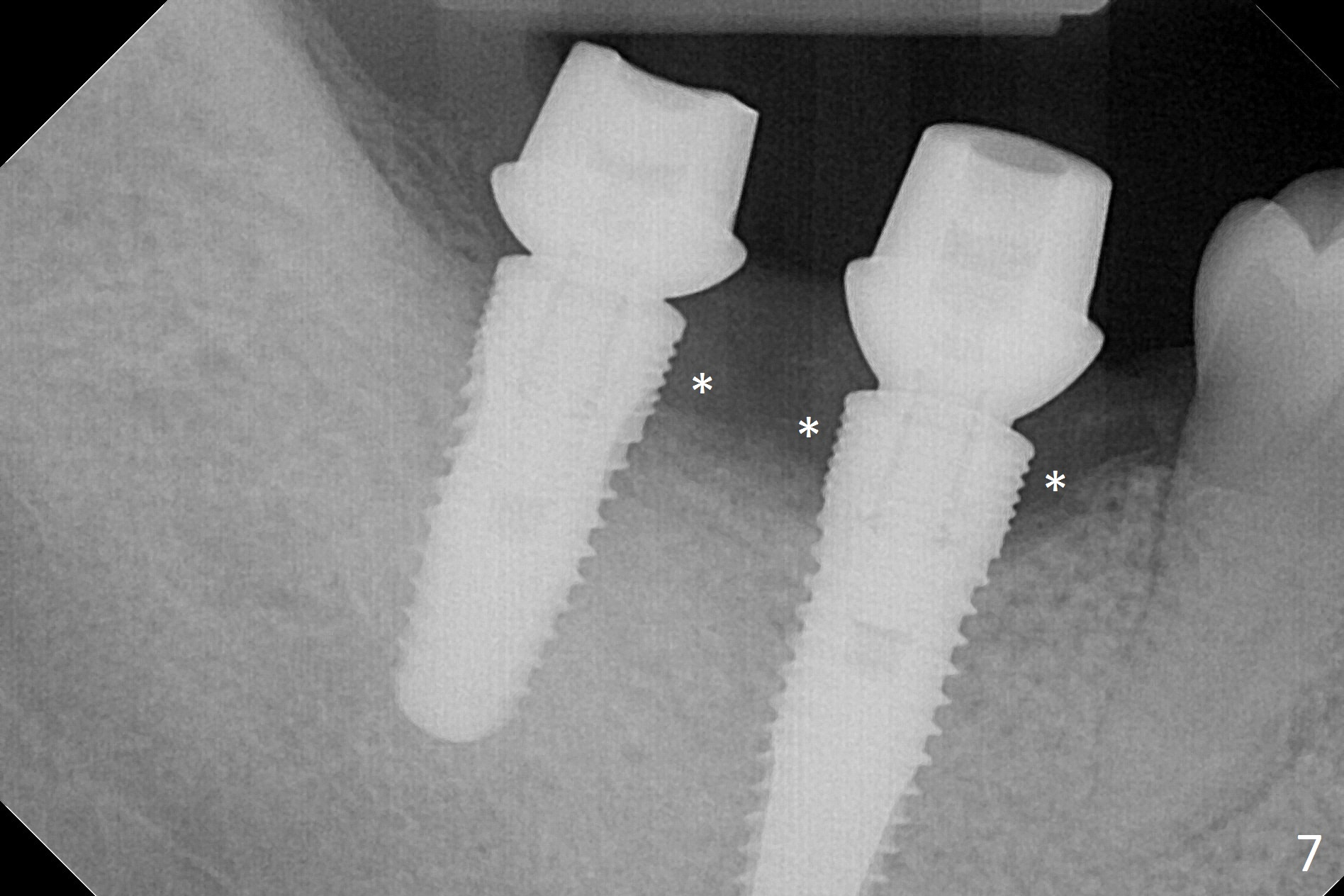
The supraerupted tooth #2 is adjusted using the lower right surgical stent. Osteotomies are initiated by using starter drill through surgical stent over the ridge (Fig.1) prior to incision. The initial depths are 10 and 12 mm at the sites of #31 and 30, respectively (Fig.2). The new sensor with the existing sensor holder cannot reach the deep portion of the lingual vestibule (Fig.2,3). Without the sensor holder, the #2 sensor with rounded corners has no problem showing the Inferior Alveolar Canal (Fig.4 red dashed line). The two implants (5x12 and 5x14 mm, Fig.5) are placed with >50 Ncm. Cemented abutments are immediately placed (6.8x4(2) and 6.8x4(3) mm) to reduce suture tension (after autogenous bone graft and collagen dressing) and hold periodontal dressing in place. The wound does not heal completely 15 days postop (Fig.6). The patient reveals that he smokes 1/2 pack per day. There is crestal bone resorption 4 months postop (Fig.7 *). It appears that for smokers, implants should be smaller, placed deeper and buried. In addition, his oral hygiene is not good.
Return to
Lower
Molar Immediate Implant, IBS,
Systemic Diseases
Xin Wei, DDS, PhD, MS 1st edition 12/13/2016, last revision 04/15/2017