

,%205.3x14,%205.8x7(4.5).jpg)
|
|
|
|
|
|
|
|
|
|
Rewarding
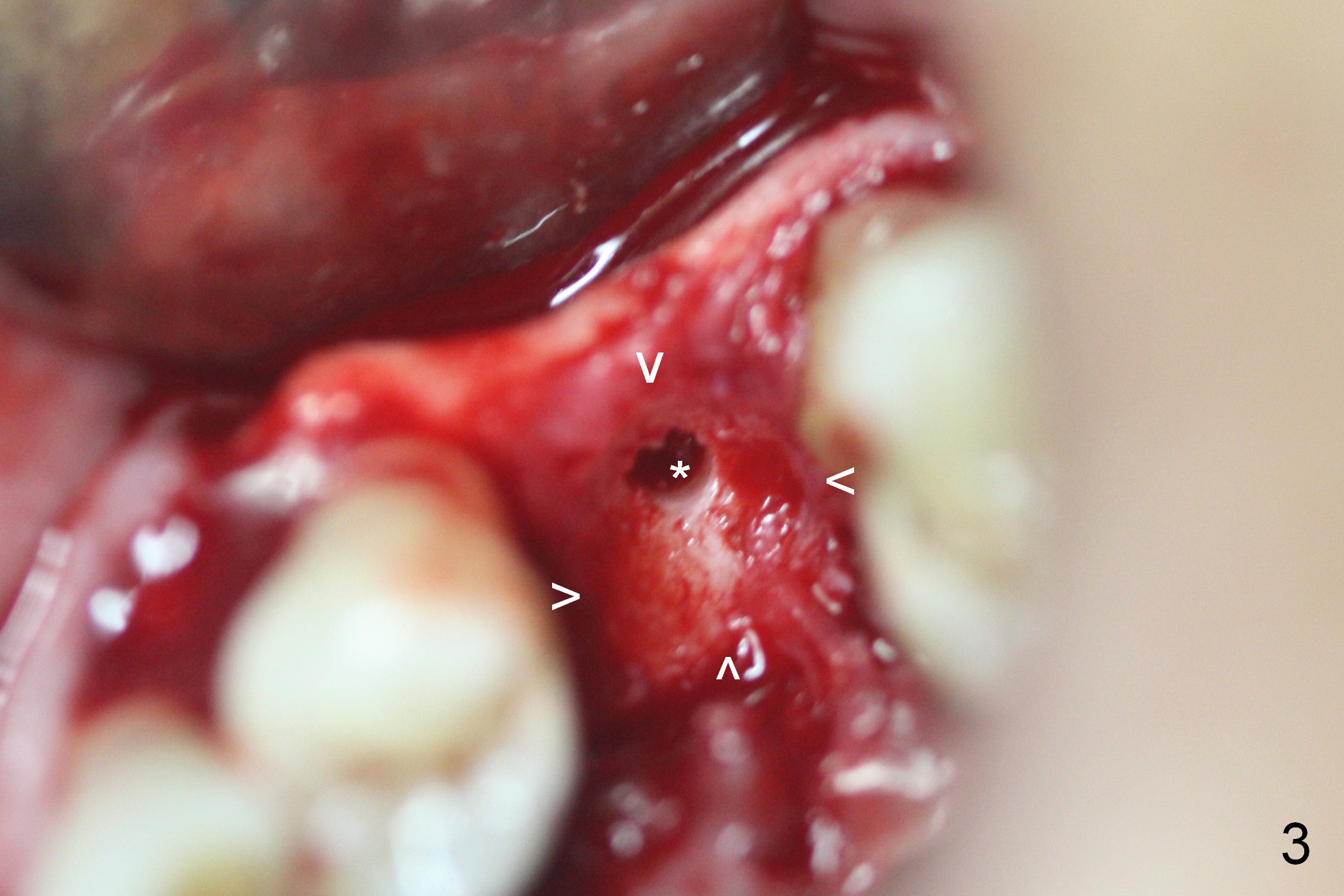
While the residual root at #13 is associated with purulent discharge, the palatal gingival recession of the tooth #14 is excessive (Fig.1). When the erythematous gingiva (Fig.1 *) is pressed, purulent discharge is from the sulcus (Fig.2 *). As planned, osteotomy is initiated first at #13 after extraction (Fig.3 *). Note the shallow socket (arrowheads). Later the osteotomy is moved more palatal.
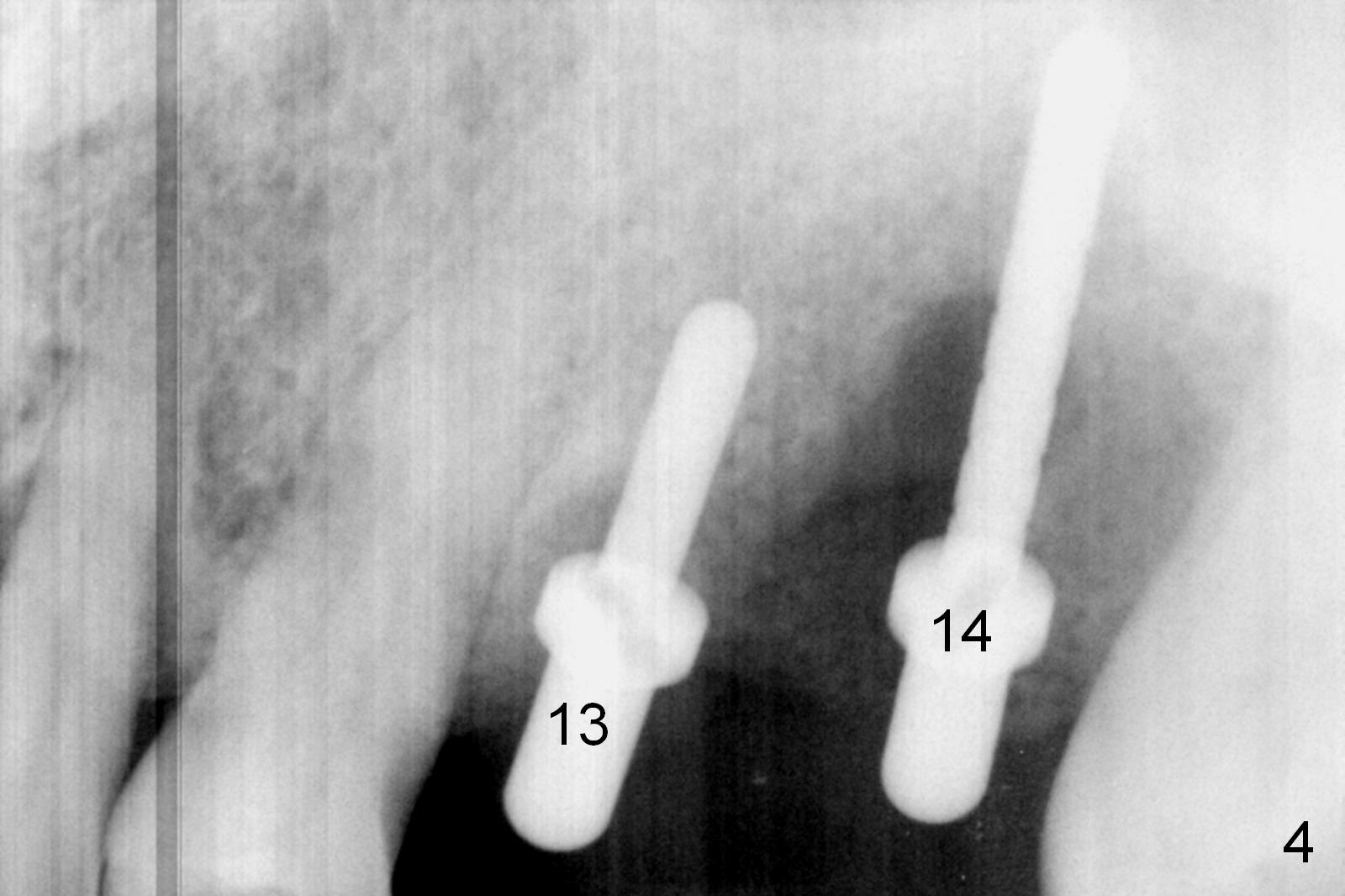
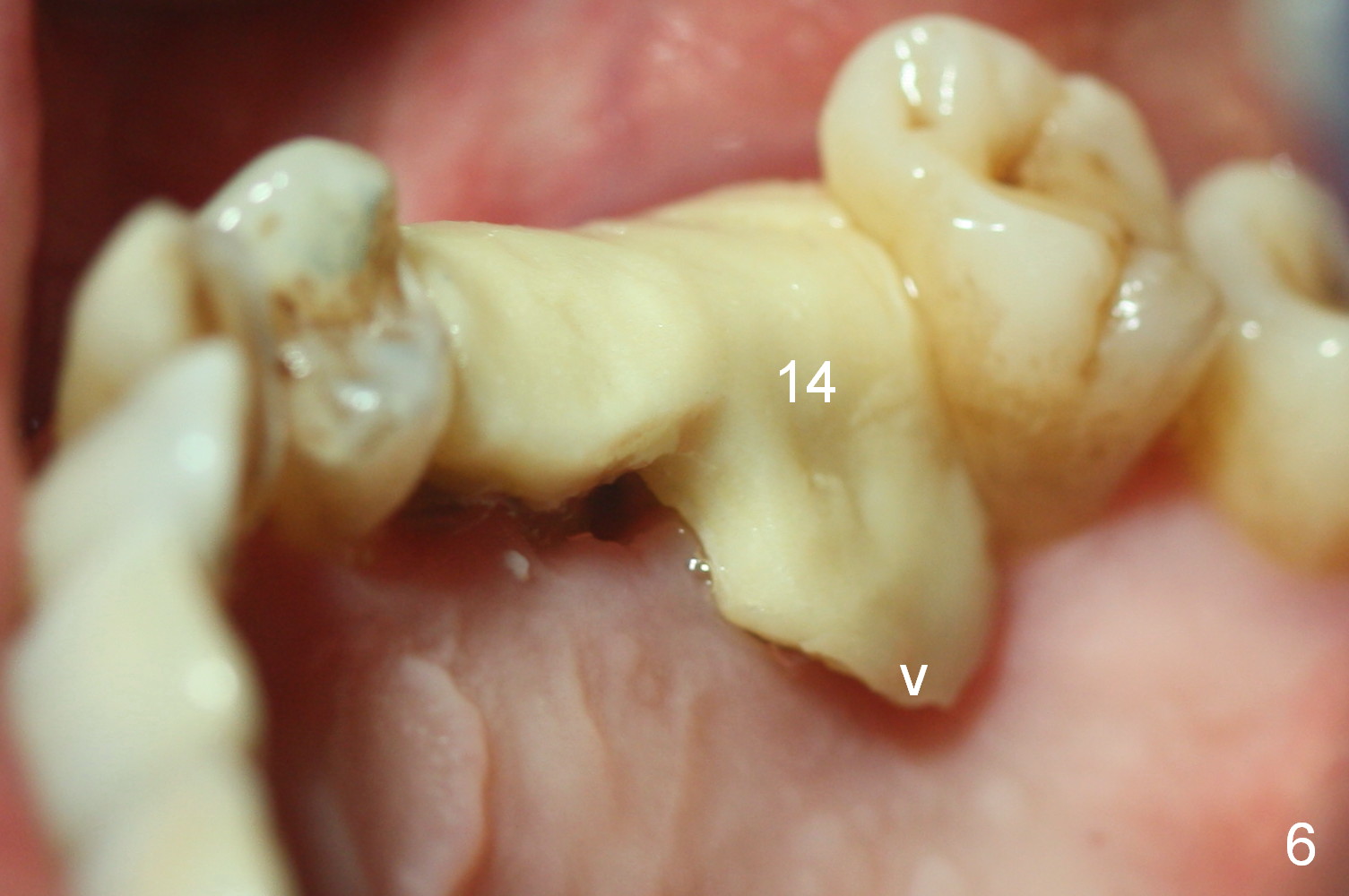
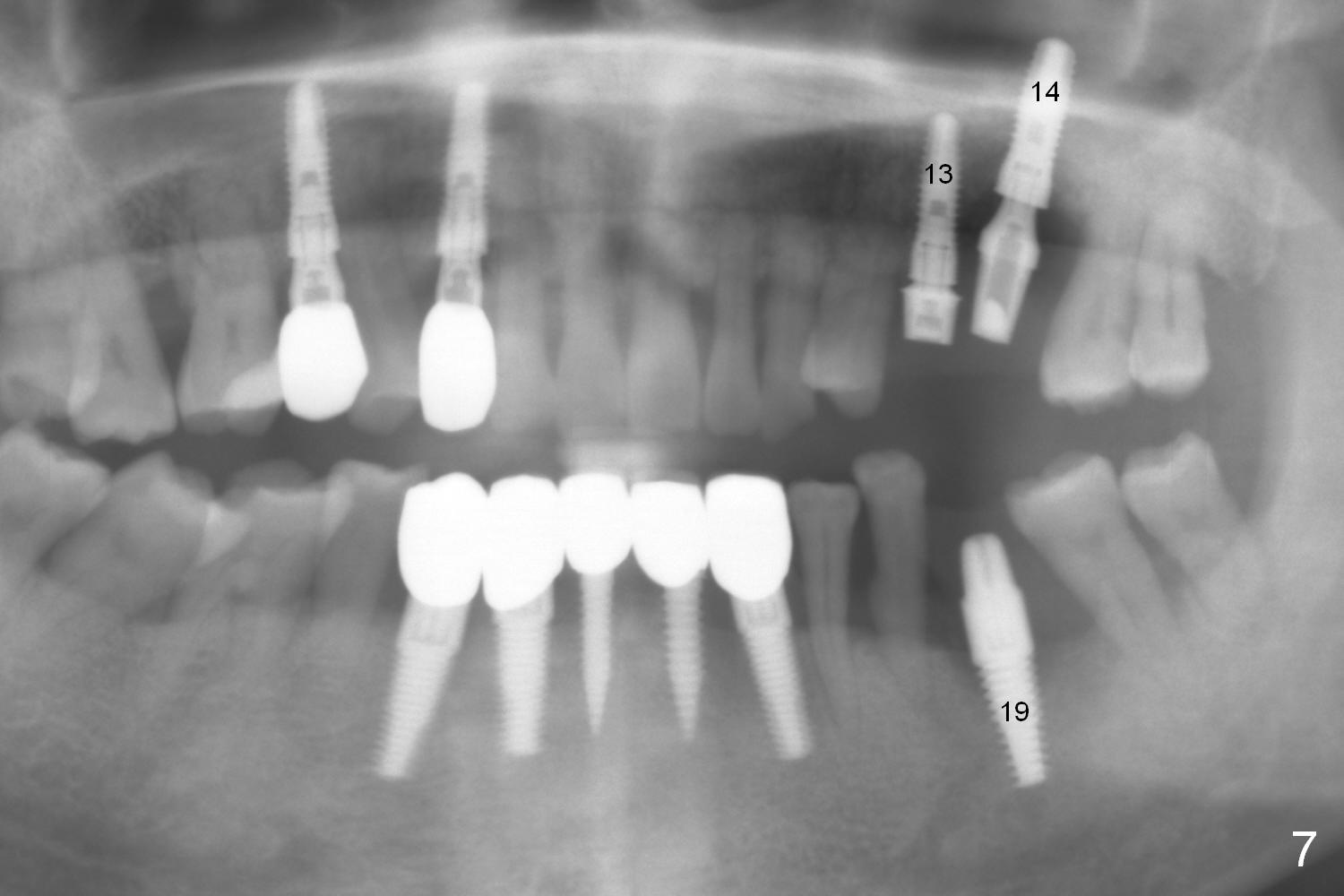
When the tooth #14 is removed, the granulation tissue in the palatal socket is so thick that scissors have to be used for removal. There is significant difference in bone height buccally vs. palatally. The 5.3x14 mm implant at #14 is placed ~ 6 mm apical to the buccal crest, ~2 mm coronal to the palatal crest, while the 4.5x14 mm one at #13 ~ 1 mm apical to the buccal plate, ~ 1 mm coronal to the distopalatal bone. The bone discrepancy is corrected by placing mixture of autogenous bone, allograft (.5-1 mm and 1-2 mm) and Osteogen. The crestal bone buccal to the site of #14 is removed with Rongeur ~2 mm. The palatal soft tissue deficiency is alleviated by placement of 6 month collagen membrane and collagen plug. Finding appropriate cemented abutments is also challenging (5.8x4(1) and 5.8x7(4.5) mm). Pain control is poor. Maxillary nerve block has been done. The patient is not cooperative, complaining that the tooth #14 should not be extracted. The sockets are oozing. It is the first time that I have realized that I actually hate dentistry, including implant. There is no clue how I can handle the rest of my life until I see that bone graft fills in the bony defect in Fig.5 (compare to Fig.4). Splinted immediate provisional is fabricated to close the large socket of #14, especially palatally. Two months later, the palatal margin of the provisional looks long (Fig.6 arrowhead). It is adjusted. Six months postop, the patient returns for definitive restoration (Fig.7). The cuff of the abutment at #13 looks short, while an angled abutment is needed at #14.
On Jul 18, 2016, #13,14 abutments were changed to 5.8x4(2) and 5.8x5.5(6), with laser gingivectomy. Temporary crowns were remade for 13,14,19. NV: #14 abutment changes to angled abutment or 5.8x7(6). #19 unipost needs resin bonding and heavy retention groove prep.
Return to Upper Molar, Lower Arch Immediate Implant,
Berkeley
Xin Wei, DDS, PhD, MS 1st edition 01/26/2016, last revision 09/02/2016