



|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
Proximity to Neighboring Root
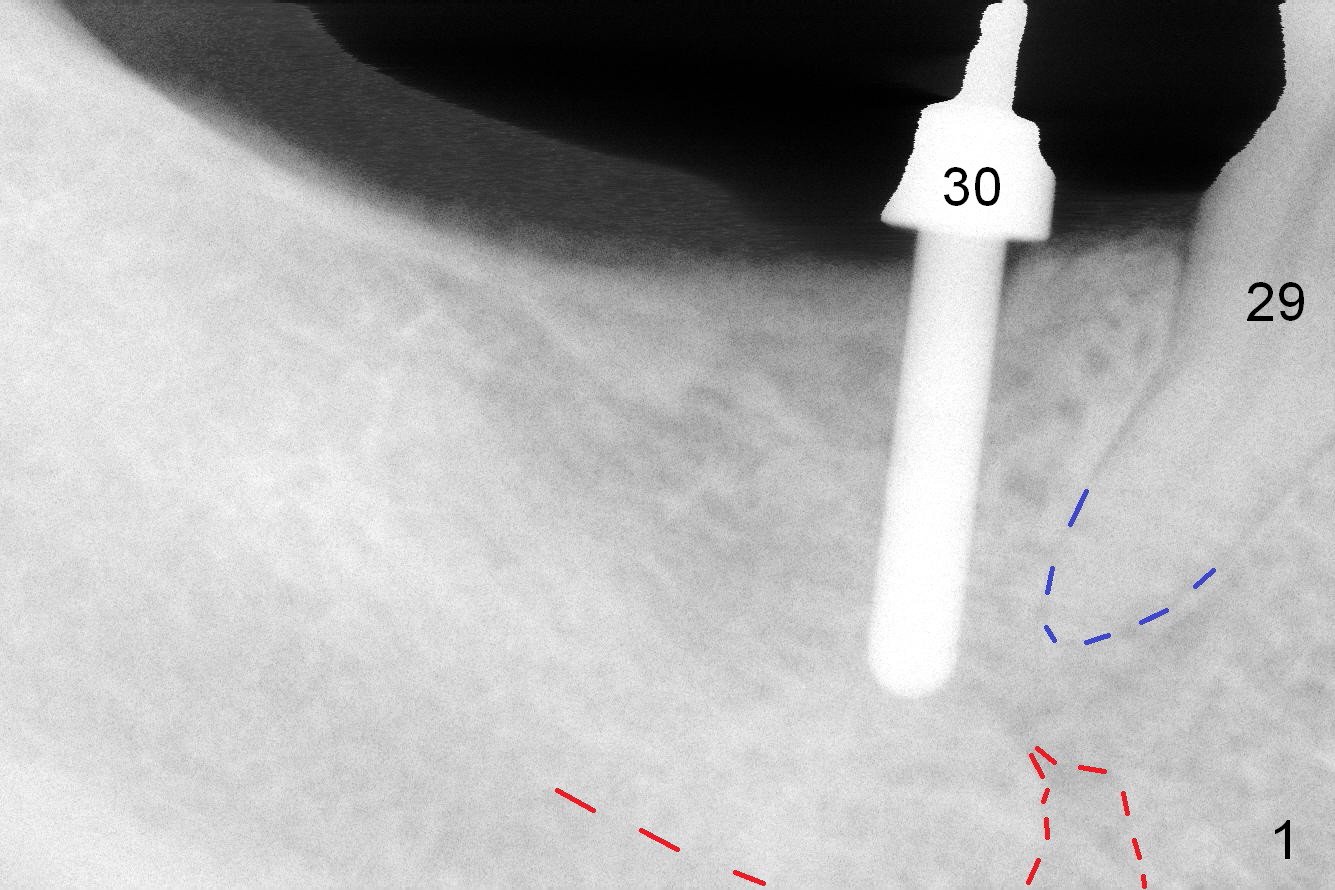
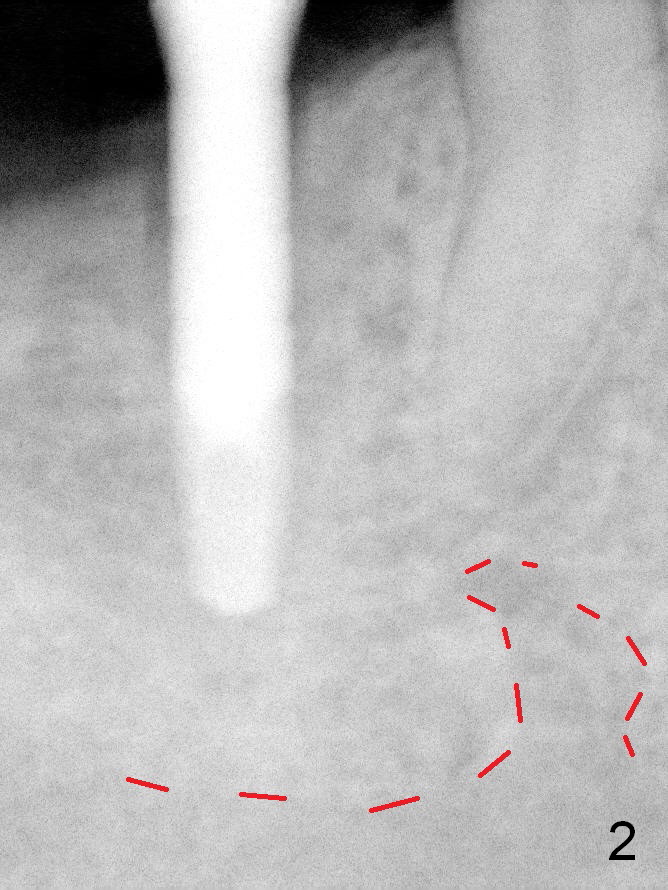
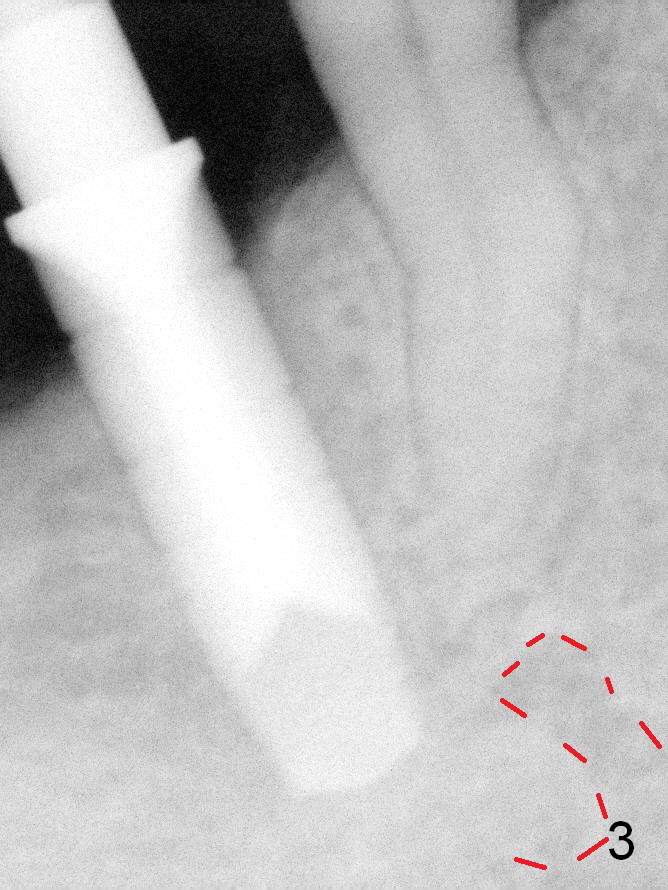
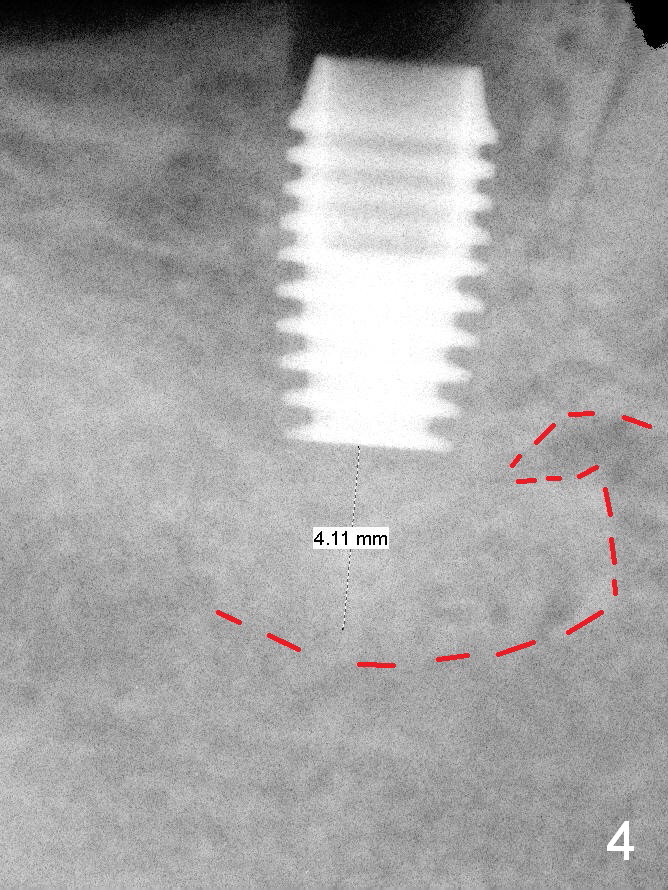
Since the edentulous ridge at #30 has a narrow zone of keratinized gingiva, a surgical stent cannot be used to start osteotomy prior to incision. Use the crown of the neighboring tooth and 4 mm implant spacer to initiate osteotomy free hand, buccal to the crest. Once a 2 mm pilot drill reach the depth of 11 mm, insert a parallel pin and the surgical stent to check the position and trajectory of the osteotomy (Fig.1). It seems that the osteotomy is close to the root of the neighboring tooth (blue dashed line (red dashed line: the superior border of the Inferior Alveolar Canal and the Mental Loop). A Lindamann bur is used to move the osteotomy slightly distally. Then lean the upper end of the 2 mm pilot drill slighly mesially. When the osteotomy increases until 3.5 mm reamer, the osteotomy is not so close to the neighboring root (Fig.2). One more PA is taken with 4.5 mm reamer in place (Fig.3) prior to insertion of 4.5x8 mm Bicon Implant (Fig.4). A 5x4.5 mm temporary abutment is placed. Autogenous bone harvested during osteotomy is placed in the buccal defect, covered with 6-month collagen membrane. The wound is closed with 4-0 Chromic gut suture. Periodontal dressing is applied.
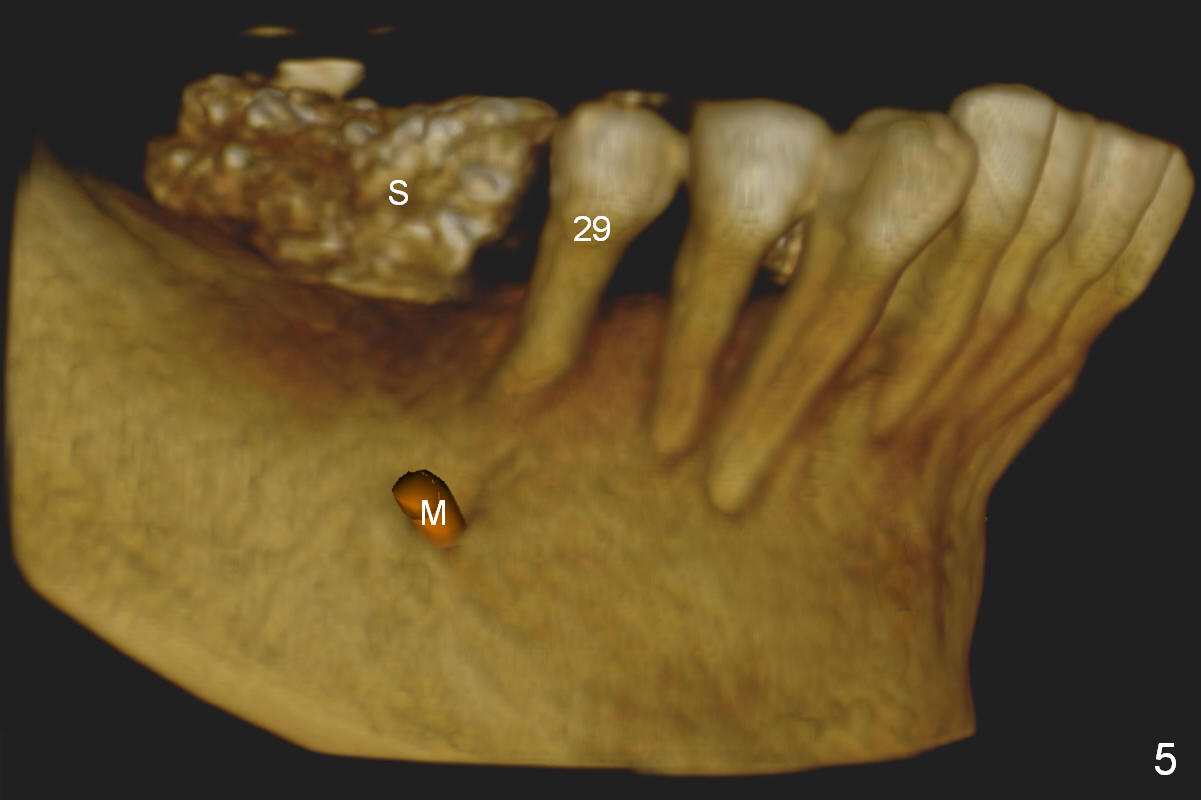
CBCT is reviewed postop (Fig.5). Root curvature of the tooth #29 and proximity of osteotomy at #30 to the Mental Loop are striking (S: CT scan stent). But these two pieces of information do not receive proper attention preop. The first pilot drill may cause injury to the neighboring root and the nerve if the depth or the trajectory is not properly controlled.
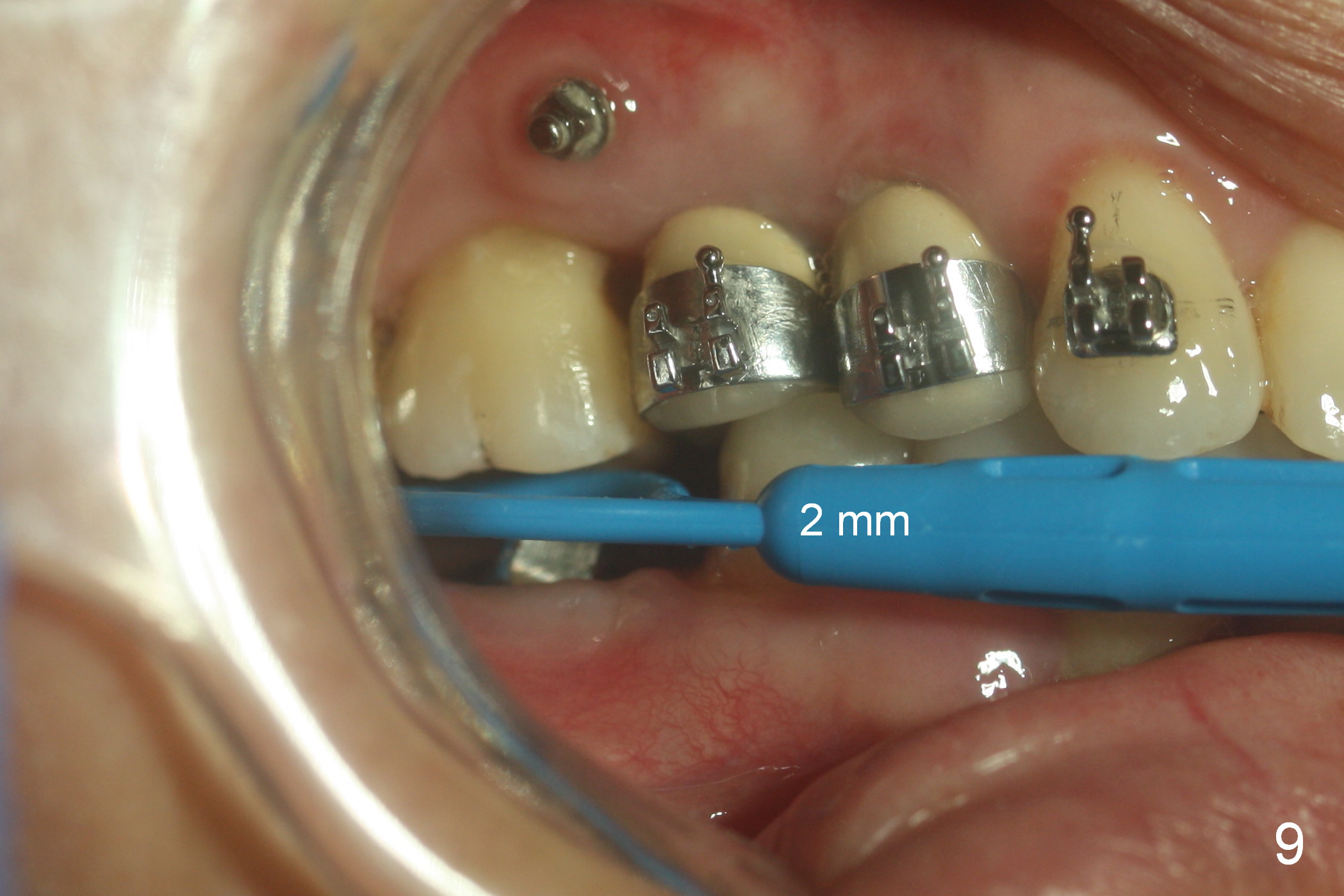
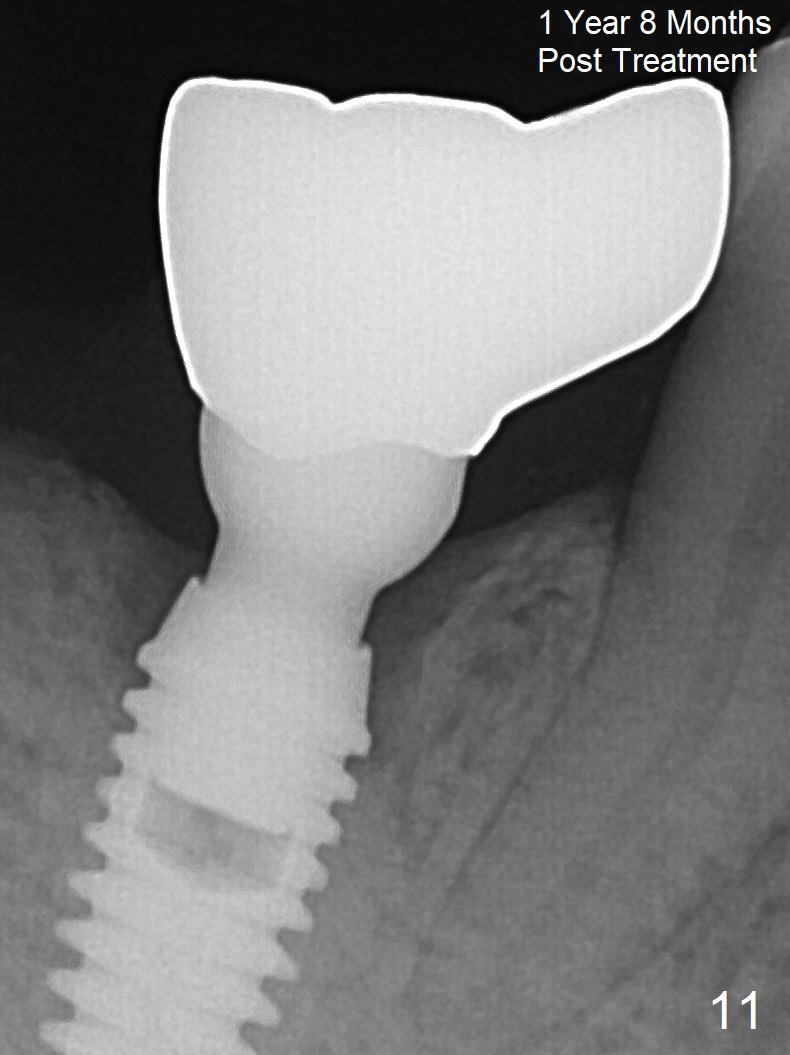
There appears to be osteointegration 2.5 months postop (Fig.6). Nearly 3 months postop, a provisional is fabricated slightly supraocclusal (Fig.7 #30) to intrude the supraerupted tooth (#3). The opposing tooth seems to have been intruded 2.5 months later (Fig.8). The clearance is more than 2 mm (Fig.9). A longer abutment is used for definitive restoration. Panoramic X-ray is taken 1 week post cementation (Fig.10). In the middle of mini-implant-assisted and orthodontic intrusion, we mutually agreed to work on #3 only. It appears that intrusion of both #2 and 3 is difficult.
Return to Lower Arch
Reconstruction,
Implant & Ortho
2
18-20
Xin Wei, DDS, PhD, MS 1st edition 03/15/2016, last revision
05/29/2018